






Click on image above to enlarge and advance with cursor over border
return to: Otology Neurotology Protocols
![]() CWR Tympmastoid-Iowa Protocols 3-18.pptx (click on link to download powerpoint presentation)
CWR Tympmastoid-Iowa Protocols 3-18.pptx (click on link to download powerpoint presentation)
General Considerations
- Reported indications
- Chronic otitis media with cholesteatoma in children and adults.
- We use this technique for most cholesteatomas as it provides visualization similar to a canal wall down tympanomastoidectomy to ensure total elimination of cholesteatoma that is far superior to traditional Canal Wall Up technique. This strategy also isolates the attic and mastoid from the tympanum preventing recurrent retraction of the tympanic membrane if the eustachian tube does not function properly.
- Reported contraindications
- Absolute:
- Severe mastoid cholesteatosis. If it is not possible to remove all cholesteatoma from the mastoid air cell tracts obliteration of the mastoid with bone pate is considered to be contraindicated. If cholesteatoma matrix cannot be completely removed for any reason, this technique is considered to be contraindicated.
- Previous Canal Wall Down procedure.
- Patient unwilling or unable to have second look procedure.
- Relative:
- Prior Damage (iatrogenic or disease related), excessive thinning or excessive lowering of posterior canal wall.
- Previous canal-wall-up tympanomastoidectomy may not be considered a contraindication for canal-wall reconstruction provided that the posterior canal wall is not lowered or too thinned.
- Absolute:
- Anatomic Considerations
- The Temporal bone consists of four parts fused together: The squamous, tympanic, mastoid and petrous bones.
- The subunits of the middle ear space include the Epitympanum, Protympanum, Mesotympanum and Hypotympanum
- Surgical Landmarks include the Tegmen Tympani, Zygomatic Root, Spine of Henle, Sigmoid sinus, Antrum, Fossa Incudis, Mastoid and Tympanic segments of Facial Nerve, Horizontal SCC, Facial Recess and Chorda Tympani, Sinus tympani (bordered by ponticulus and subiculum).
Note: Complete surgical anatomy is beyond the scope of this protocol and the authors would like to refer the reader to their temporal bone anatomy text of choice.
Preoperative Preparation
- Evaluation
- Complete history, focused on otologic symptoms, medical co-morbidities, medications, allergies
- Physical exam including otomicroscopic exam of ears with pneumotoscopy, Weber/Rinne tuning fork exam (256, 512, 1024 Hz), and documentation of facial nerve function (House-Brackmann Scale).
- Complete audiogram
- CT imaging is suggested in revision procedures. Radiographic imaging is not necessarily compulsory in all primary procedures, but should be considered if there is concern for complications associated with advanced cholesteatoma (i.e. labyrinthine fistula, sensorineural hearing loss, tegmen erosion/intracranial extension, facial weakness/spasm, or revision surgery).
- Consent
- Benefits :
- To remove all cholesteatoma from the middle ear and mastoid and provide a dry, safe ear
- with a lower recalcitrant rate than canal-wall-up
- no chronic care needs like the canal-wall-down.
- To provide for eventual hearing restoration, if possible
- To remove all cholesteatoma from the middle ear and mastoid and provide a dry, safe ear
- Alternatives:
- Canal wall up (CWU), down (CWD) procedures.
- An individual with a cholesteatoma is at significant risk for intracranial and other complications if they refuse surgical intervention in this disorder.
- Risks
- Bleeding
- Infection, including loss of reconstructed bony canal wall or exposure of bone in canal wall
- Facial paralysis - reported 0.6-3.6%
- Taste alterations from sacrifice of chorda tympani
- Deafness/sensorineural hearing loss
- Worse hearing (conductive loss) immediately after surgery is commonly due to ossicular discontinuity
- Vertigo - 5-10% of cholesteatomas form lateral semicircular canal fistula
- Recurrence of cholesteatoma - 1.5%
- Complications of general anesthesia including heart attack, stroke, and death
- Need for further surgeries, including a planned surgery for re-evaluation of the ear and possible reconstruction of ossicles (bones that transmit sound from the eardrum to inner ear).
- We do not do primary reconstruction at time of surgery
- Benefits :
Nursing Considerations (TBA)
Anesthesia Considerations
- Positioning
- Head of patient 180° from anesthesia
- Double check arms and legs padding to ensure safety. A "test roll" is performed after 3 sets of safety straps and padding in place
- Three straps
- Lower body BairHugger only, if Bairhugger desired by anesthesia personnel
- NIMS facial nerve monitor set up and tested according to manufacturer's instructions.
- Post-auricular hair shaved
- Towel roll under contralateral cheek to prevent hyperrotation and subluxation in pediatric/geriatric patients
- Medications
- Piperacillin-tazobactam 3.375 mg (or clindamycin 900mg IV) and levofloxacin 500mg 1 hour prior to surgical incision in adults.
- We are currently using Cipro 750 mg IV OCTOR as Levaquin has gone off-formulary at our institution. Levaquin would be the preferred med if available at your institution.
- Decadron 10 mg IV on call to operating room
- Advise the need for "no paralysis" during the case for facial nerve monitoring
- We recommend against the use of nitrous oxide because of tympanic membrane grafting
- Piperacillin-tazobactam 3.375 mg (or clindamycin 900mg IV) and levofloxacin 500mg 1 hour prior to surgical incision in adults.
Operative Procedure
-
A post-auricular incision is made down to the level of the superficial layer of the deep temporalis fascia.
-
An anteriorly based, wide musculoperiosteal Palva flap (approximately 4 × 4 cm) is created.
-
A bone pâté collector is used to collect bone pâté from the cortex of the mastoid and squamous temporal bone. Bone pâté collection stops before exposure of the mastoid air cells. Bacitracin solution is drawn through the bone pâté, and the pâté is set aside.
-
A complete cortical mastoidectomy is performed, including total exenteration of the sinodural angle and mastoid tip air cells. Cholesteatoma disease is removed in the standard fashion. The posterior canal wall bone is left relatively thicker than in typical CWU procedures. If a canal defect is noted greater than can be reconstructed with bone grafts or if the canal wall is lowered extensively, one must convert to a CWD procedure.
- The facial recess is opened and extended inferiorly to the level of the floor of the external auditory canal. The incus and head of the malleus are removed. The chorda tympani is sacrificed.
-
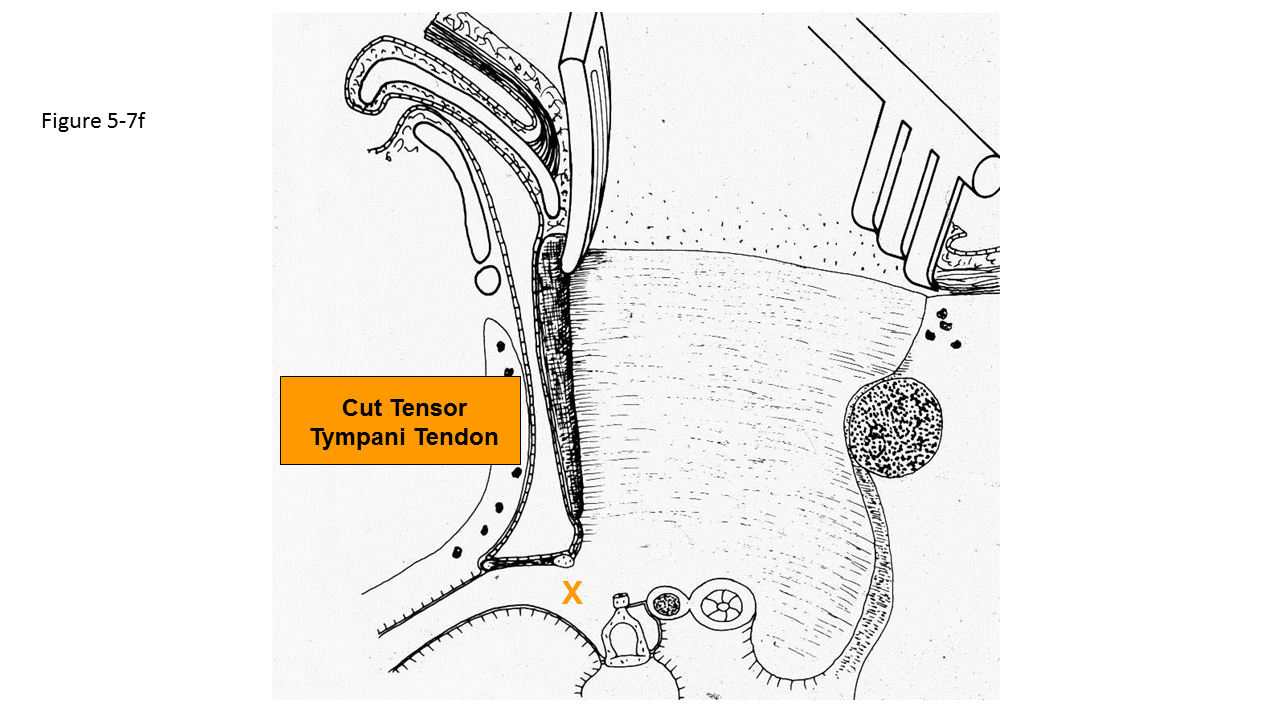
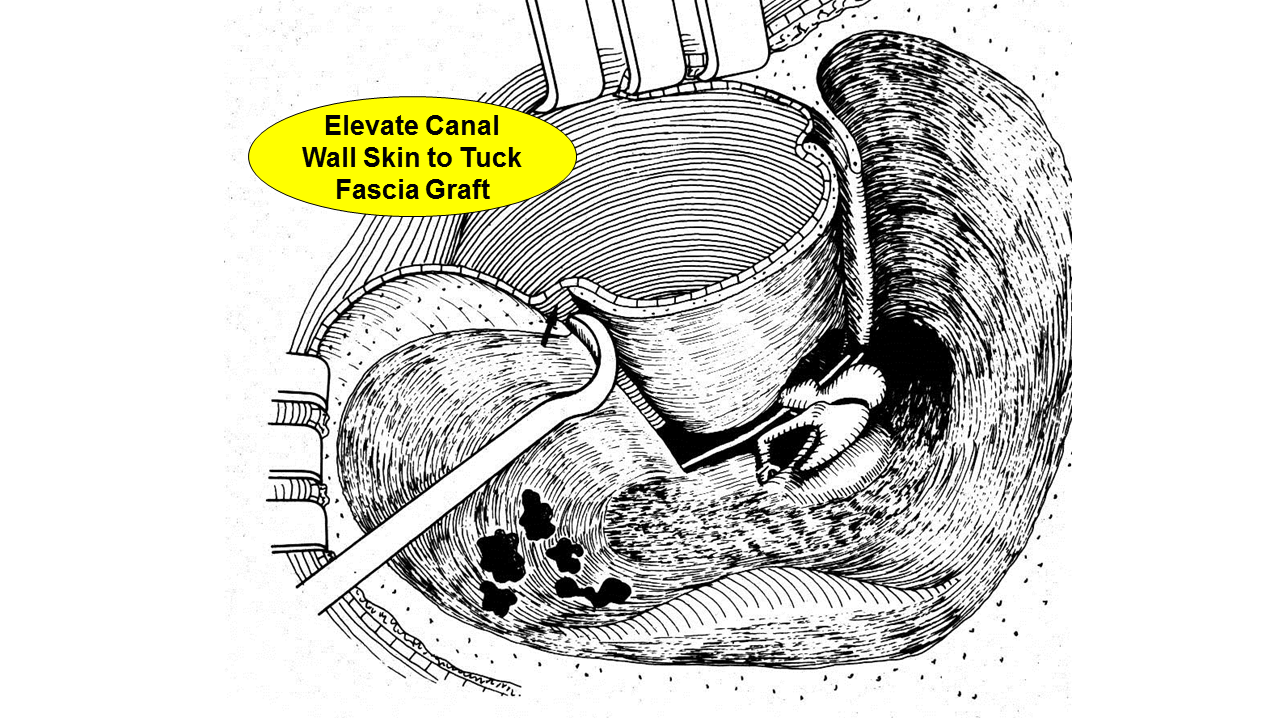
Working post-auricularly, the external canal skin is elevated off the posterior canal wall without making any incisions in the posterior canal wall skin. The annulus is elevated out of the annular sulcus to about 6:00. The tensor tympani tendon is transected, allowing exposure of the entire mesotympanum. Care is taken to raise the canal wall skin anteriorly to protect it from the posterior bony canal wall cuts.
-
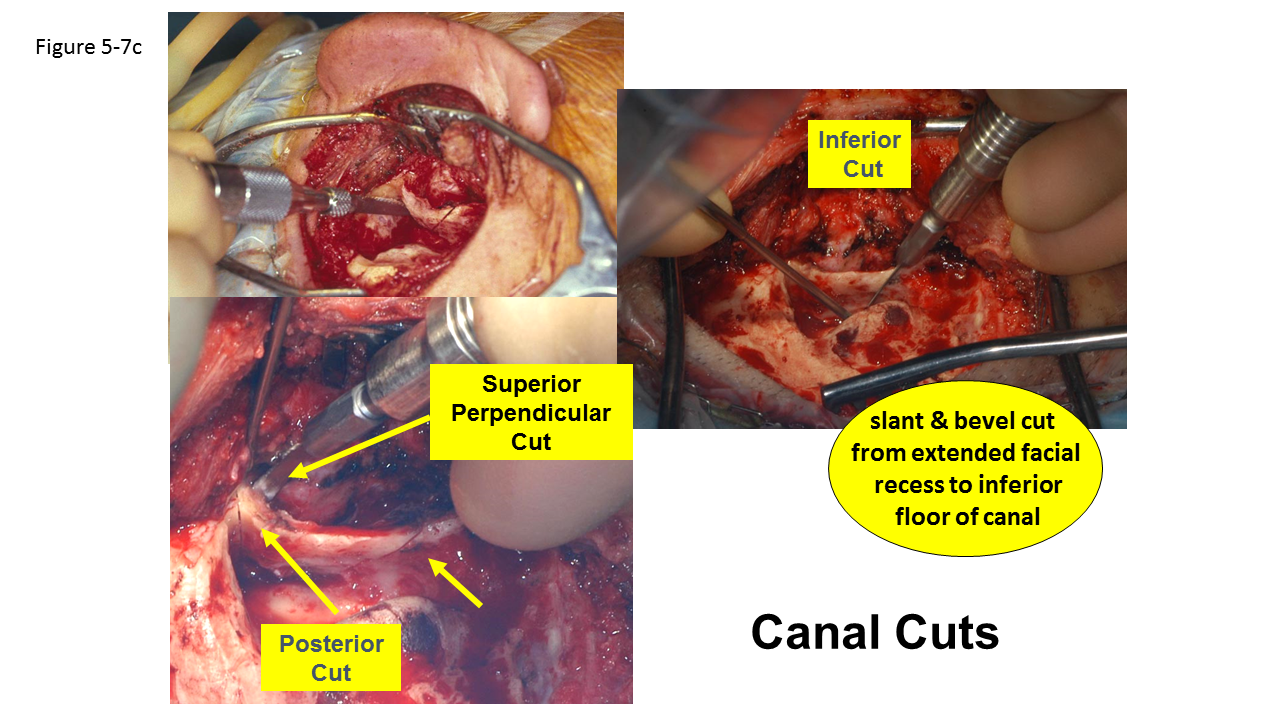
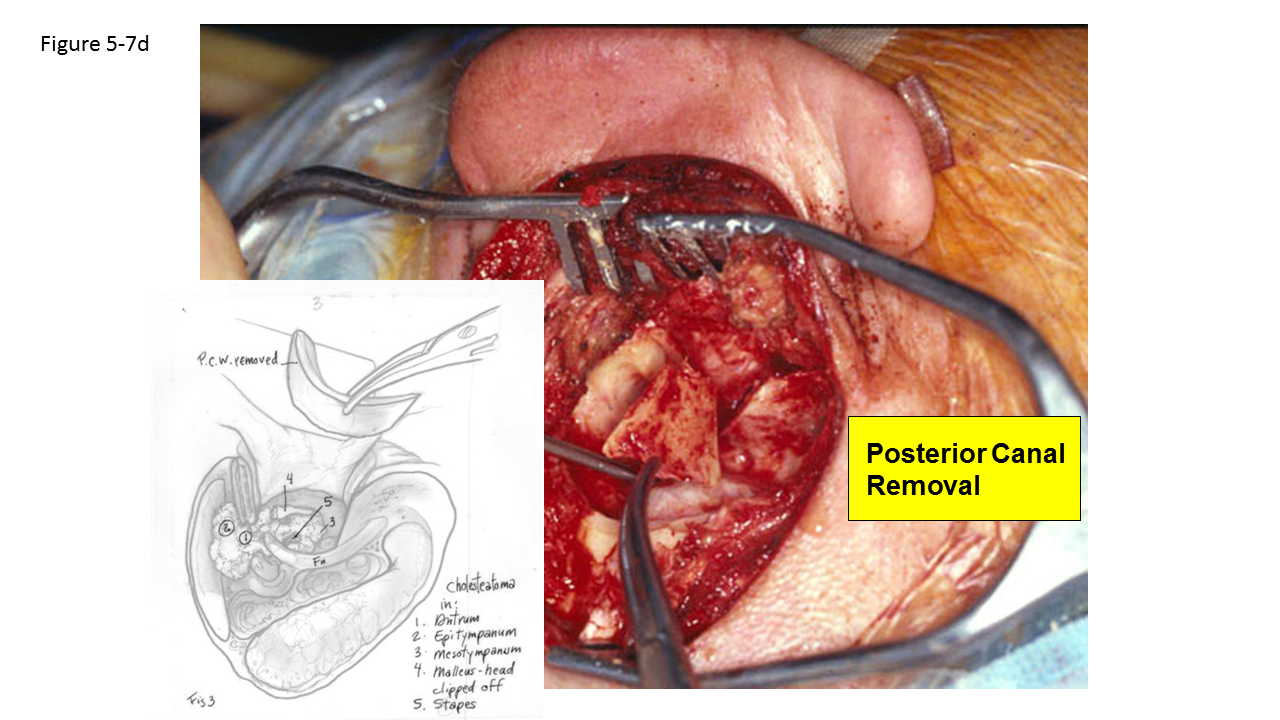
A microsagittal saw (Jed Med Bien Air, St Louis MO, or Anspach, Palm Beach Gardens, FL) is used to create superior and inferior cuts in the posterior canal wall. The cuts are performed in a locking, mitered fashion to help prevent collapse of the canal into the mastoid after reconstruction (see figure). The inferior cut extends from the inferior facial recess laterally, widening and beveling as a compound miter. Superiorly, two cuts are made. The first is parallel to the temporal lobe in a posterior to anterior direction. The second cut is perpendicular to the first, made from the external canal to meet the superior cut. The posterior canal wall segment is then removed and placed aside for future reconstruction.
Canal cuts should give the operative surgeon pause for caution. The inferior cut can damage the facial nerve inferiorly in the facial recess. The superior canal cut may lacerate the dura in a low-lying tegmen. Passing point with the saw superiorly may also endanger the geniculate ganglion. Another approach should be considered if the patient is known pre-operatively to have a low-lying tegmen.
INFERIOR CANAL CUT
SUPERIOR CANAL CUTS
POSTERIOR CANAL REMOVAL
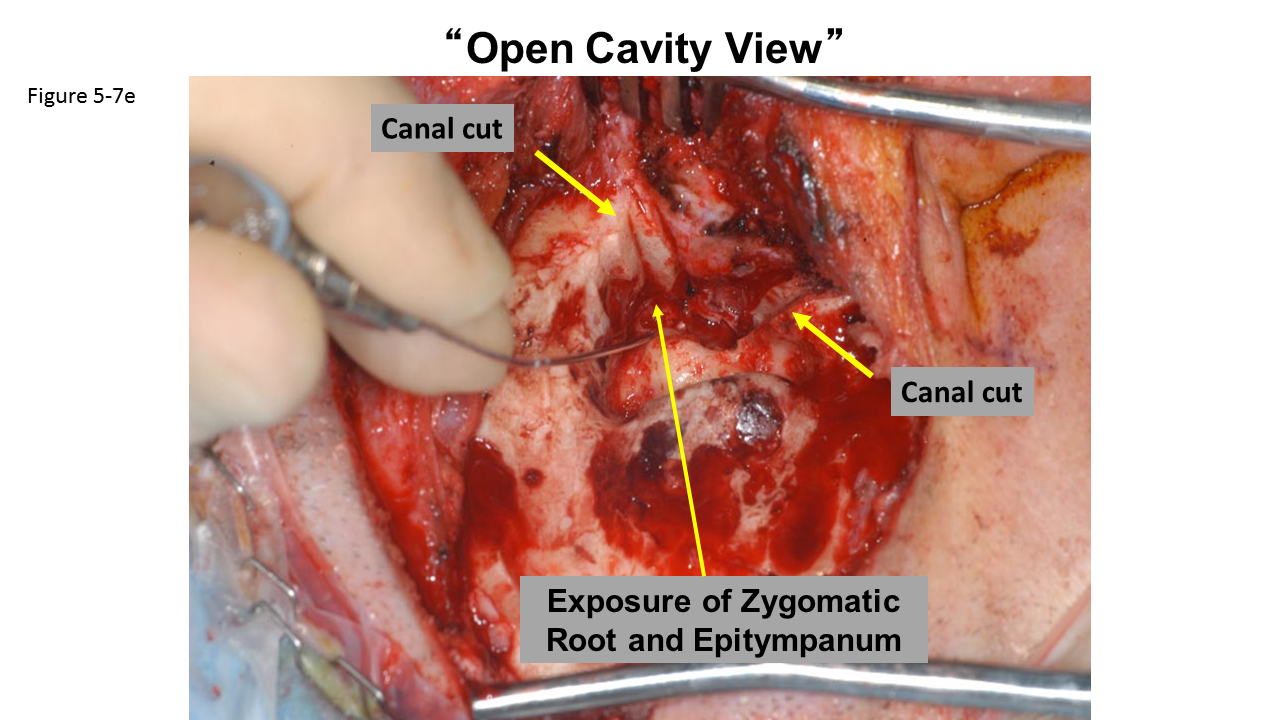
"OPEN CAVITY" VIEW
- Cholesteatoma may then be completely removed from the tympanic cavity, anterior attic, and mastoid. The canal wall piece needs to be carefully examined to ensure all cholesteatoma and squamous epithelium has been removed.
-
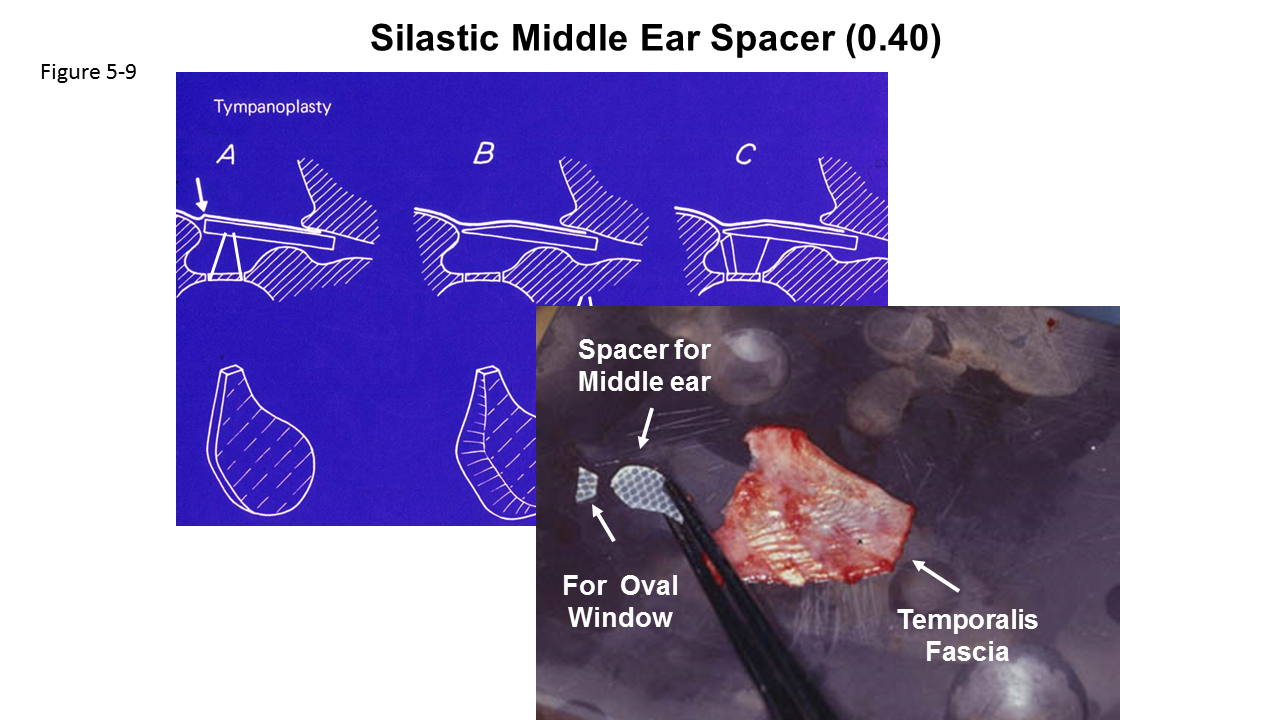
Reconstruction involves placing a ~1cm tear-drop piece of silastic sheeting (0.04 inch thickness) in the middle ear space. The taper of the silastic is placed in the eustachian tube orifice, with the remainder maintaining a middle ear space. If the stapes superstructure is present, the silastic is placed laterally and acts to transfer acoustic energy to the inner ear before second stage ossiculoplasty. If the superstructure is destroyed, a small wedge of silastic is placed between the footplate and the larger piece of silastic. This will maintain and identify the oval window and footplate for futher surgeries. Retraction of the reconstructed tympanic membrane and middle ear space contraction are complications of surgery if the silastic does not maintain the space.
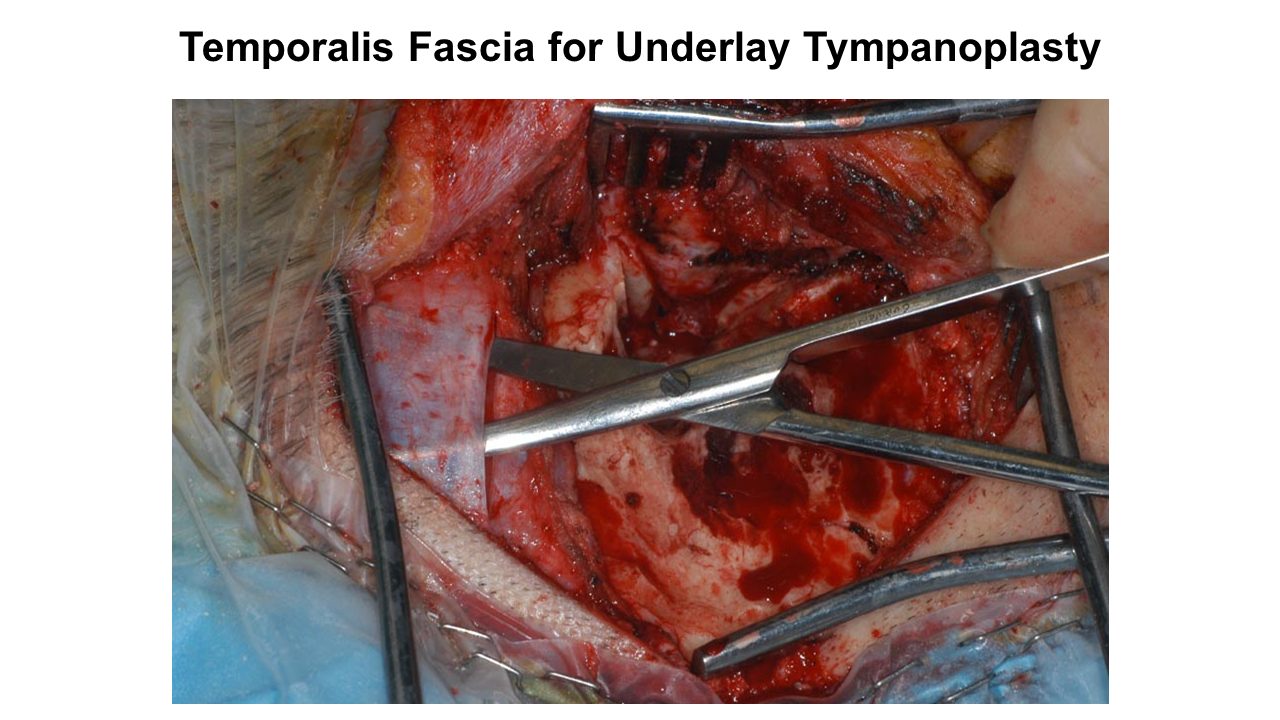
Temporalis fascia should be larger than posterior canal bone as it should cover the margins of the bone cuts.
- A generous temporalis fascia graft is harvested. This must be large enough to extend up the posterior canal wall, over the canal wall cuts, and is used in an underlay fashion to reconstruct the tympanic membrane.
-
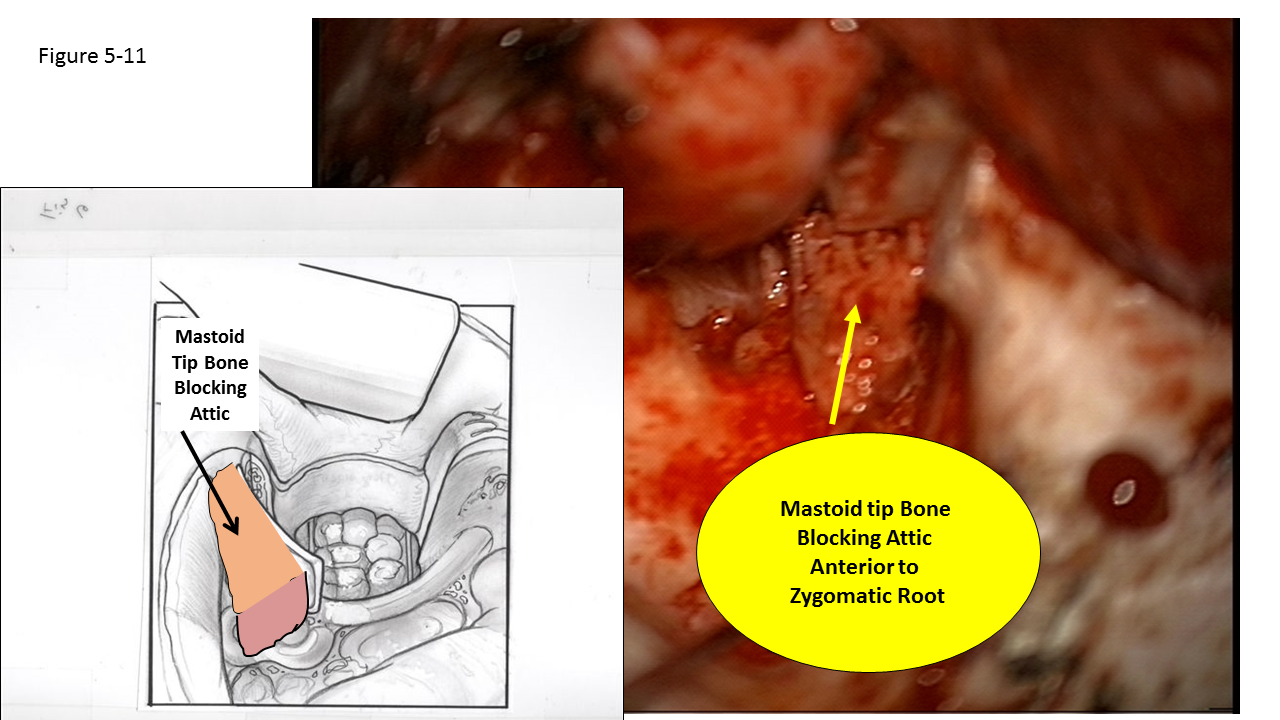
The posterior canal wall segment is then replaced, and several large cortical bone chips are harvested from the mastoid tip with a nasal chisel. The bone chips are trimmed to block the attic and mastoid from the mesotympanum. The attic bone chip should be large enough to span the distance between the scutum and the tympanic segment of the facial nerve and extend anteriorly into the zygomatic root. The facial recess is blocked in a similar manner.
| |
| |
Silastic is placed in the middle ear space with the tip of the Silastic into the eustachian tube. This is done before the posterior canal wall is placed.The fascia graft is placed between the ear drum and the Silastic. Gelfoam is placed between the fascia and Silastic to hold the graft in place. The posterior canal wall is then replaced.
-
Bone pâté is drained and then carefully placed in the attic and mastoid to hold the bone chips in place. The remainder of the mastoid and attic is filled with pâté to the level of the mastoid cortex. Packing should be firm to prevent posterior displacement of the canal wall when the external canal is packed.
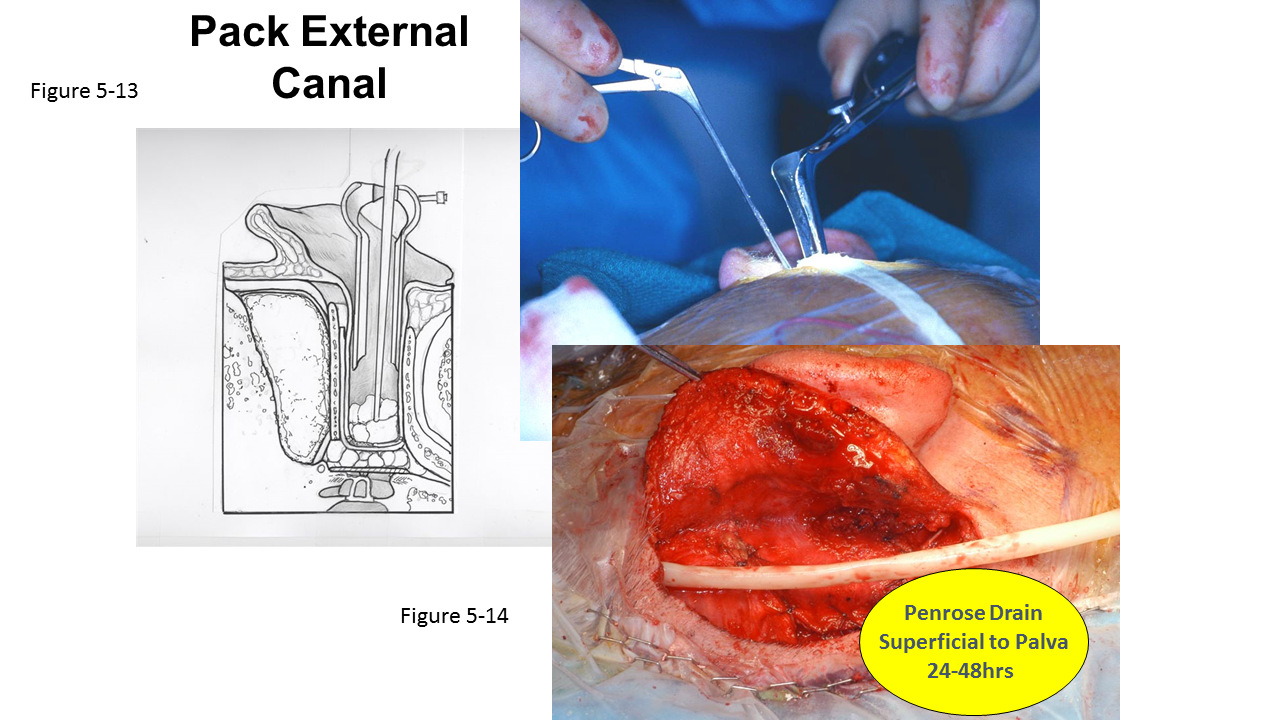
- Working transcanal, the external auditory canal is repositioned by inserting a long, thin Cottle nasal speculum to compress the posterior canal wall skin back into position. This is packed by several pieces of Gelfoam over the tympanoplasty graft, followed by half-inch iodoform strip gauze impregnated with bacitracin ointment.
- The Palva flap is closed, and a quarter inch Penrose drain is placed superficial to the Palva flap. The wound is closed in two layers. Interrupted closure is preferable for cutaneous closure. A standard mastoid dressing is applied.
| |
Post-operative Care
- Patients are given perioperative IV antibiotics for 48 hours. Adults are given piperacillin-tazobactam and levofloxacin. Patients under the age of 18 are administered piperacillin-tazobactam without levofloxacin. Penicillin-allergic patients are typically administered clindamycin with or without levofloxacin. Ciprofloxacin may be an alternative if levofloxacin is not available.
- The Penrose drain is removed on postoperative day number 2.
- The mastoid dressing is changed daily until discharge, at which time the patient is instructed to remove it in 2 to 3 days for a total of 5 days of compression. The patient may shower and get the incision wet after 5 days, but must exercise caution to keep the EAC dry.
- Patients are sent home with either oral levofloxacin (in adults), amoxicillin-clavulanate (in adults allergic to levofloxacin and patients under age 18), or clindamycin (in patients under 18, allergic to penicillin), to complete a 14 day course.
- Sutures and iodoform strip gauze are removed post-operative day 7. Antibiotic ear drops are then initiated until the next follow up appointment in 3 weeks (4 weeks post-operatively). Quinolone drops are preferred, but Cortisporin may be used if the round and oval windows are sealed.
- A second look tympanoplasty with ossiculoplasty is performed, typically 6 months after the initial tympanomastoidectomy. During this second surgery, the status of the middle ear and tympanic membrane graft are assessed, the middle ear is examined for the presence of residual cholesteatoma, and ossicular reconstruction is performed. Ossiculoplasty usually involves placement of a tragal or conchal cartilage graft over a titanium ossicular prosthesis. Please see Head and Neck protocol: Ossiculoplasty/Middle Ear Exploration.
References
Moffat DA, Gray RF, Irving RM. Mastoid obliteration using bone pate. Clin Otolaryngol Allied Sci 1994;19:149-57.
Gantz BJ, Wilkinson EP, Hansen MR. Canal wall reconstruction tympanomastoidectomy with mastoid obliteration. Laryngoscope 2005;115:1734-40.
Palva T. Surgical treatment of chronic middle ear disease. II. Canal wall up and canal wall down procedures. Acta Otolaryngol 1987;104:487-94.