






click on image above to enlarge; advance with cursor over lateral border
return to protocol: Posterolateral Neck Dissection
more anatomic detail: Case example 2 Posterolateral Neck Dissection and Anatomy
History
44-year-old woman whose family members identified a pigmented lesion at the junction of the hair bearing scalp in the postauricular region in September 2006. This warranted an evaluation and referral after a January 2007 small punch biopsy that showed invasive melanoma to a depth of only 0.88 mm despite the 1 x 1 cm plaque-like area with elevations that may suggest other areas that could potentially be more invasive as to their depth.
Biopsy:
0.88 mm melanoma of posterior neck/scalp
Resection of primary site (porcine skin graft) with sentinel lymph node biopsy (SLN bx):
Malignant melanoma, superficial spreading type, Breslow depth 0.99 mm, Clark's level IV. Tumor present 0.9 cm from 9 o'clock margin.
Metastatic malignant melanoma identified in one lymph node (1/1), less than 0.1 cm in greatest dimension, no extracapsular (left level 5 underlying SAN)
Further resection of primary site with skin graft reconstruction:
A. Skin, 12 to 3 o'clock, excision: Acute and chronic inflammation.
B. Skin, 3 to 6 o'clock, excision: Acute and chronic inflammation.
C. Skin, 6 to 9 o'clock, excision: Acute and chronic inflammation.
D. Skin, 9 to 12 o'clock, excision: Acute and chronic inflammation.
Posterolateral neck dissection: 33 nodes negative
Sample Operative Note
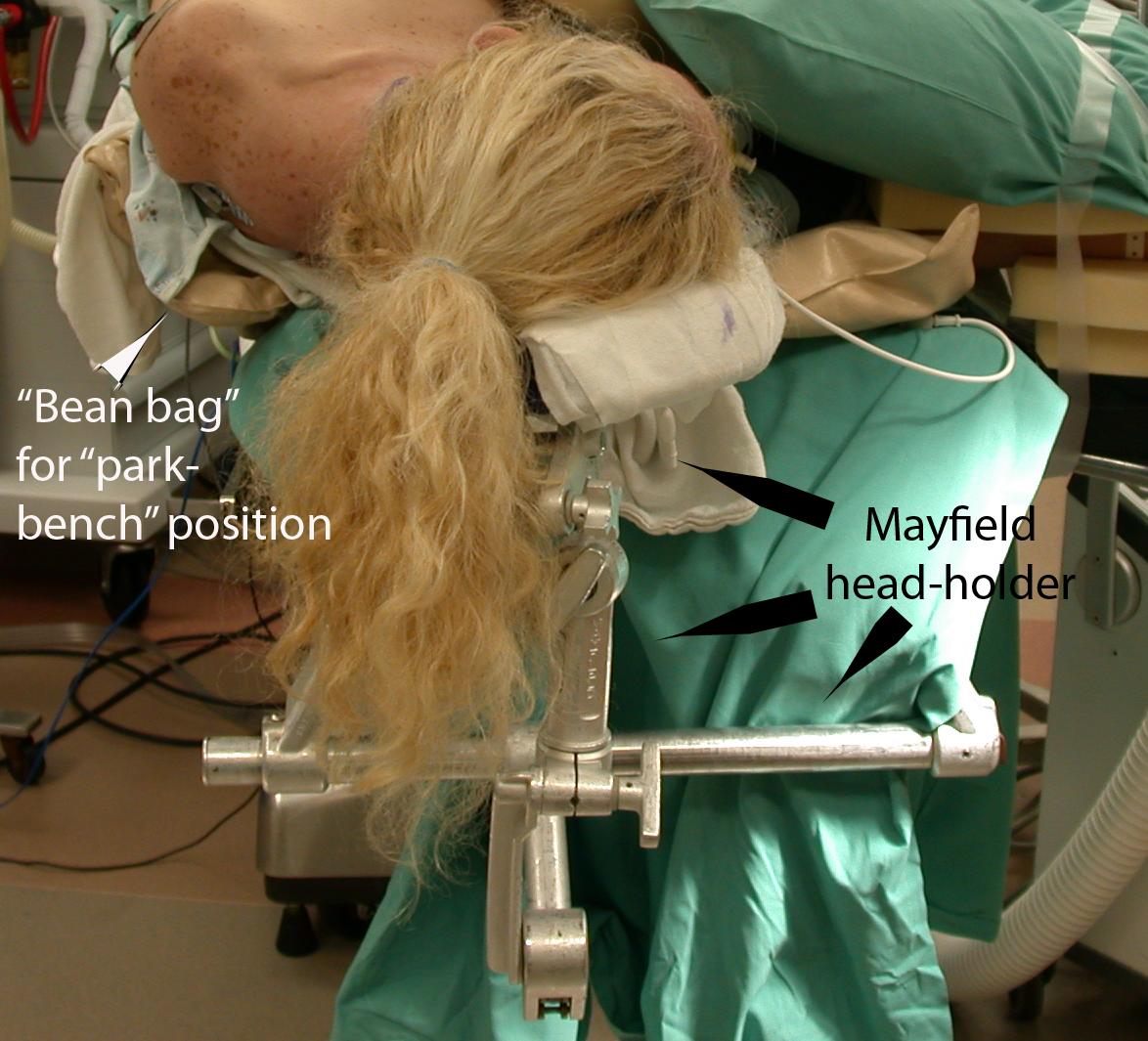
After confirming fully consent, patient was brought in and was induced with intravenous mask anesthesia, patient was intubated. Head of bed was rotated 180 degrees. Patient had been previously positioned on a beanbag and head was positioned on a Mayfield headrest. Patient was rolled into the right lateral position and beanbag was deflated. A small area of hair over the previous incision and over the extent of the posterolateral neck dissection was performed, the incision was marked extending from the original melanoma defect incorporating an ellipse over one of the sentinel lymph node biopsy sites and headed down anteroinferiorly towards the clavicle. This was injected with 10 cc of 1:100,000 parts epinephrine. Patient was prepped and draped in the usual sterile fashion. Skin incision was made with a 15 blade down through the subcutaneous tissue. The subcutaneous level of dissection was performed with care being insured to avoid damage to the hair follicles and leave a slight amount of cobblestoning on the superficial surface.
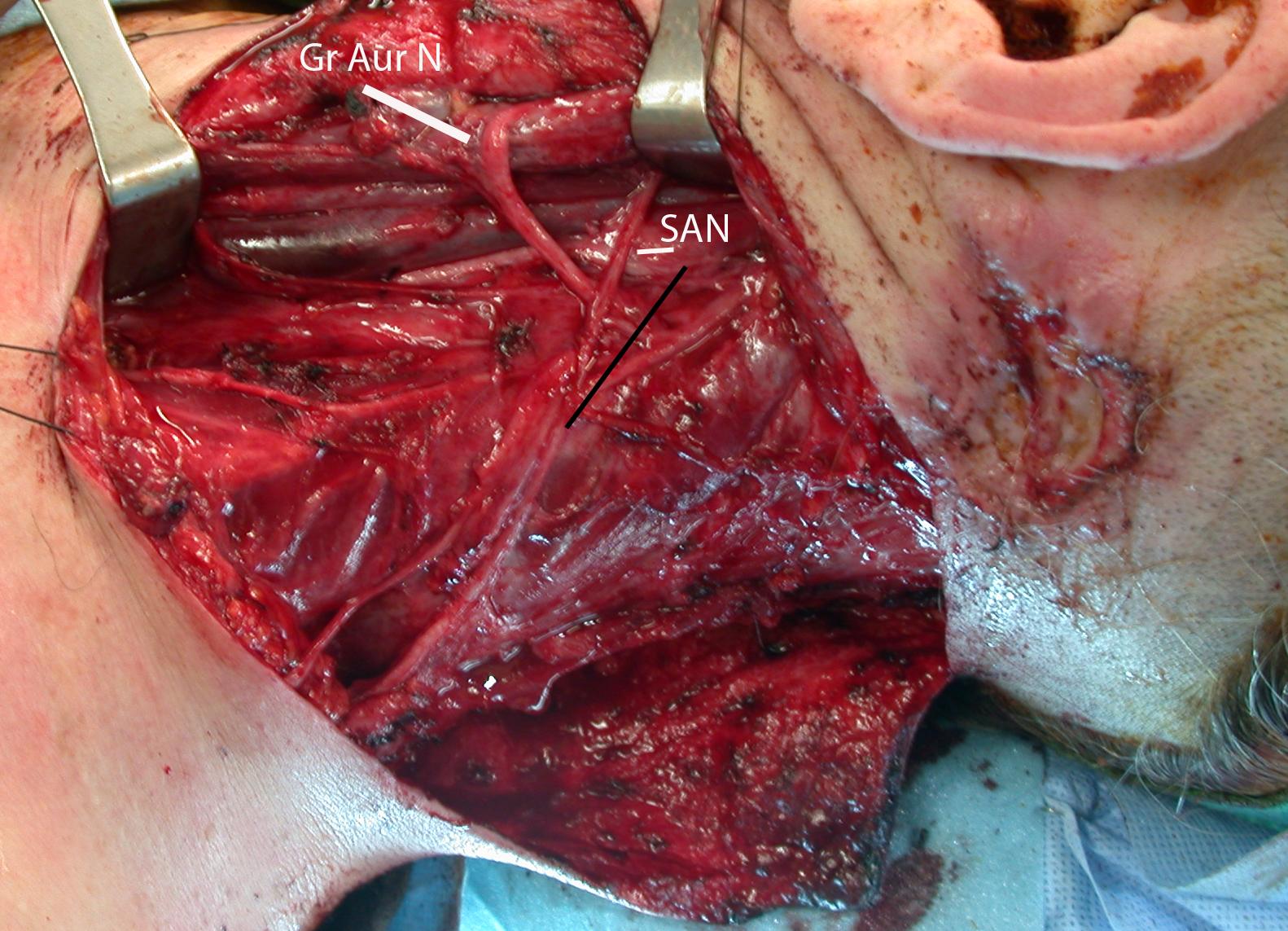
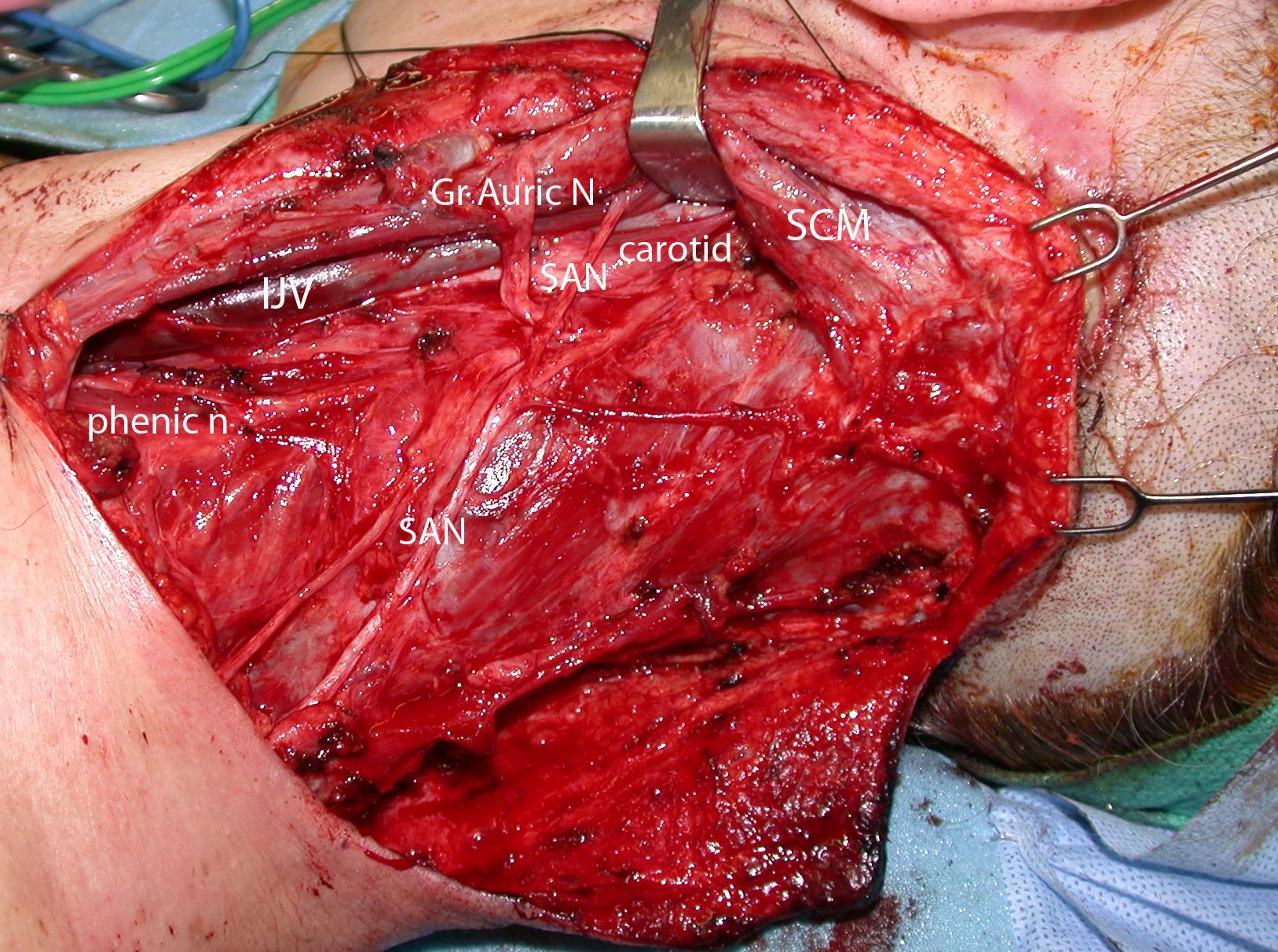
Dissection proceeded anteriorly up towards the posterior border of the sternocleidomastoid muscle. The platysma was divided over the anteroinferior portion of the incision and dissection was carried down on top of the sternocleidomastoid muscle. Posterior border was clearly defined and the SCM was retracted forward. The spinal accessory nerve and the great auricular nerve were both identified and preserved in their entirety. Accessory nerve was traced posteriorly from the sternocleidomastoid muscle to the trapezius. It was also further traced deeply from the sternocleidomastoid muscle up to the skull base. Tissue was reflected posteriorly off the sternocleidomastoid muscle until the internal jugular vein was reached. Again, fascia was reflected posteriorly off the internal jugular vein until the carotid artery and vagus nerves were identified which were preserved in their entirety. After reflecting superoposteriorly off the carotid, vagus and internal jugular veins in an inferior to superior manner the hypoglossal nerve was also identified deep and was left preserved.
Tissue was dissected from the mastoid tip and the sternocleidomastoid muscles superiorly and reflected posteriorly. The inferior aspect of the dissection was at the transverse cervical neurovascular bundle. The tissue was swept posteriorly off the floor of the dissection and up towards the trapezius. The levator scapula was identified as was the splenius capitis tissue, reflected off of those muscles and a portion of the trapezius was divided allowing inferior reflection of the suboccipital node group. During reflection of this material, the previous scar from the lymph node biopsy was taken as part of the main specimen. Specimen was cleaned off the trapezius (and under its upper aspect to include suboccipital nodes), the splenius capitis, lelevator scapulae deeply and the scalene muscles deeply, and was removed from the body and sent off as per the specimen section.
Meticulous hemostasis was obtained of the wound. Three 10 mm fully perforated Jackson-Pratt drains were inserted inferior to the skin flaps. One went up the posterior midline, the second went superficially over the incision, and the third came up in the gutter along the internal jugular vein and carotid. These were all secured with 3-0 nylon in the standard fashion. The platysma was closed using 3-0 Vicryl in interrupted fashion, the dermis was closed using 4-0 Monocryl in interrupted fashion. A small standing cone deformity was excised revealing the area of previous elliptical skin excision. The scalp skin was reapproximated using staples. The neck skin was reapproximated using 5-0 Prolene in a running locked fashion. Bacitracin was applied to the incision. The patient's head was washed. Patient was turned back to Anesthesia, placed on a regular head bed, bean bag deflated and taken to recovery in stable condition.