







see also: Case Example Parotid Lipoma-like Liposarcoma
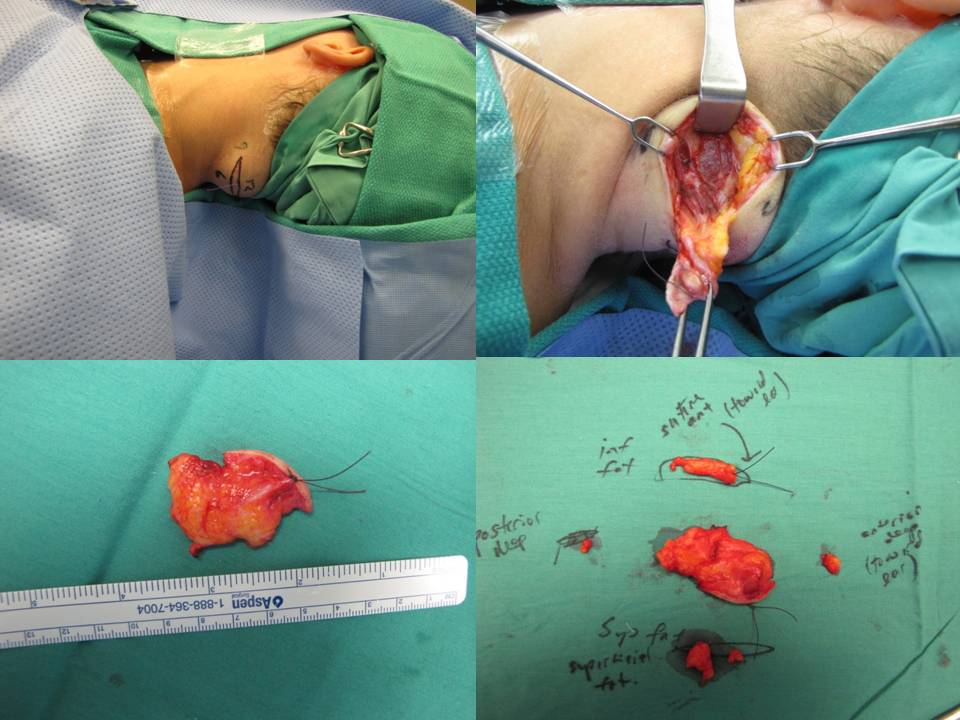
Positioning for posterior neck lesion resection |
|
|---|---|
 |
 |
 |
 |
 |
 |
 |
 |
|
3 month follow-up |
3 month follow-up |
 |
|
|
8 month follow-up |
|
Modified Operative Note
Procedure: Resection of posterior upper neck 5 cm mass (culture sent of cystic fluid from center)
Complex multilayered closure with placement of #7 fully perforated Jackson Pratt drain
Procedure Details
The operative techniques, indications, and risks versus benefits and alternatives to surgery were discussed with the patient, and informed consent was obtained. The patient was brought back to main operating and laid in a supine position on an operative table where a 'bean bag' had been appropriately placed. She was mask ventilated while placed under general anesthetic, and an uncomplicated intubation was performed by our colleagues in Anesthesiology with a 6.5 ET tube. A multidisciplinary timeout was performed. The operating table was turned approximately 120 degrees away from the Anesthesiology unit. The operating table headrest was replaced with the Mayfield, and the patient was placed into a "park bench" position with appropriate cushioning and molding of the 'bean bag' to cradle her in a semi-lateral position. She was prepped and draped in standard sterile fashion. Attention was turned to the posterior neck mass. An ellipse of skin was incorporated into our 5-cm planned incision site. An orientation stitch at 12 o'clock was placed with 12 o'clock being cephalad. A #15 blade was used to incise down through the dermis. The ellipse of skin was grasped, and sharp dissection around the mass ensued. We stayed above the level of the underlying muscle. The mass was elevated away from soft tissue attachments and removed with care to obtain appropriate margins. We then obtained additional specimens of adipose tissue from the superior and inferior borders of the dissection plane. Attention was turned to hemostasis, and this was achieved, using bipolar cautery. A 7-mm, fully perforated Jackson-Pratt drain was placed into the wound and secured to the skin, using 3-0 Ethilon suture. We then turned our attention to complex, multilayered closure, using 3-0 Vicryl, deeply to obliterate dead space. The superficial layers of the skin were closed, using 5-0 Prolene in a running fashion at the medial and lateral aspects of the wound and simple interrupted in the central aspect of the incision. Bacitracin was applied to the wound, and the drain tubing was secured to the shoulder, using benzoin and cloth and plastic tape. The patient was turned back over to Anesthesiology and ultimately extubated in the operating room and taken back to recovery in stable condition.
Final pathology: apocrine cystadenoma with all margins free.