
click on image above to enlarge; advance with cursor over border
Return to: Laryngeal Surgery (Benign Disease) Protocols
Background
Airway compromise associated with cricoarytenoid joint fixation due to rheumatoid arthritis is an uncommon but well-described complication of rheumatoid arthritis and is ascribed to acute inflammation or chronic ankylosis of the joint. The cricoarytenoid joint is characterized as a diarthrodial joint with a ligamentous capsule lined by synovium (Peters 2011).
Reported symptoms of cricoarytenoid joint (CAJ) arthritis include hoarseness, dyspnea, dysphagia, odynophagia (Montgomery 1963). Series from the 1960's suggested that a high percentage of patients with rheumatoid arthritis had CAJ involvement - ranging from 26% (Montgomery, 1963) to 27% (Bienenstock, 1963) and to 31% (Grossman, 1961). Improved contemporary medical therapy of rheumatoid arthritis is thought to make rheumatoid involvement of the CAJ much less common (Hoffman 2016).
CAJ arthritis may be identified with erythema and swelling of the arytenoid and aryepiglottic folds but also may also present without identifiable inflammation or swelling. It may present as an impaired vocal fold movement that may be difficult to discriminate from laryngeal paralysis or paresis (Peters 2011).
Autopsy study (Bienstock 1963) identified synovial proliferation, pannus and destruction of articular cartilage consistent with typical rheumatoid change (Peters 2011).
Septic cricoarytenoid arthritis has been reported in association with trauma, including that of prolonged intubation (Marmouset 2013) (obtaining CT image).
In 1981, Berger and Calcaterra reported septic cricoarytenoid arthritis occurring in a 66 you woman with a 10-year history of rheumatoid arthritis. Symptoms of neck tenderness and hoarseness prompted indirect laryngoscopy identifying a necrotic membrane on the surface of the left arytenoid with reduced glottis airway associated with decreased abduction to the left true vocal cord. Direct laryngoscopy identified a 1.5 cm sinus tract extending from the arytenoid surface to the cricoarytenoid joint with cultures growing Staphylococcus aureus and Pseudomonas aeruginosa. This report (in 1981- in the pre-CT imaging era) employed plain lateral neck x-rays to identify distention of the hypopharynx withsoft tissue mass impinging on the posterior larynx.
Case Report
68 yo woman with rheumatoid arthritis on long-term treatment with methotrexate, leflunomide and prednisone had been seen 5 months earlier by her local Otolaryngologist with mild stridor with shortness of breath and a transnasal laryngoscopy showing impaired abduction to the left vocal cord and 'some inflammatory changes'. She had been admitted with epiglottitis one month before that time with resolution with medical therapy and had an unremarkable laryngeal CT at that time.
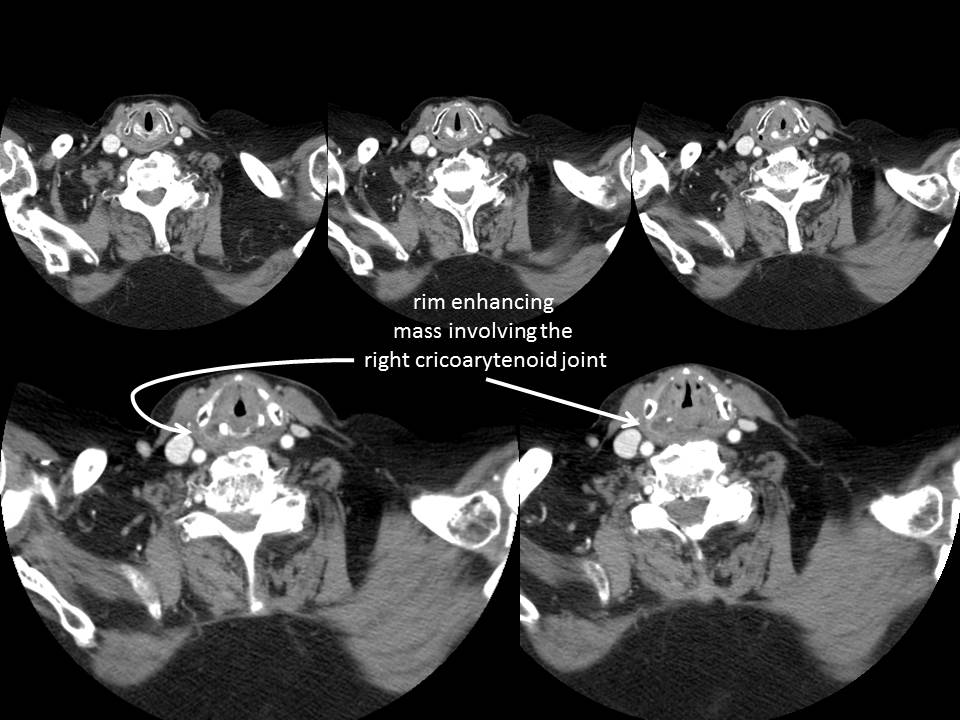
When seen by her local Otolaryngologist prior to this admission at the University of Iowa she reported pain with swallowing and choking on thin liquids with progressive shortness of breath and a cough productive of yellow green sputum. A CT (see below) was done showing a new ring enhancing lesion in the right cricoarytenoid joint region - not seen on the laryngeal CT done in March.
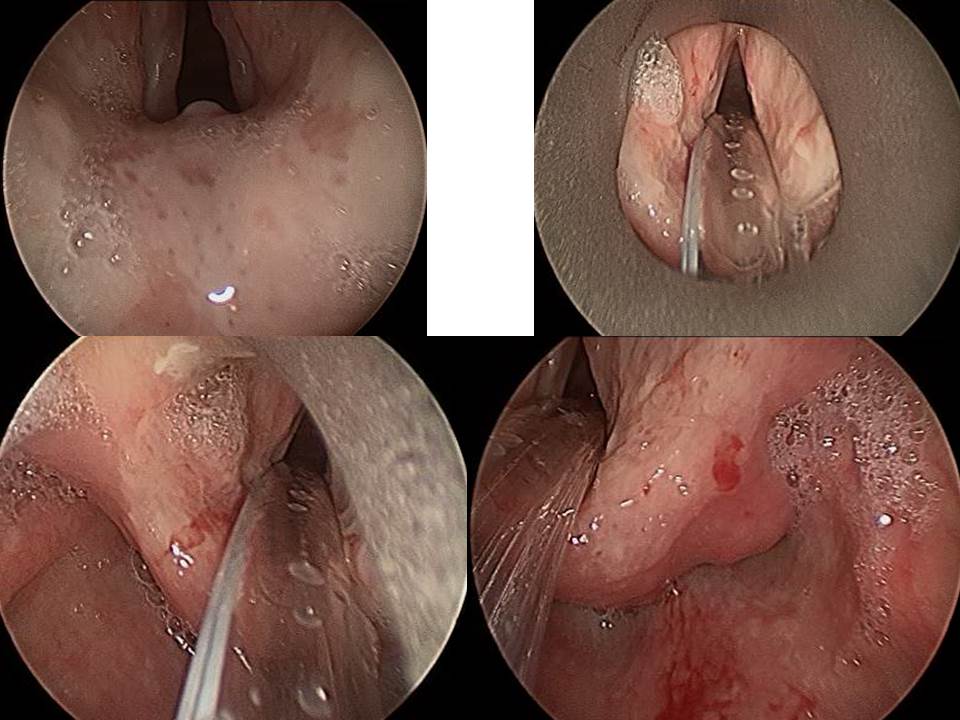
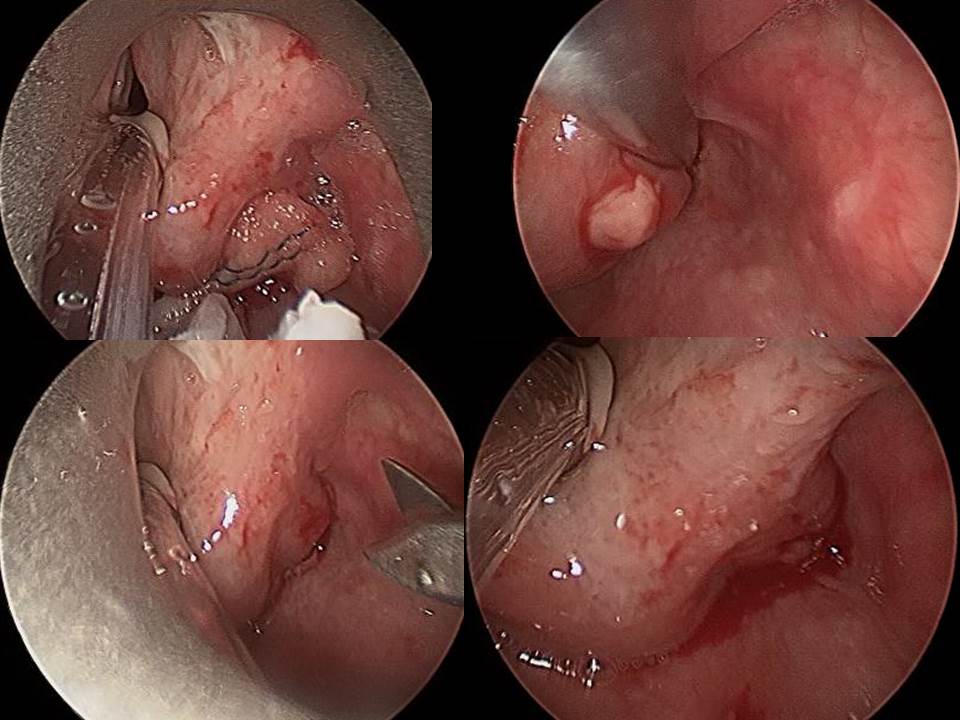
She was transferred to the University of Iowa where she was treated with an increased dose of steroid, antibiotics and examined with a bedside transnasal laryngoscopy showing an immobile right vocal cord with arytenoid swelling and a hypomobile left vocal cord permitting a sufficient airway for observation during which time vitamin K was given to reverse the anticoagulation (warfarin) she was on for atrial fibrillation for operative intervention the following day with microdirect laryngoscopy with drainage of right cricoarytenoid abscess with tracheostomy performed.
|
|
|
|
References
Foggia MJ, Hoffman HT. Cricoarytenoid joint abscess associated with rheumatoid arthritis. Am J Otolaryngol. 2019 May-Jun;40(3):459-461. doi: 10.1016/j.amjoto.2019.03.013. Epub 2019 Mar 28. PMID: 30948137.
Berger A and Calcaterra VE: Septic cricoartyenoid arthritis Otolaryngol Head Neck Surg.1983 Apr;91(2):211-3pp 211-213
Marmouset F, Moriniere S, Hammoudi K, Domengie F and Pujol A: Post intubation collected septic cricoarytenoid arthritis: case report Rev Laryngol otol Rhinol (Bord) 2013;134(2):113-6
Grossman A, Martin JR, Root HS: Rheumatoid arthritis of the cricoarytenoid joiont. Laryngoscope 1961 71:530-544
Bienenstock H, Ehlreich GE, Freyberg RH et al Rheumatoid arthritis of the cricoarytenoid joint; a clinicopathological study. Arthritis Rheum 1963 6:48-66
Montgomery WW: Cricoarytenoid arthritis. Laryngoscope 1963 73:801-836
Peters JE, Burke CJ, and Morris VH: Three cases of rheumatoid arthritis with laryngeal stridor. Clin Rheumatol 2011 May;30(5):723-7
Hoffman HT, Hoffman MR, Dailey SH: Editorial response to "A novel approach to cricoarytenoid joint injections, An anatomic study" Laryngoscope 2016 Aug 31 epub doi:10.1002/lary.26251
Sivam S, Burkett A, Simpson CB. A novel approach to cricoarytenoid joint injections: an anatomic study. 2016. doi: 10.1002/lary.26163. Epub ahead of print.
Wang L, Want F-S, Gershwin ME. Human autoimmune diseases: a comprehensive updated. J Intern Med 2015;278:369–395.
Dailey SH, Kobler JB, Hillman RE, et al. Endoscopic Measurement of vocal fold movement during adduction and abduction. Laryngoscope 2005;115:178–183.