












return to: Reconstructive Procedures Protocols
see also: Lip Melanoma Resection with W-plasty and Sentinel Node Biopsy Case Example with sample op note
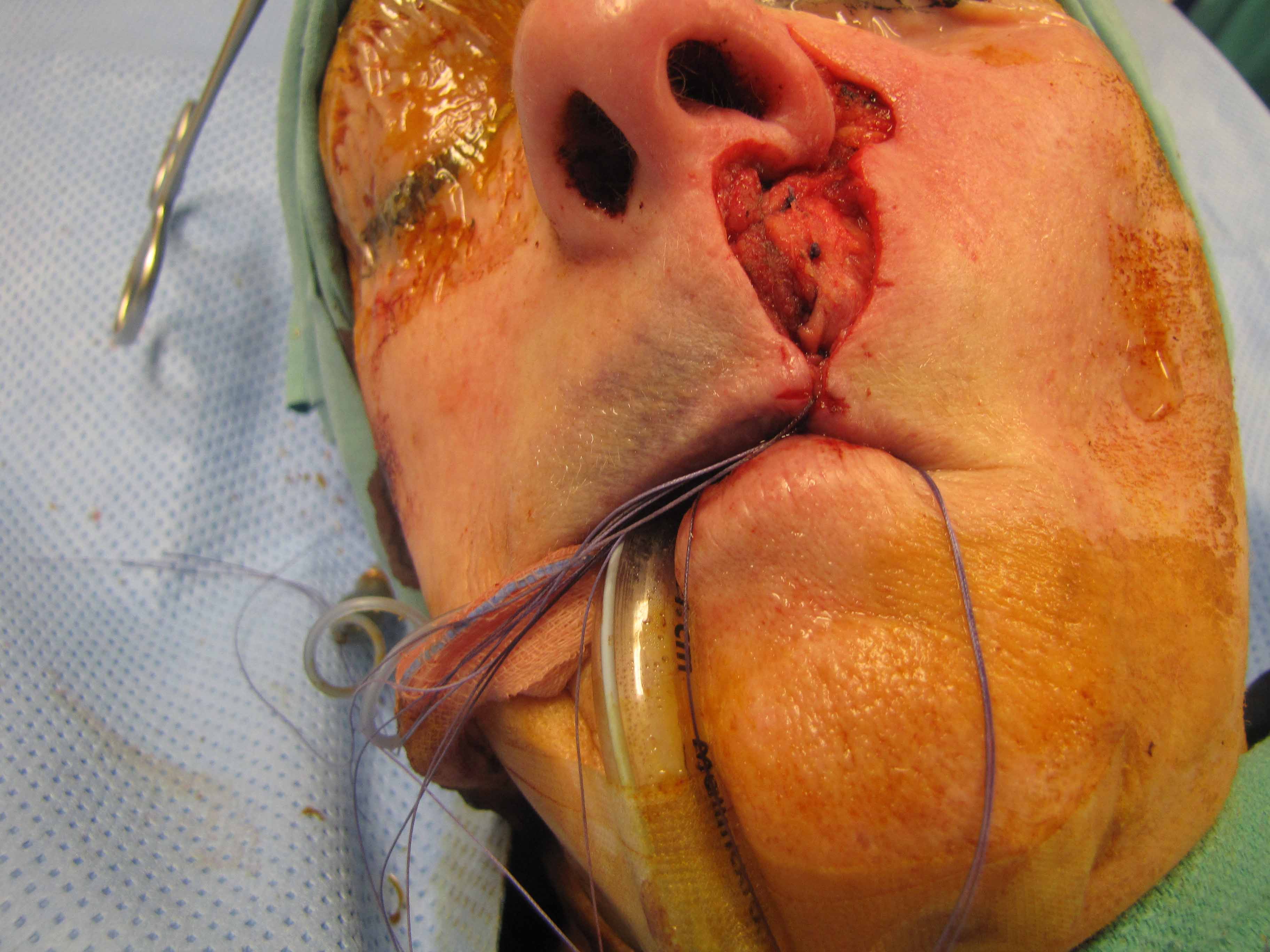
Case Example
S/P "Moat" Procedure for lentigo maligna surrounding invasive melanoma
- Moat Procedure: refers to circumferential clearance of margins by Mohs procedure to ensure adequate peripheral margins - like a "moat around castle" (see references below re: margins for melanoma in situ and 'square' procedure).
Brief Case History
Patient presented with what she thought was “just an age spot” on her left upper lip that developed about 1 year ago, and noticed it starting to get darker about 6 months ago. The lesion was diagnosed via biopsy as melanoma of the upper lip (immediately above the vermilion).
Sample Operative Note
After obtaining an informed consent, patient was laid supine and intubated after anesthesia was induced intravenously. A time-out was performed and the operating table was rotated 180 degrees. A Betadine prep of the oral cavity and head and were performed.
Margins for resection were surgically determined by Dermatology with Mohs resection. Bovie cautery was used for deep dissection and removal of the specimen at the level of the muscle, deepest at the central area of the tumor and tapering towards the edges. The specimen was marked with 12, 3, 6, 9 o’clock positions with a suture placed at the 12 o’clock position.
Plans for closure were placed with sutures and primary closure with a peri-alar crescentic flap was outlined, followed by a lateral wide undermining. Multiple sutures were laid in place to assure for good tension-free closure.
The lateral nasal excised skin was sent for Pathology. A deep muscular specimen was sent for a deep margin and to debulk the upper lip in order to allow for issue advancement. Deep 3-0 Vicryl sutures and intermediate Monocryl sutures were used intermittently. The skin was then closed using 6-0 nylon in both interrupted and vertical mattress form. There was no dead space due to imbricating sutures. The patient was extubated in the operating room and transferred to the PACU in stable condition.
Review
Reconstruction of the lip, a cosmetically sensitive area, often requires elaborate procedures due to the difficulty of reestablishing its complex symmetry and anatomic landmarks after resection. The peri-alar crescentic advancement flap was first introduced by Webster for repair of large defects that could not be approached using a linear ellipse closure, which inevitably creates an ablation of the natural alar crease and the nasolabial fold. (Webster, 1955) Incisions for the peri-alar crescentic advancement flap are placed more fully within the alar fold in comparison to earlier techniques, and include a removal of U-shaped areas of cheek tissue adjacent to the alae. Such modifications have allowed the prevention of visible scarring. (Spinelli, 2006)
The peri-alar crescentic advancement flap has become a widely used technique for the reconstruction of large, central defects of the upper cutaneous lip. The technique prevents deformity of the alar base, the lip, and the oral commissure by preserving and recreating the alar crease. (Wang, 2005) Depending on the location of the defect, the inferior portion of the final scar can be hidden within the nasolabial fold, the philtral column, or relaxed skin tension lines. The sphincteric integrity of the orbicularis oris muscle can be recreated with careful approximation during flap advancement. (Spinelli, 2006)
For reconstructions that require larger shifts, a wider ellipse of skin can be outlined on the paranasal area. Wider ellipse resections allow for longer outer edges of flap, thus providing more shifts of cheek into the lip. The cheek is then undermined until the skin can be advanced comfortably to close the defect without tension. (Jackson, 2002)
The peri-alar crescentic advancement flap is a simple and straightforward single-stage procedure with relatively low post-operative morbidity and patient inconvenience, providing satisfactory functional as well as aesthetic results.
Regarding treatment of Lentigo Maligna
Lentigo maligna (LM) and melanoma in situ, lentigo maligna type (MIS, LM type) are really two separate entities with different biological behavior and histology. The literature sometimes does not differentiate between the two, however, and most studies group the two. The rate of possible conversion to lentigo maligna type melanoma is usually a slow process and lesions can contain both LM and MIS, LM type. Original 1992 guidelines for MIS margins were 5-mm but this has proven to be inadequate and studies suggest that 5-mm margins are sufficient in less than 50% of cases, with more appropriate margins such as 9 to 15 mm resulting in greater than 94% clearance rates. Various techniques including "moat" or "square" help identify and clear the subclinical disease at the periphery and that associated with deep adnexal structures - the two reasons thought to bely the high recurrence rates found with inadequate margins.
Reference 9 below reviews various surgical techniques with a good overview of disease as well.
Square procedure (Johnson 1997)
The staged resection demonstrated in this case is an example of the "square" (or "moat") procedure, in which only the margin of the lesion is excised with a double-bladed scalpel. Like Mohs, this procedure theoretically provides visualization of 100% of the peripheral margin with precise mapping and tissue sparing. Because it leaves the center portion of the lesion for subsequent removal at the same time as the reconstructive procedure, it avoids creation of a large granulating wound, and the associated need for wound care, risk of infection, and potential difficulty with delayed reconstruction efforts.
References
Spinelli, H.M., Tabatabai, N., Muzaffar, A.R., et al. (2006). Upper lip reconstruction with the alar crescent flap: a new approach. Journal of Oral and Maxillofacial Surgeons, 64, 1566-1570.
Tirone, L., Moscatiello, F., & Molea, G. (2006) Case report: reconstruction of the upper lip and philtrum. Journal of Plastic, Reconstructive & Aesthetic Surgery, 59, 865-866.
Wang, S.Q., Behroozan, D.S., & Goldberg, L.H. (2005). Perialar crescentic advancement flap for upper cutaneous lip defects. Dermatolic Surgery, 31, 1445-1447.
Jackson, I.T. (2002). Local Flaps in Head and Neck Reconstruction. St. Louis, MO: Quality Medical Publishing.
Johnson TM, Headington JT, Baker SR, Lowe L. Usefulness of the staged excision for lentigo maligna and lentigo maligna melanoma: the "square procedure". J Am Acad Dermatol 1997 Nov; 37 (5 Pt 1): 758-64.
Demirci H, Johnson TM, Frueh BR, Musch DC, Fullen DR, and Nelson CC: Management of periocular cutaneous melanoma with a staged excision technqiue and permanent sections - the square procedure. Opthalmology 2008 Dec;115(12):2295-2300
Jejurikar SS, Borschel GH, Johnson TM, Lowe L and Brown DL: Immediate, optimal reconstruction of facial lentigo maligna and melanoma following total peripheral margin control. Plast Reconstr Surg. 2007 Oct;120(5):1249-55
Kunishige JH, Brodland DG, and Zitelli JA: Surgical margins for melanoma in situ. J Am Acad Dermatol 2012 Mar;66(3):438-44
Webster, J.P. (1955). Crescentic peri-alar cheek excision for upper lip flap advancement with a short history of upper lip repair. Plastic Reconstruction Surgery, 16, 434.
Blum A:The moat technique. A two-step surgical technique for extensive basal cell carcinomas of the lip Der Hautarzt 2004 vol:55 iss:9 pg:869-873
Surgical treatments for lentigo maligna: a review. Dermatologic surgery [1076-0512] McLeod, Michael yr:2011 vol:37 iss:9 pg:1210 -1228