








return to: Temporal Arteritis aka Giant Cell Arteritis and Temporal Artery Biopsy Technique
see also: Steroids Side Effects Systemic Corticosteroid Therapy Adverse Effects
CLINICAL HISTORY
S.W. is a 66-year-old Caucasian female who presented with 4 episodes of transient R sided vision loss, a 5-day history of worsening tip of tongue burning, and a 1 month history of non-pulsatile headache mostly of occipital distribution with scalp tenderness at 'veins' noted while combing her hair. She was found to have elevated LFTs, ESR and CRP. She had a total thyroidectomy 2 weeks prior to presentation for papillary thyroid carcinoma with neck dissection revealing disease metastatic to lymph nodes.
 Initial Presentation
Initial Presentation  10 Days after initial presentation
10 Days after initial presentation
S.W. was started on Solumedrol 1000mg qd for a presumptive diagnosis of temporal arteritis. On hospital day 3, she underwent a R temporal artery biopsy:
*Biopsy Photo is NOT intended for instructional purposes, only for completeness in case report. For instruction, see 'Temporal Artery Biopsy' in Temporal Arteritis aka Giant Cell Arteritis and Temporal Artery Biopsy Technique.
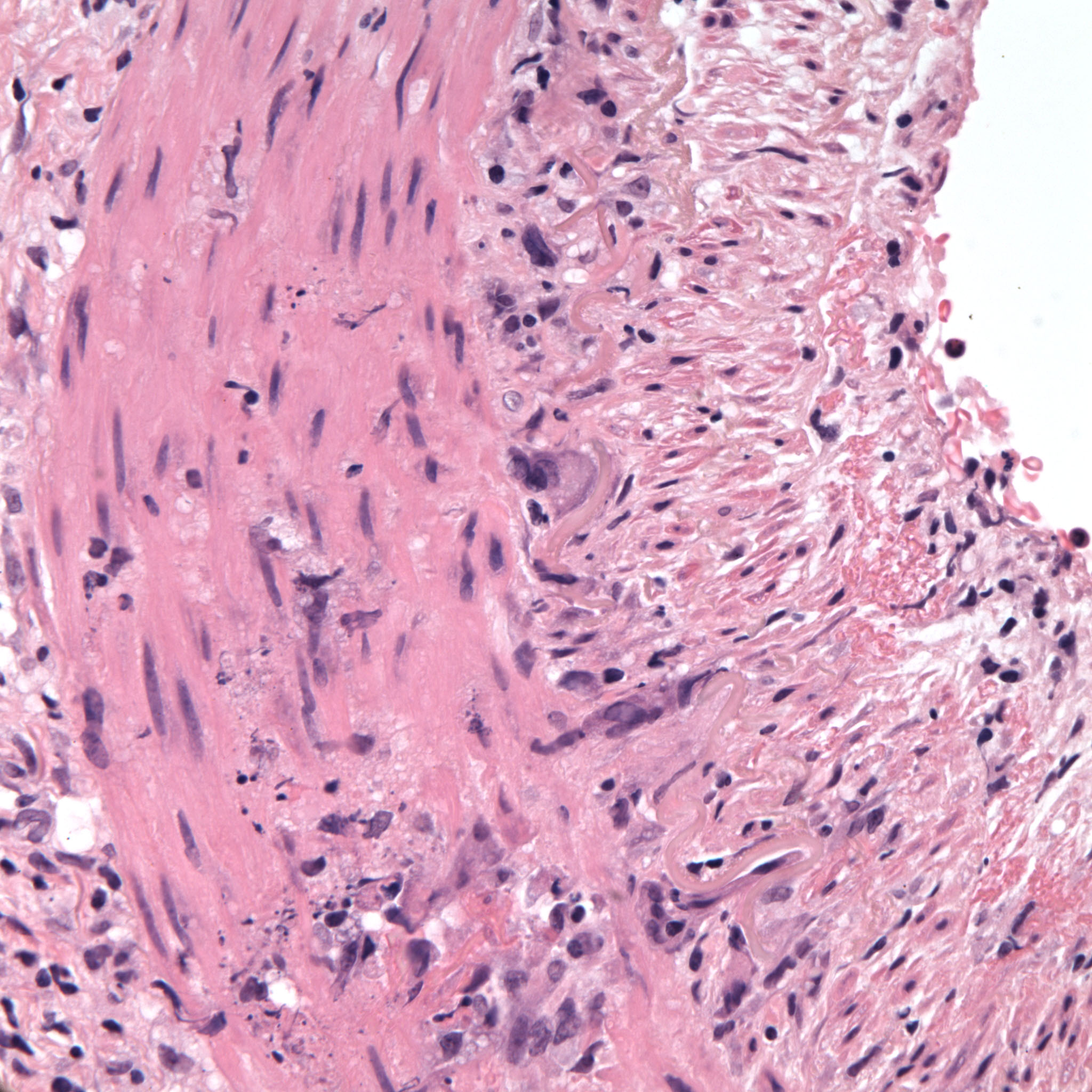
MICROSCOPIC DESCRIPTION
The intima is relatively unremarkable. The muscularis layers and adventitial layers are infiltrated with lymphocytes and epithelioid histiocytes. Many of these are adjacent to the internal elastic lamina. The lamina demonstrates mild disruption on elastic stain.
DIAGNOSIS
Granulomatous arteritis consistent with giant cell arteritis.
TREATMENT
Solumedrol 1000mg qd x 3days, then Prednisone taper 80mg qd x 1wk, 70mg qd x 2wks, 60mg qd x 2wks
see: Steroids Side Effects Systemic Corticosteroid Therapy Adverse Effects
REFERENCES
Pathology Slides: Courtesy of Nasreen A. Syed MD, Depts. of Ophthalmology and Pathology, University of Iowa