



see: Thyroglossal Duct Cyst Embryology, Anatomy, and Treatment (video)
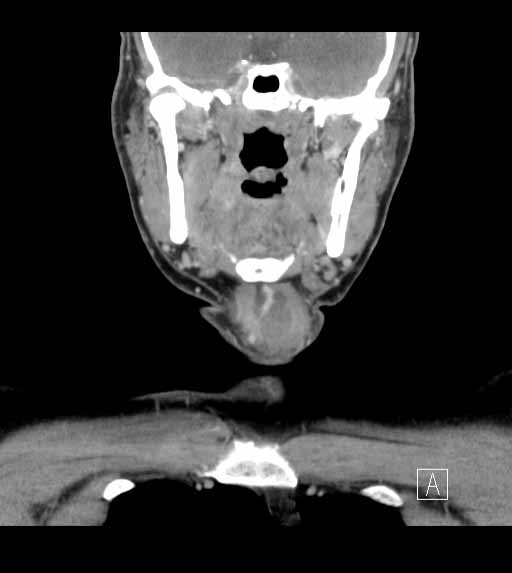
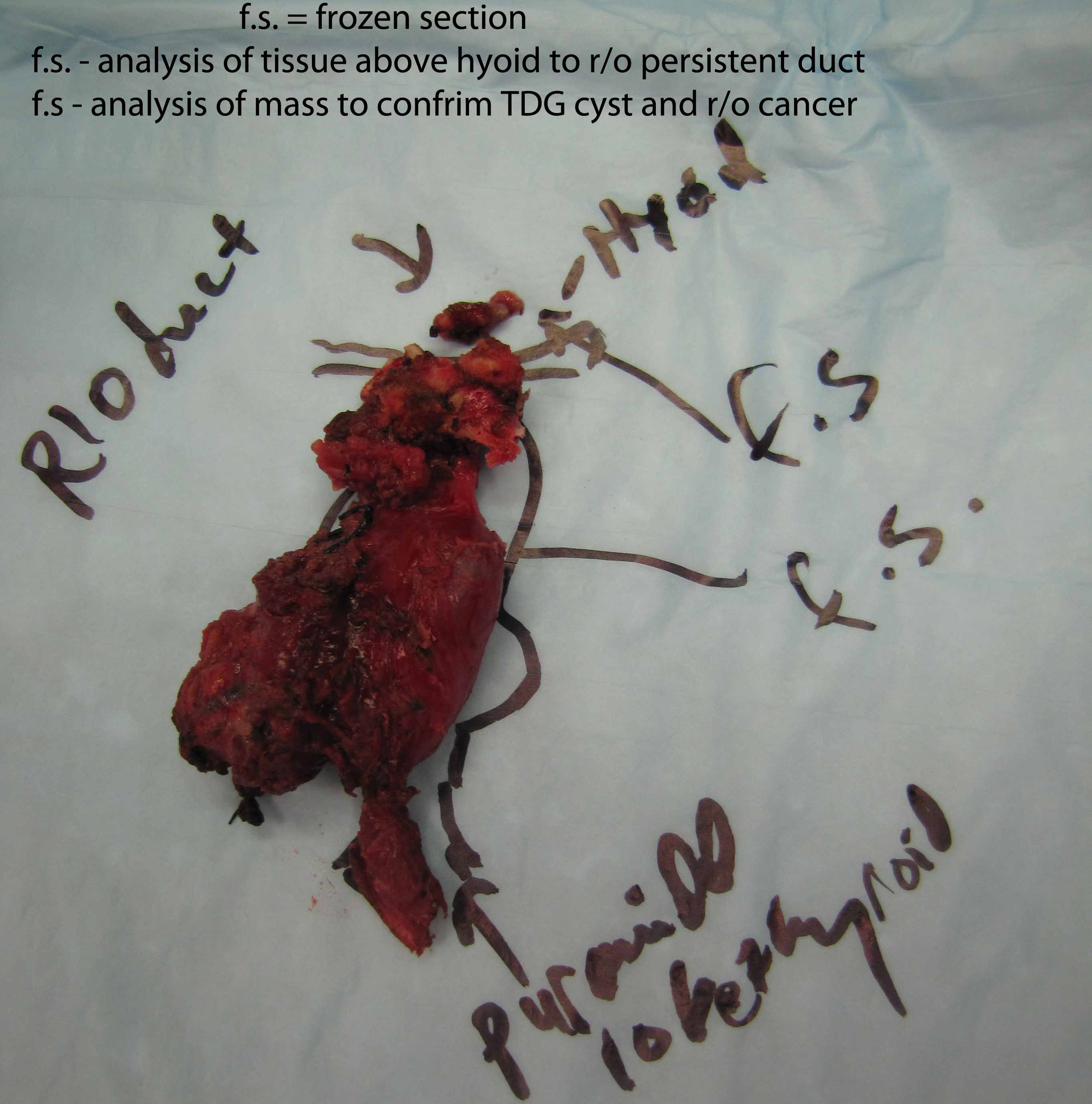
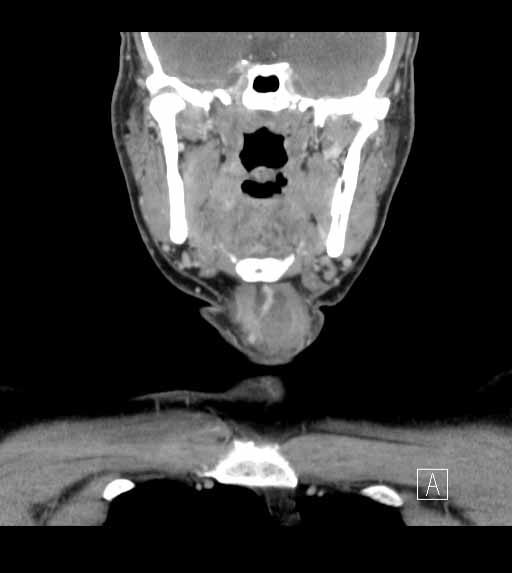
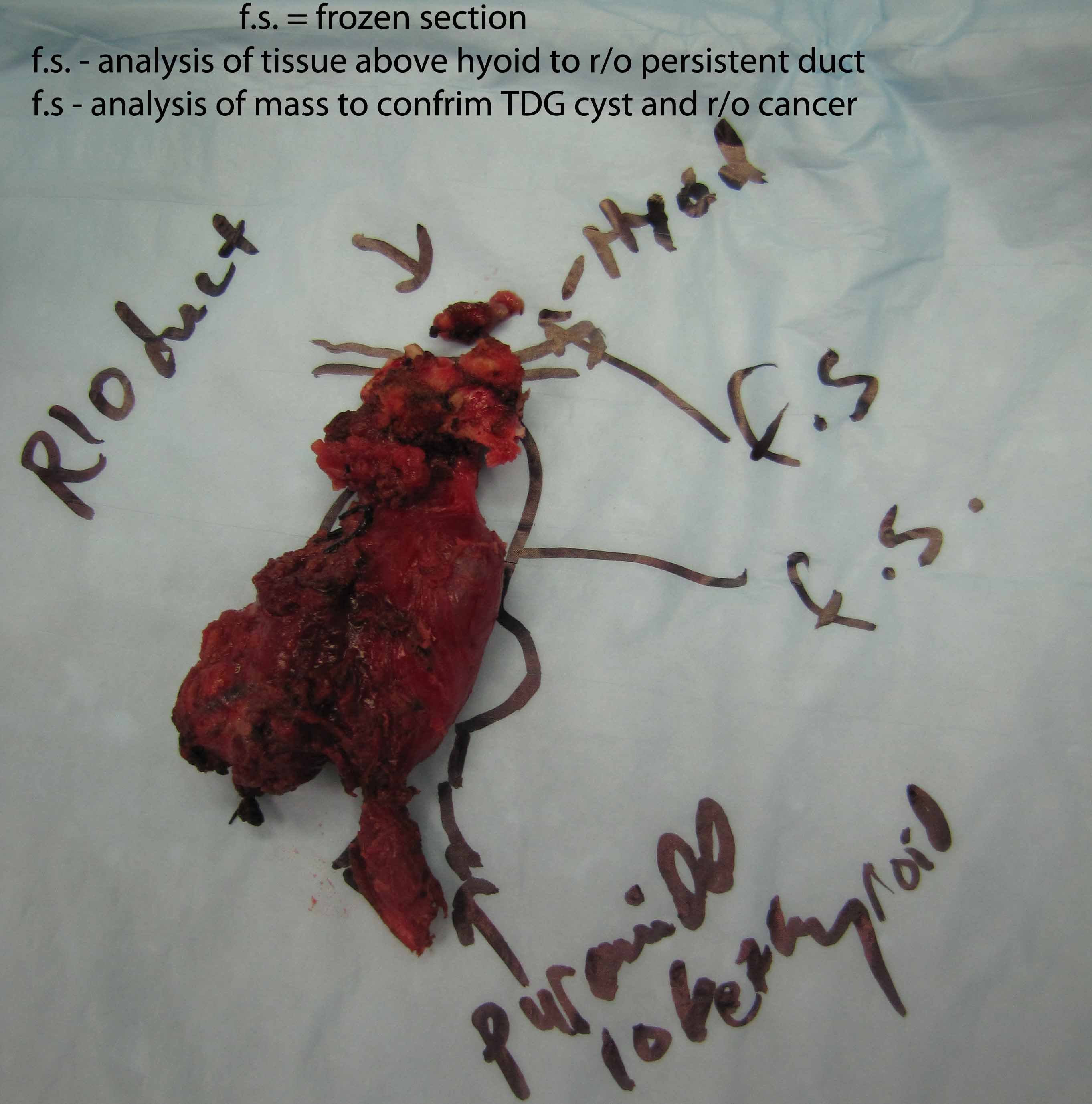
Case example - thyroglossal duct cyst with tract through to oropharynx
return to: Thyroglossal Duct Cyst Excision
Sample Operative Note (modified, but applicable to case presented)
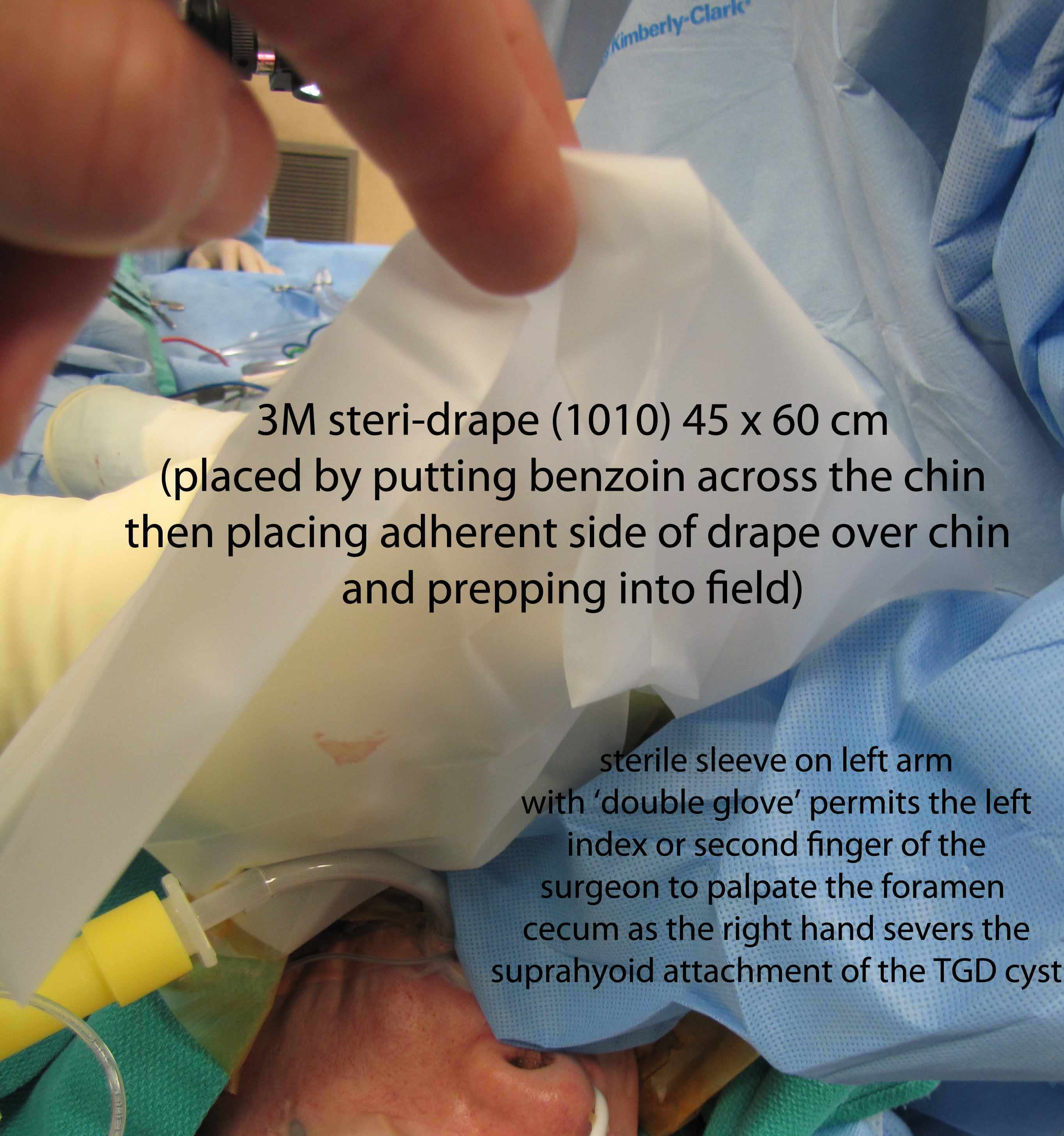
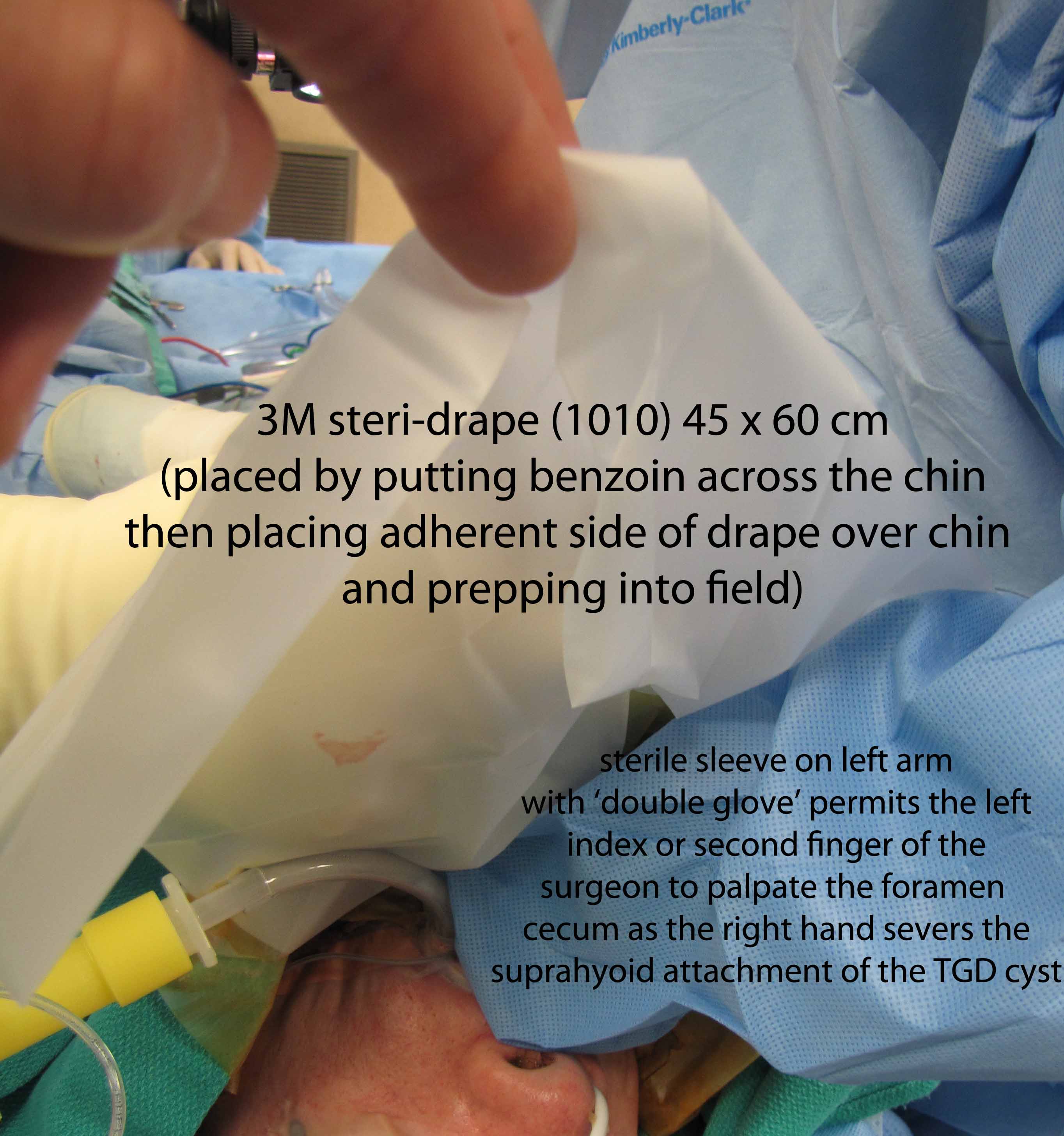
After written informed consent was obtained with a history and physical reviewed along with a brief 'time out', the patient was placed under general anesthesia with endotracheal intubation with a 6.0 MLT tube. The patient was positioned with the back-elevated, neck extended position with the head toward anesthesia. Benzoin was placed across the chin and a 1010 drape placed with adherent (sticky) portion applied to benzoined region with remained draped over mouth to permit later access to oral cavity.
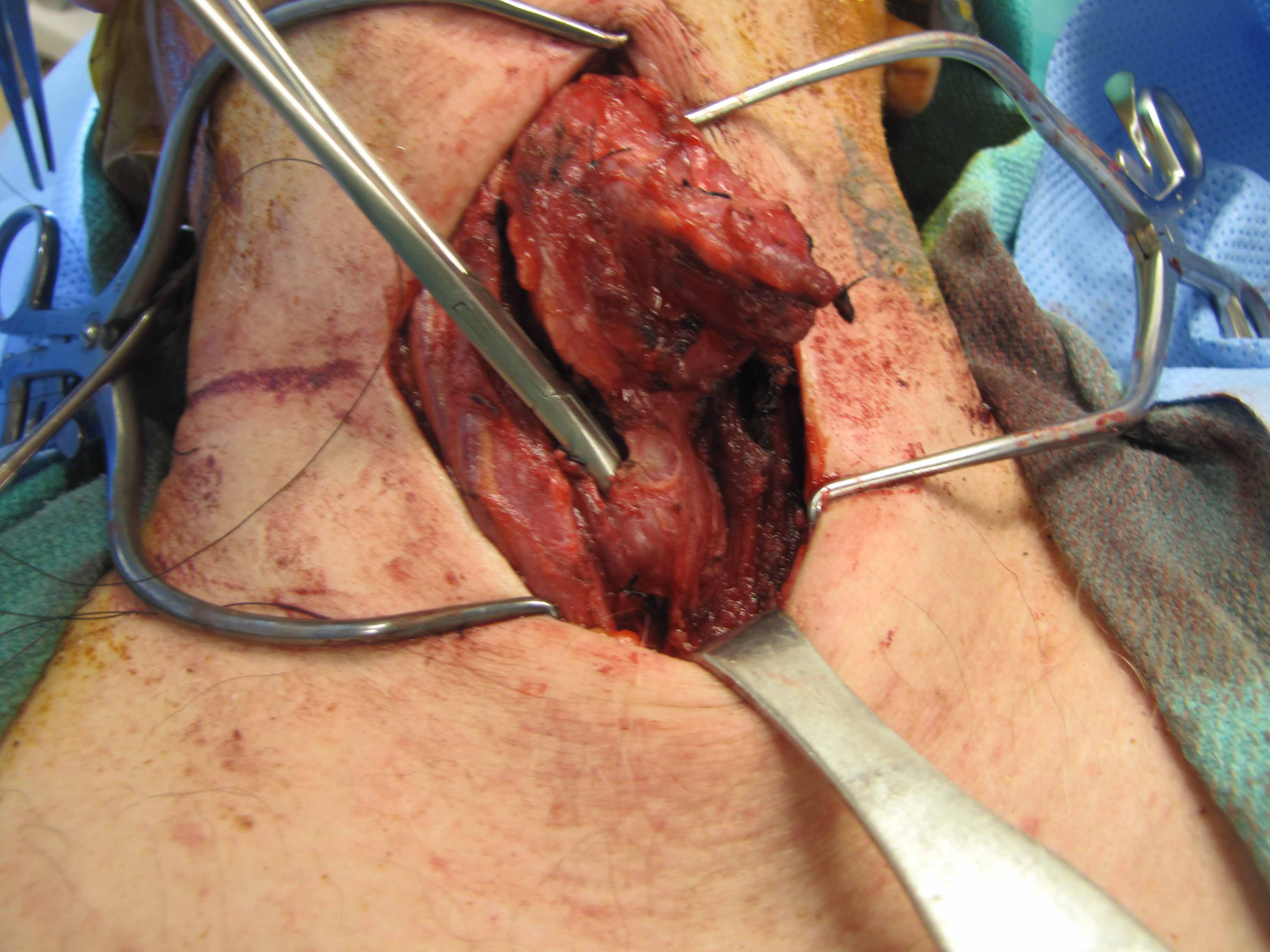
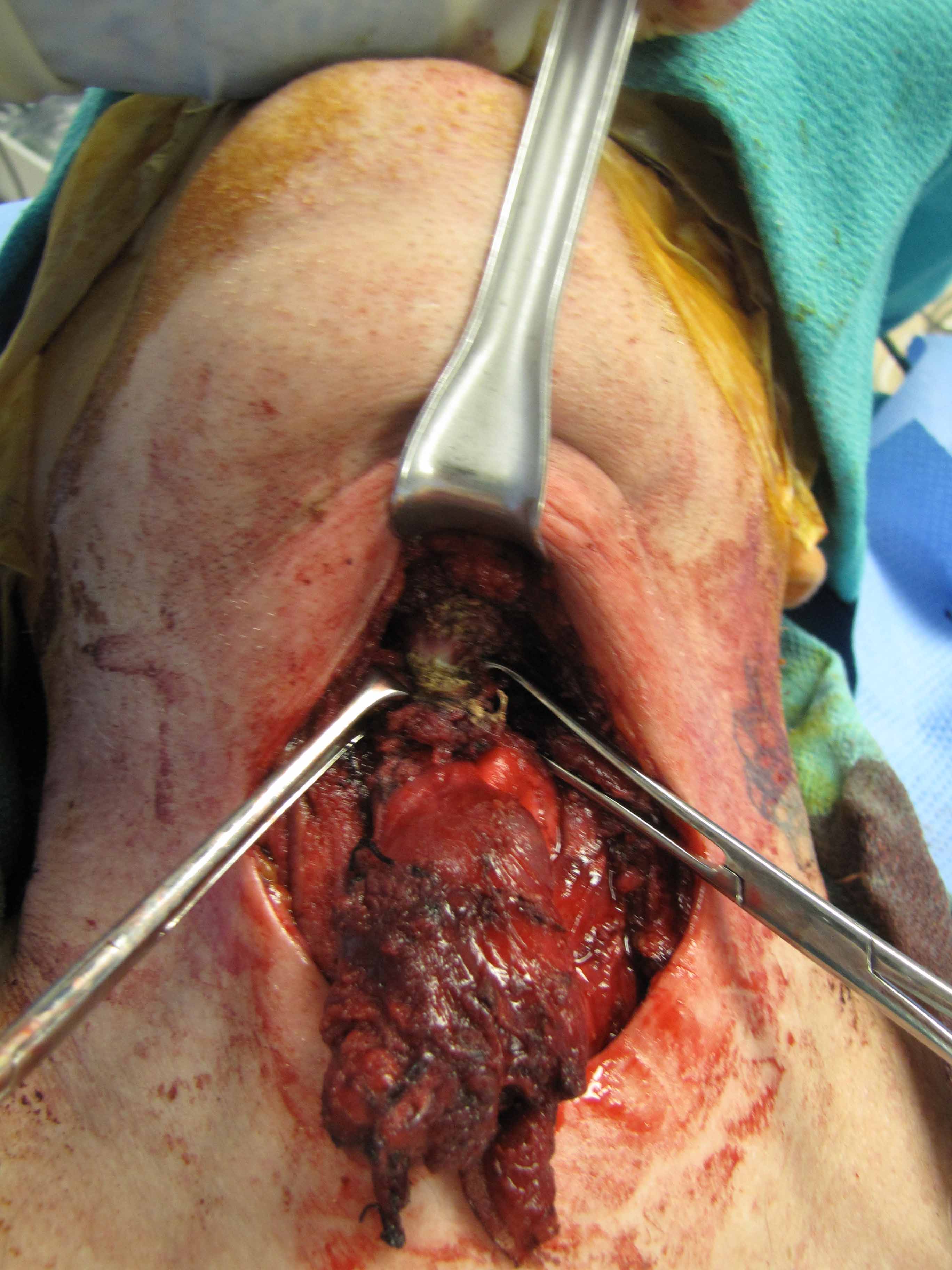
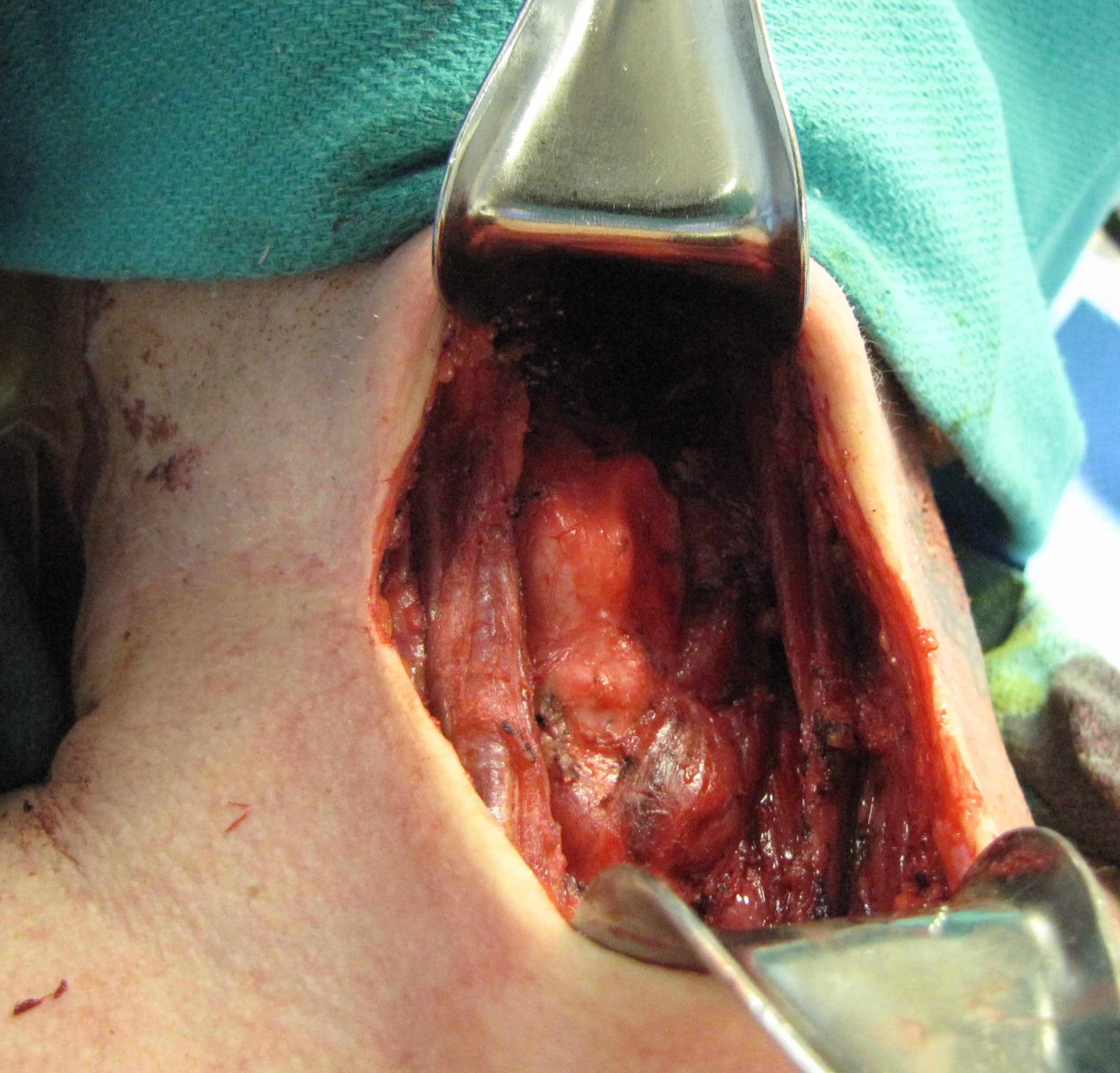
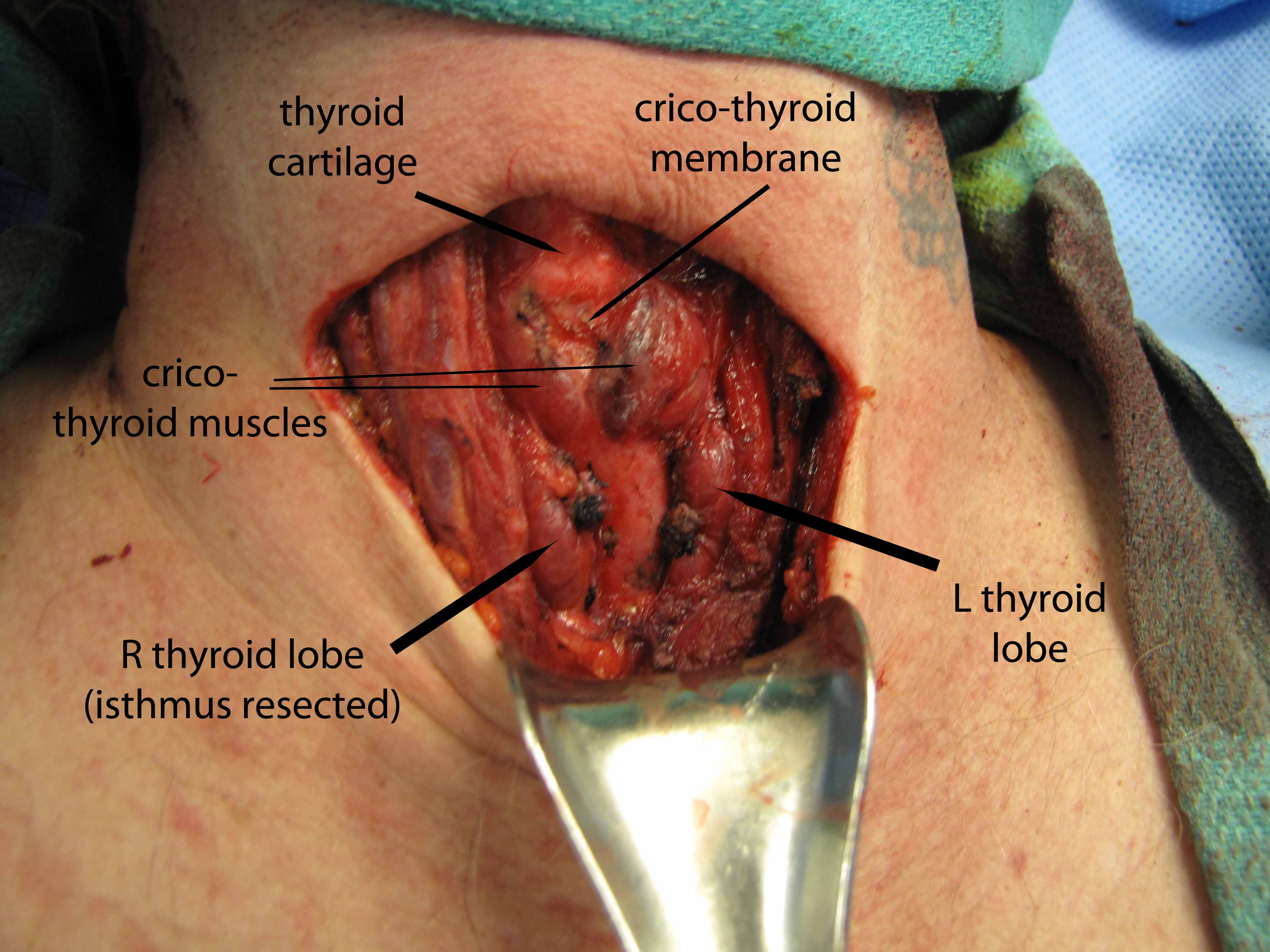
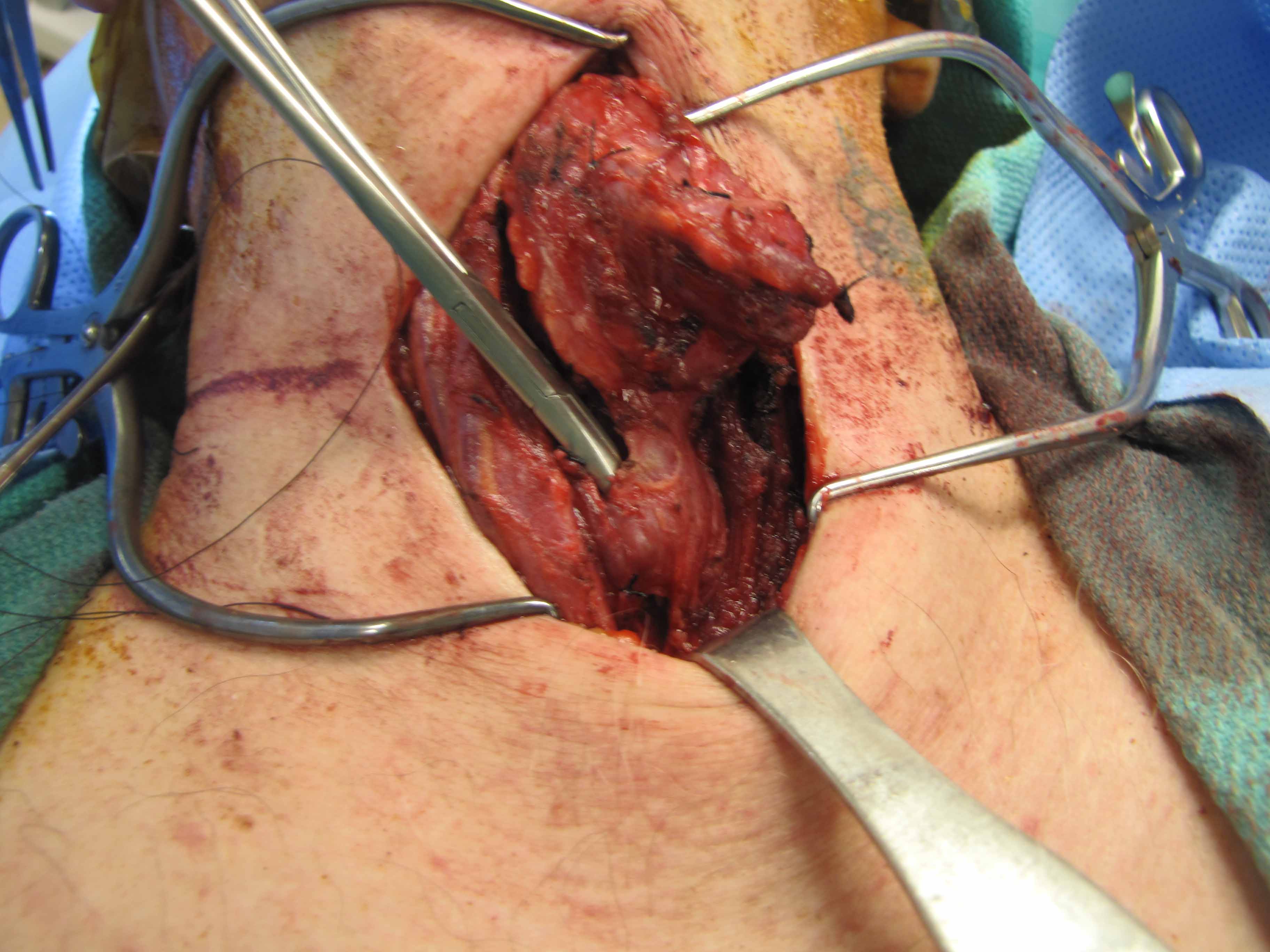
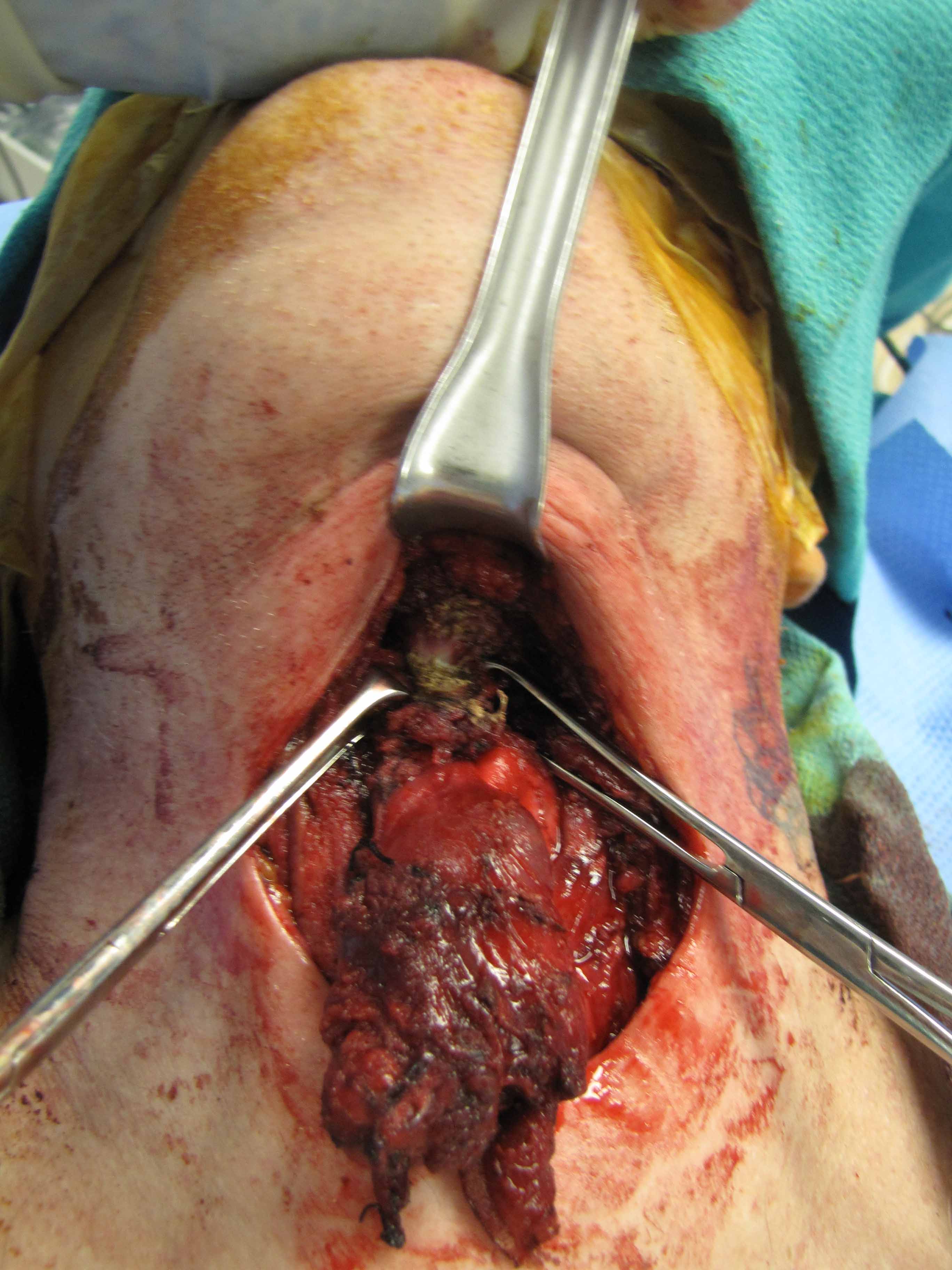
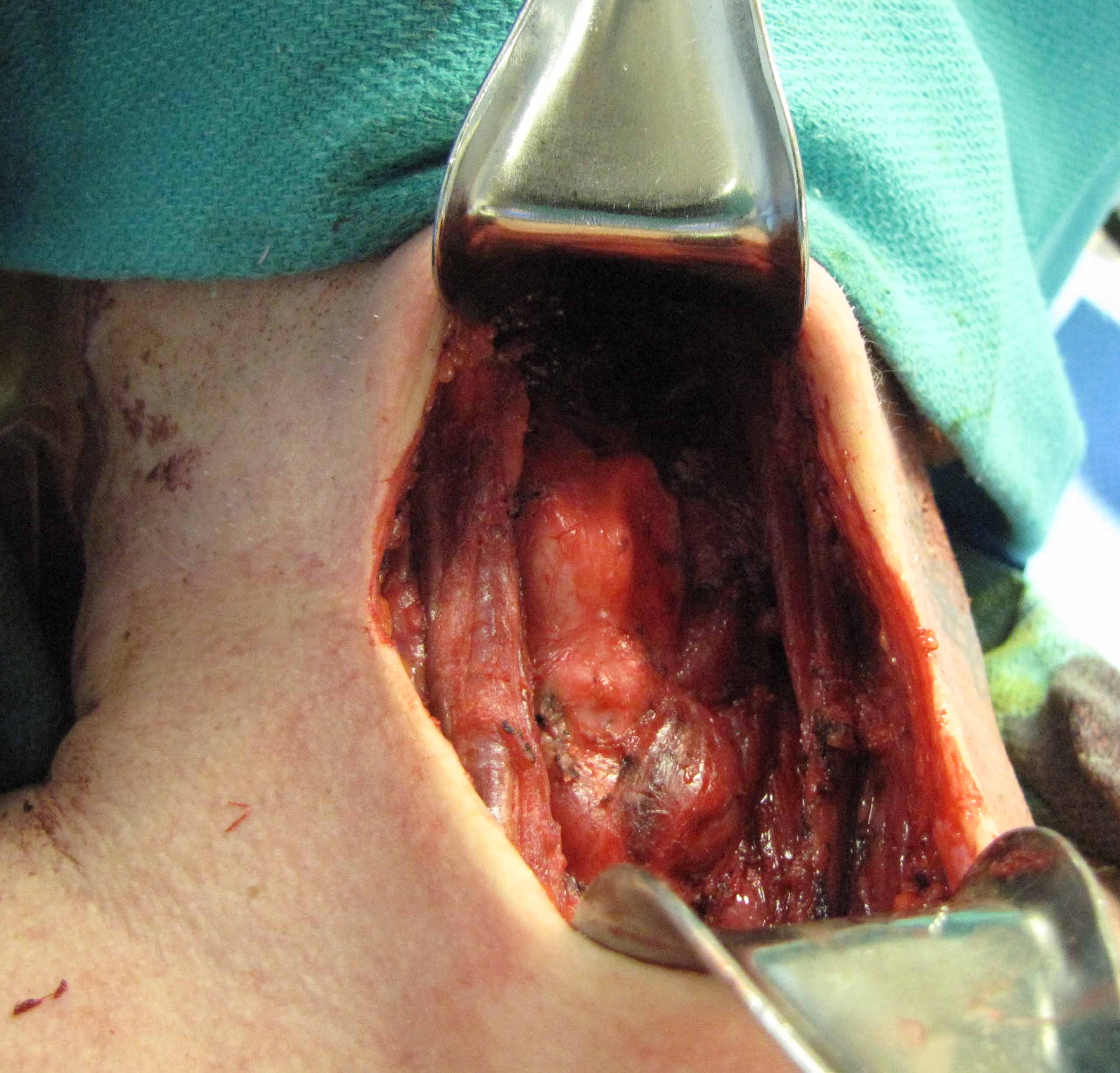
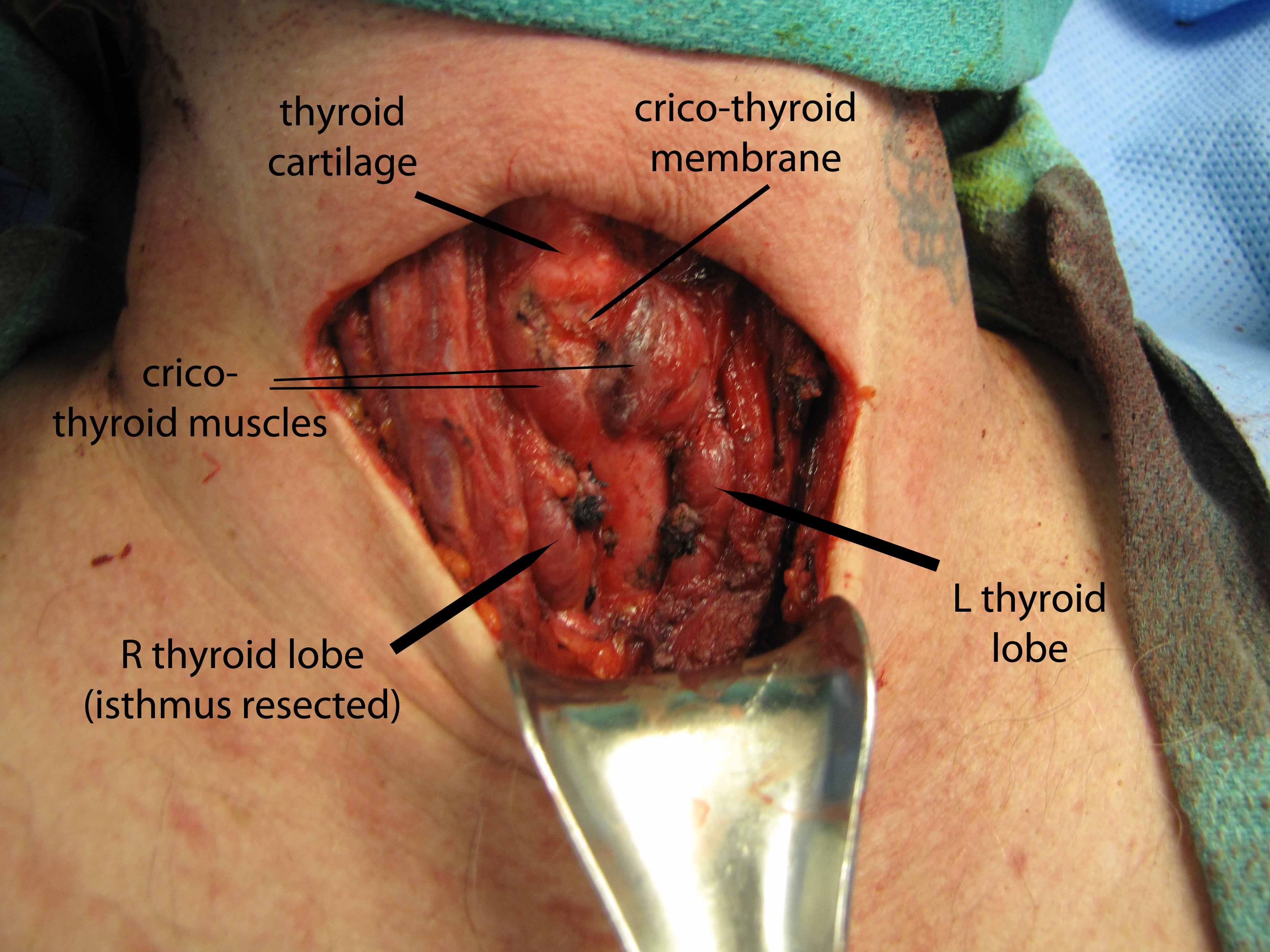
The patient was then prepped (including 1010 drape) and positioned for a central neck dissection thyroglossal duct cyst removal. Just to the left of midline, a large mass was palpated. A 15 blade was used to incise the skin with a horizontal marked incision and down onto the mass. Subplatysmal flaps were raised superiorly and inferiorly down to the area of the thyroid. We divided the straps midline. Of note just to the left of midline, the strap muscles were adherent to the cyst. Inferiorly the cricoid cartilage was identified as well as the thyroid. The mass was dissected around and it appeared to be in continuity with the pyraminal lobe and isthmus. The thyroid was divided to the right and then to the left and tied off with a 3-0 silk running stitch to permit resection of the isthmus in-continuity with the mass extending above.
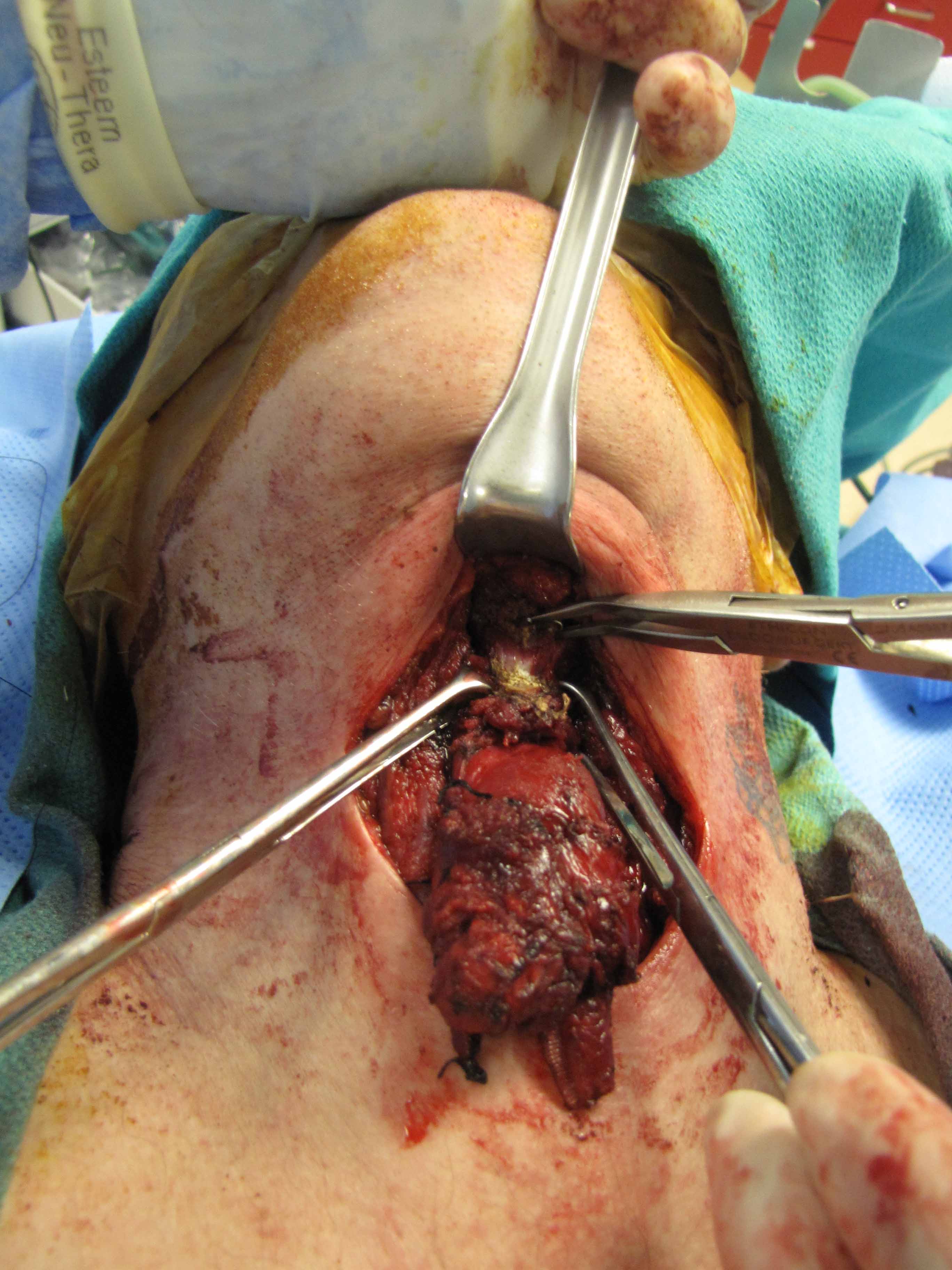
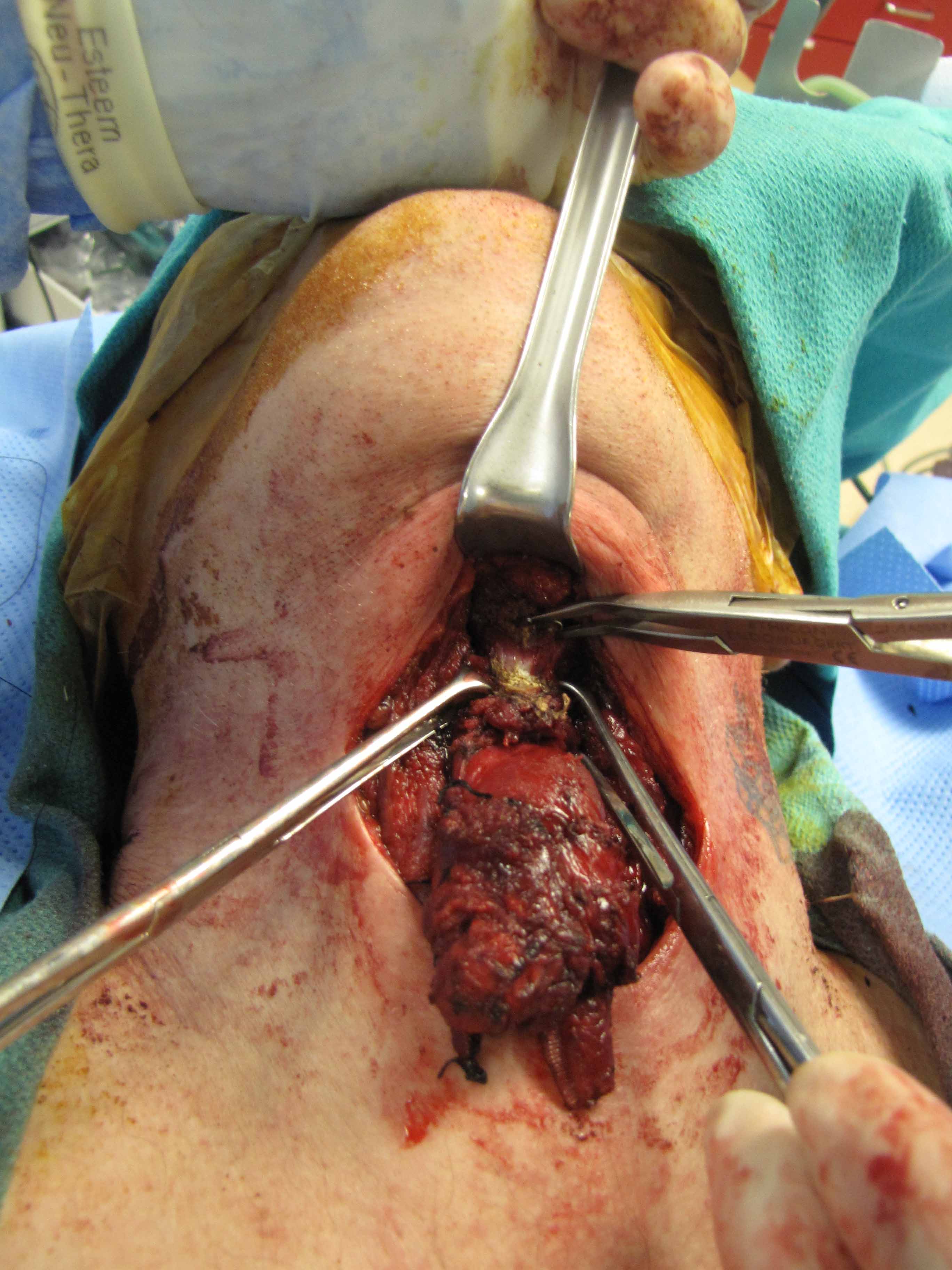
We dissected the cyst and mass from an inferior to superior direction as it was removed from the cricothyroid muscles and thyroid cartilage up to the hyoid bone with care to avoid the superior laryngeal nerves. A small amount of strap musculateure was removed with the specimen where it was densely adherent on the left side.
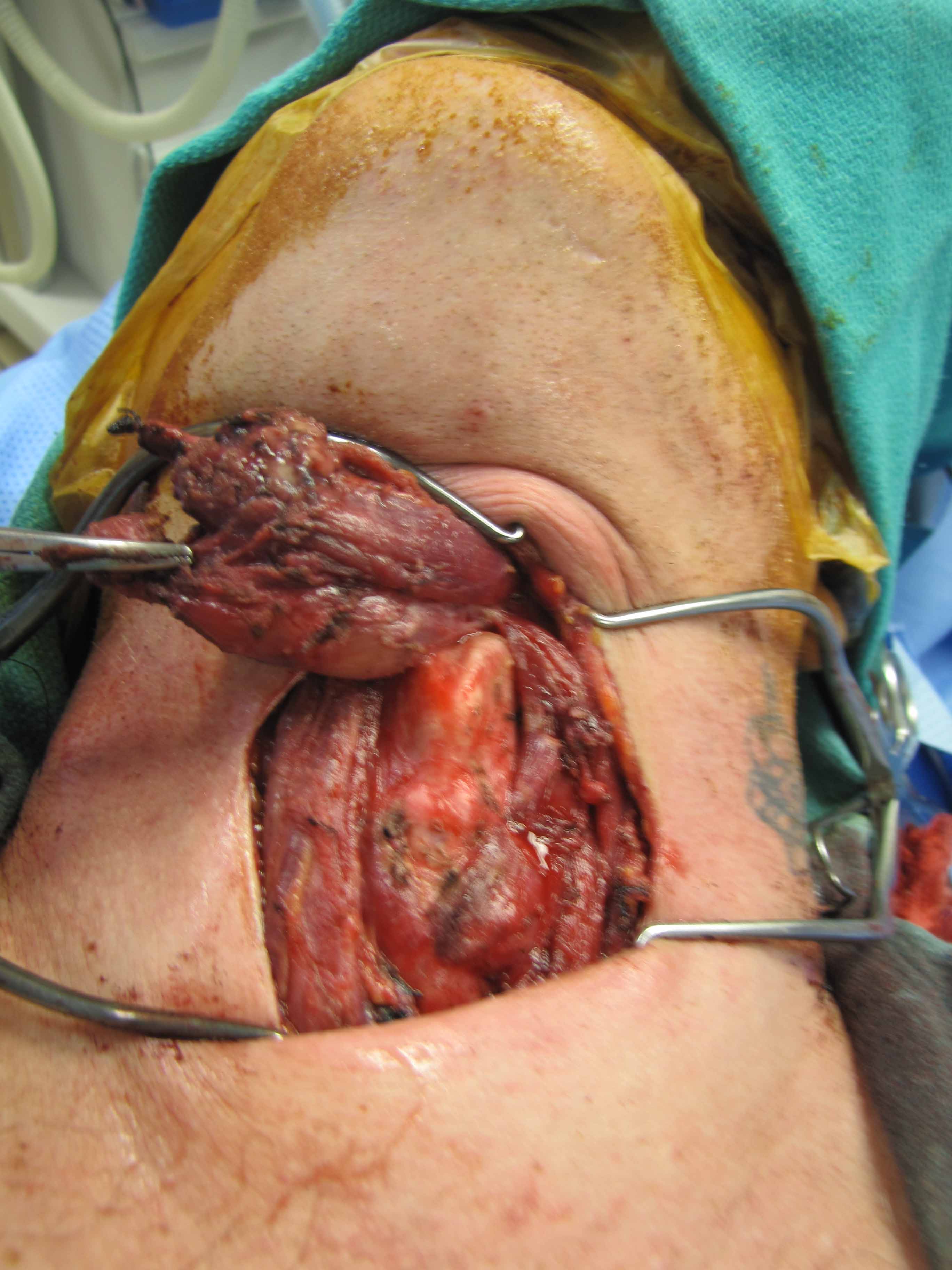
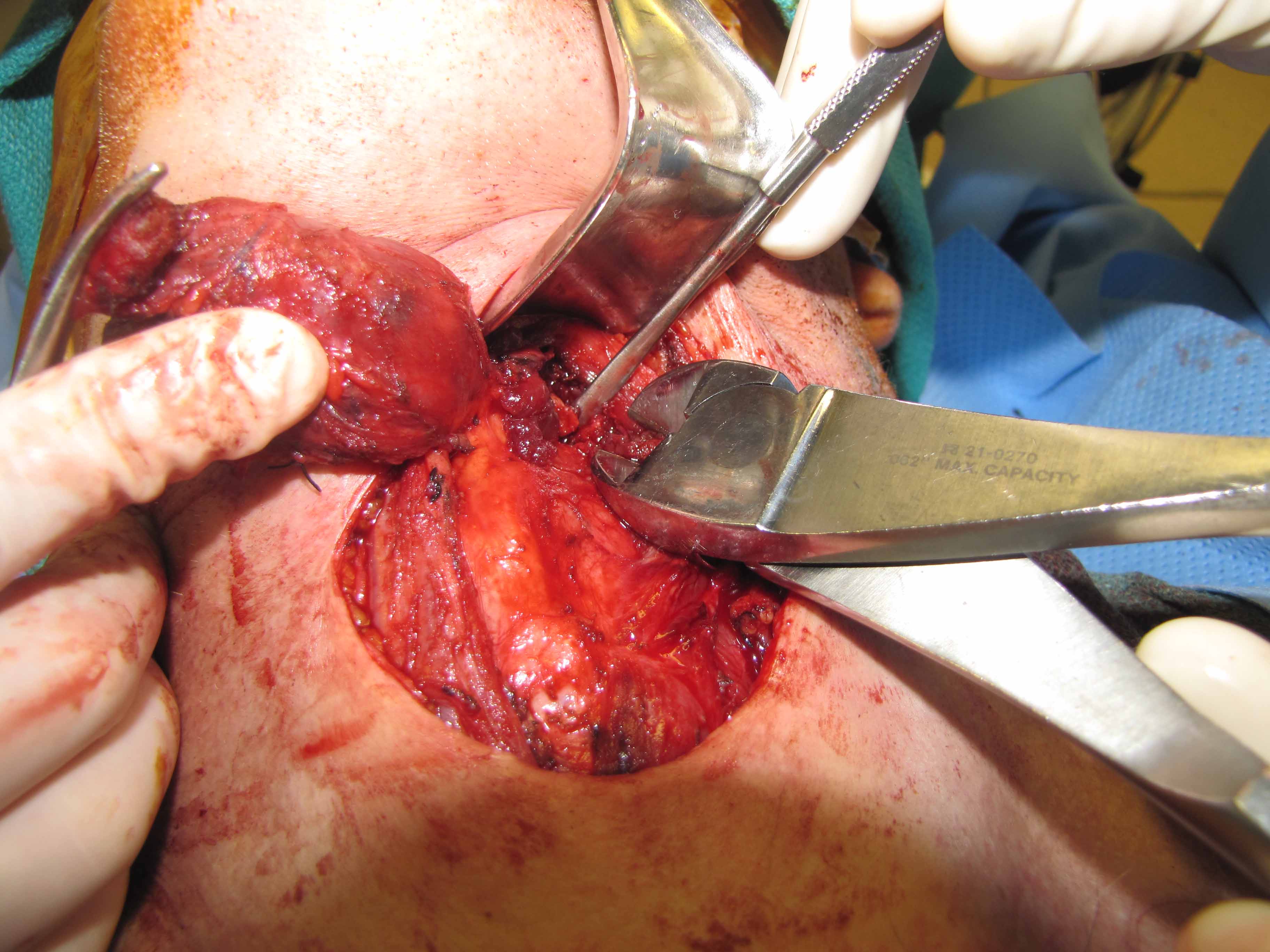
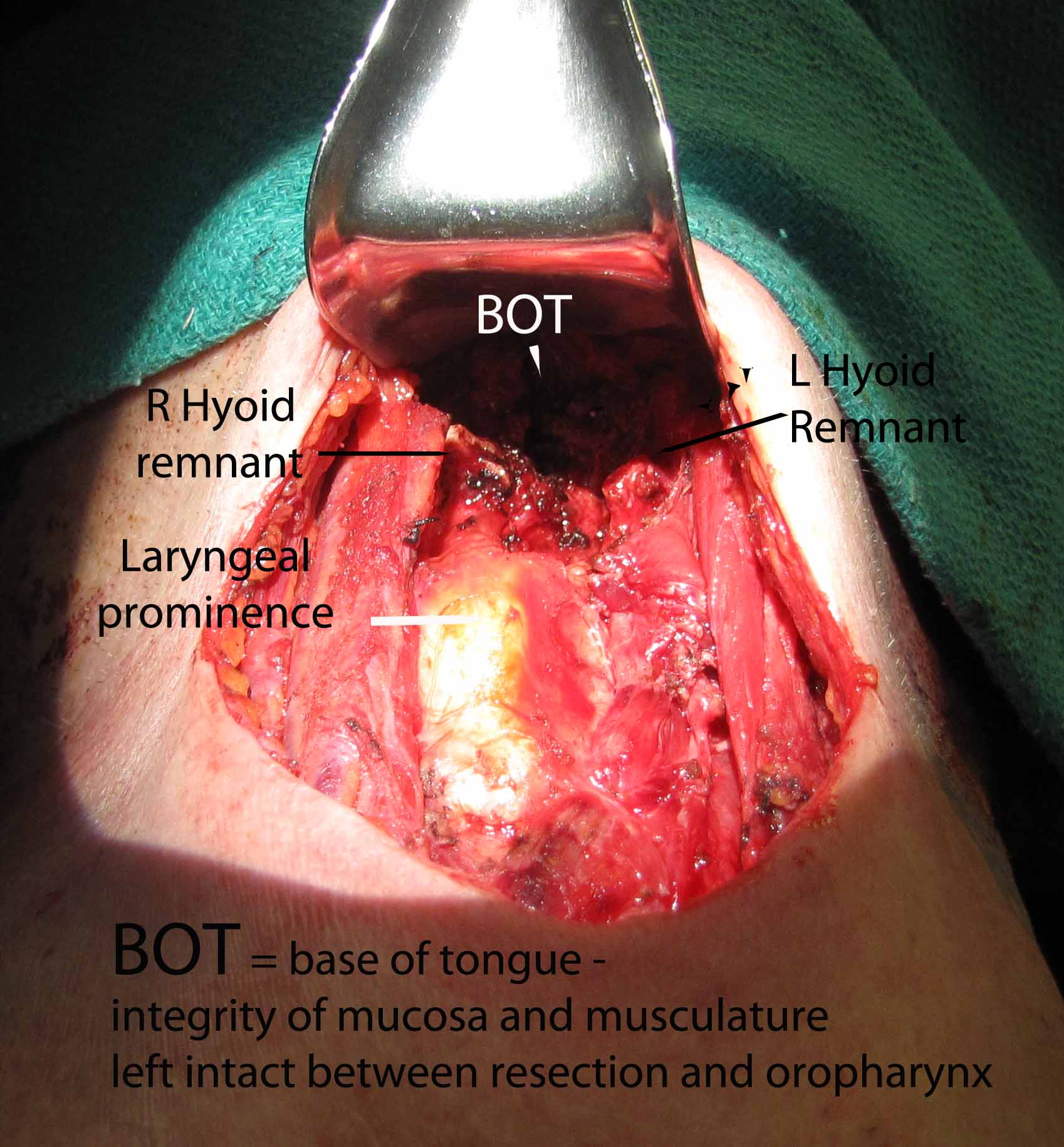
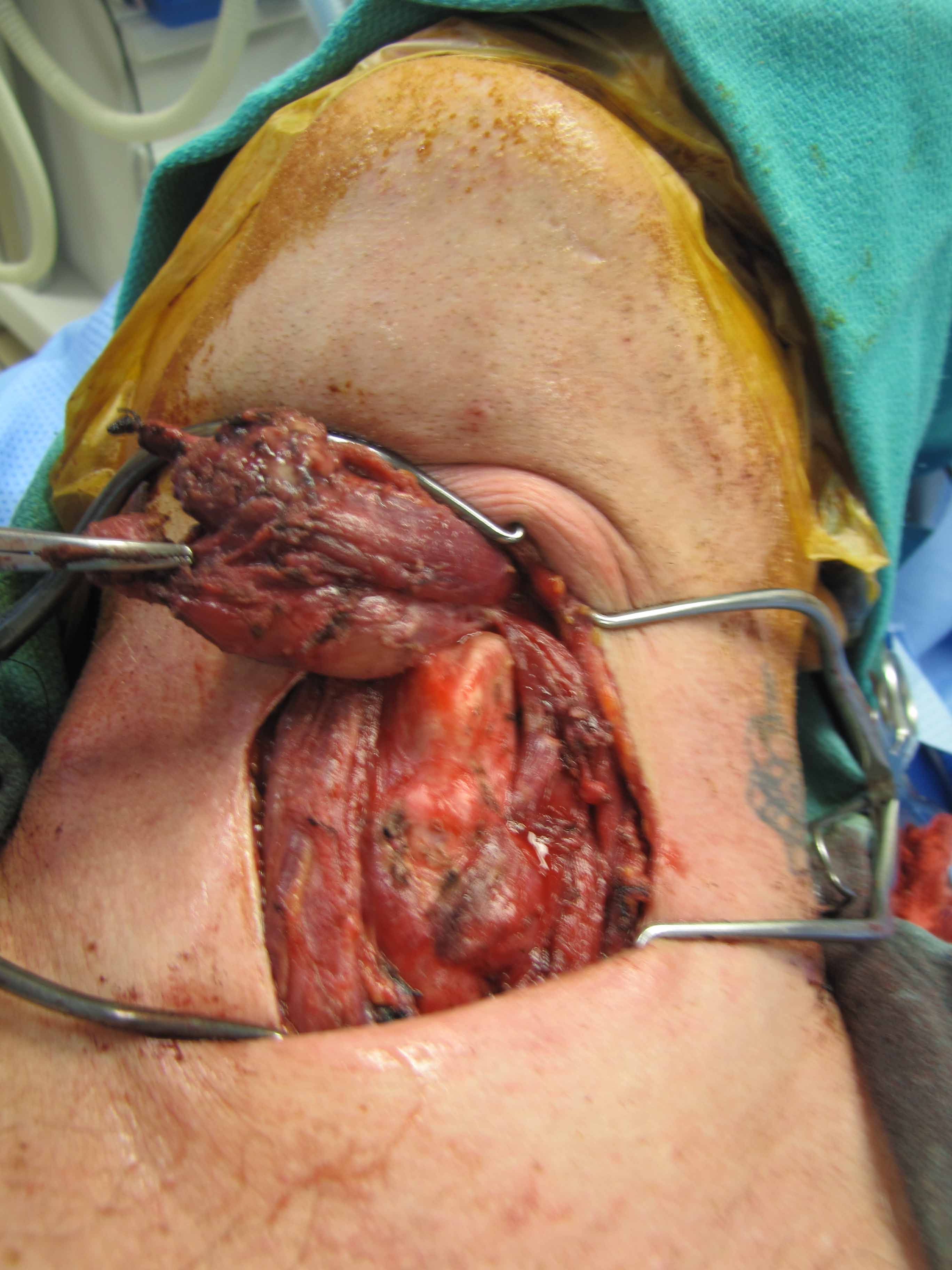
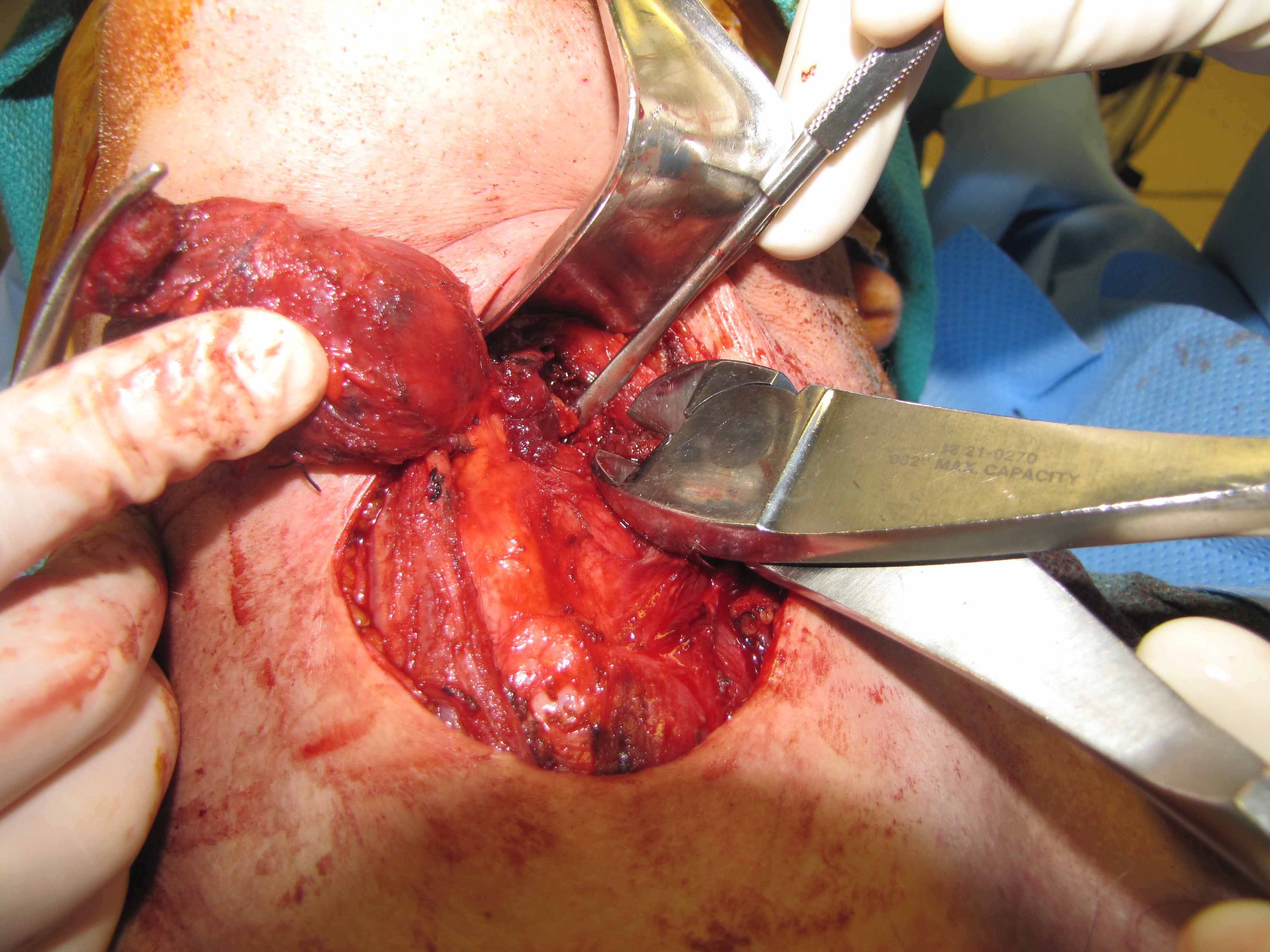
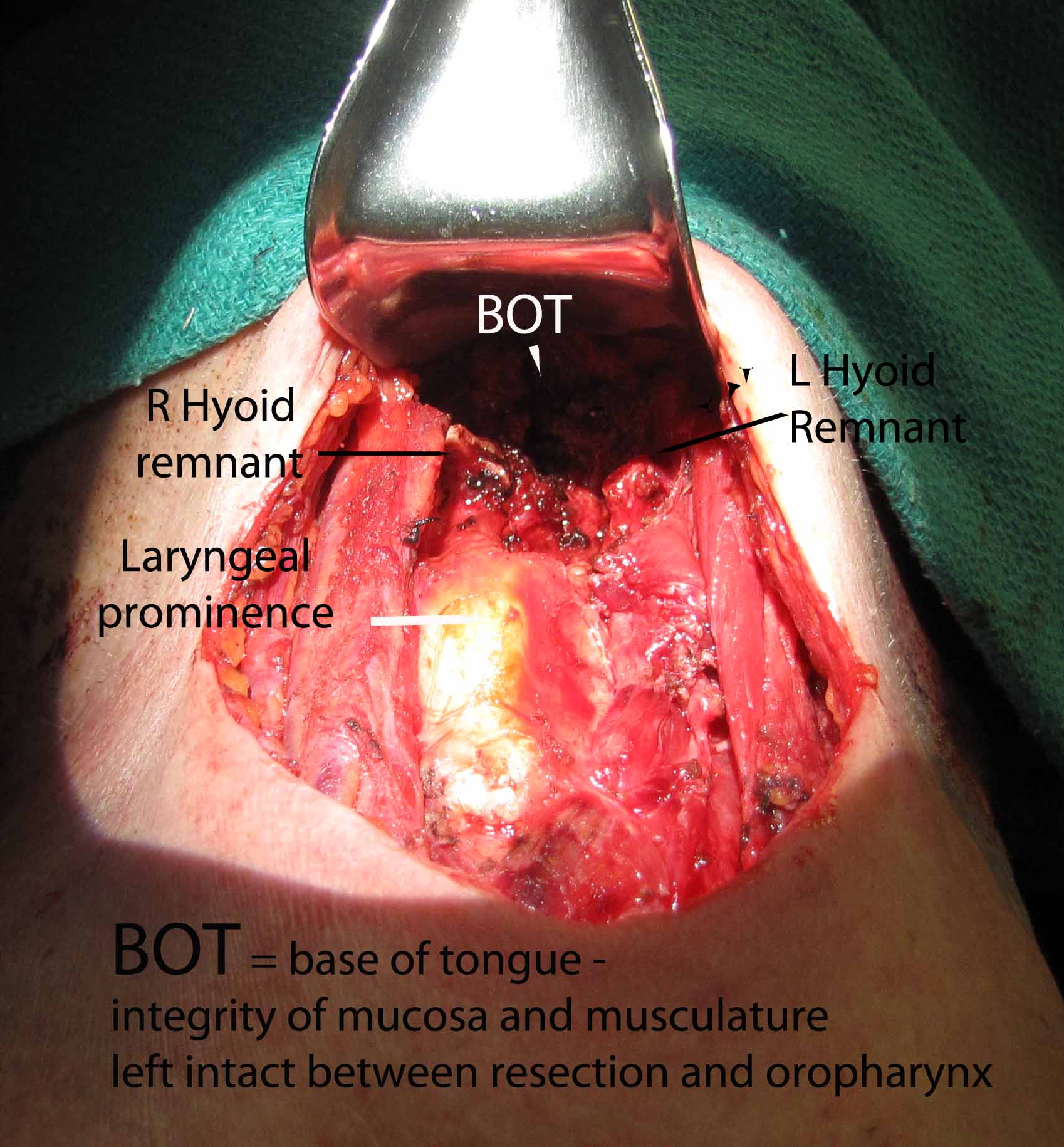
The hyoid bone was identified with preservation of soft tissue about the central portion and isolation of the bone laterally. On the right side, just medial to the lesser cornua and used a Freer underneath to protect while we released the hyoid with the mighty bite. The left side was addressed in identical fashion, except that we were lateral to the lesser cornua. The dissection was carried superiorly with a cuff of muscle.
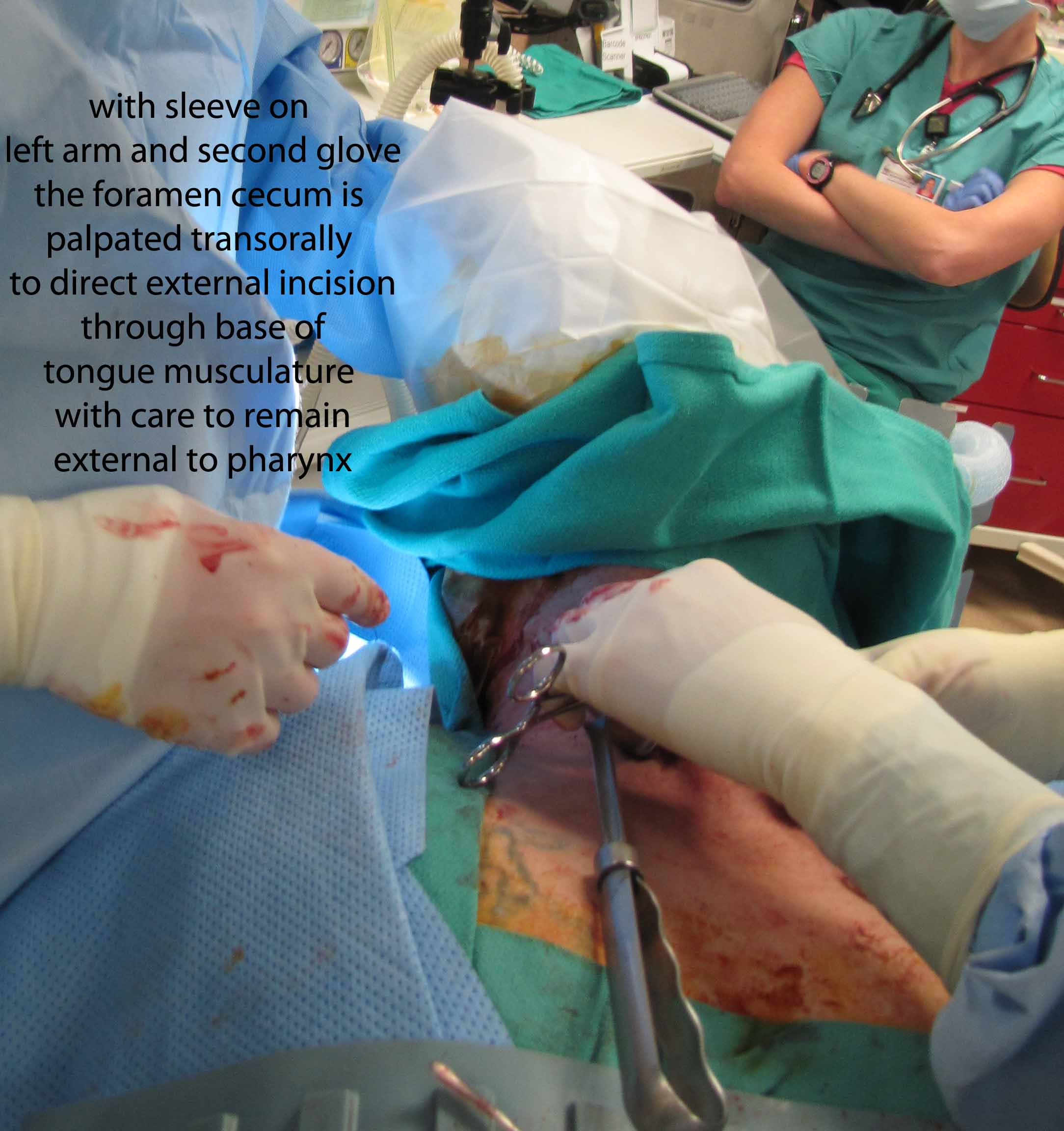
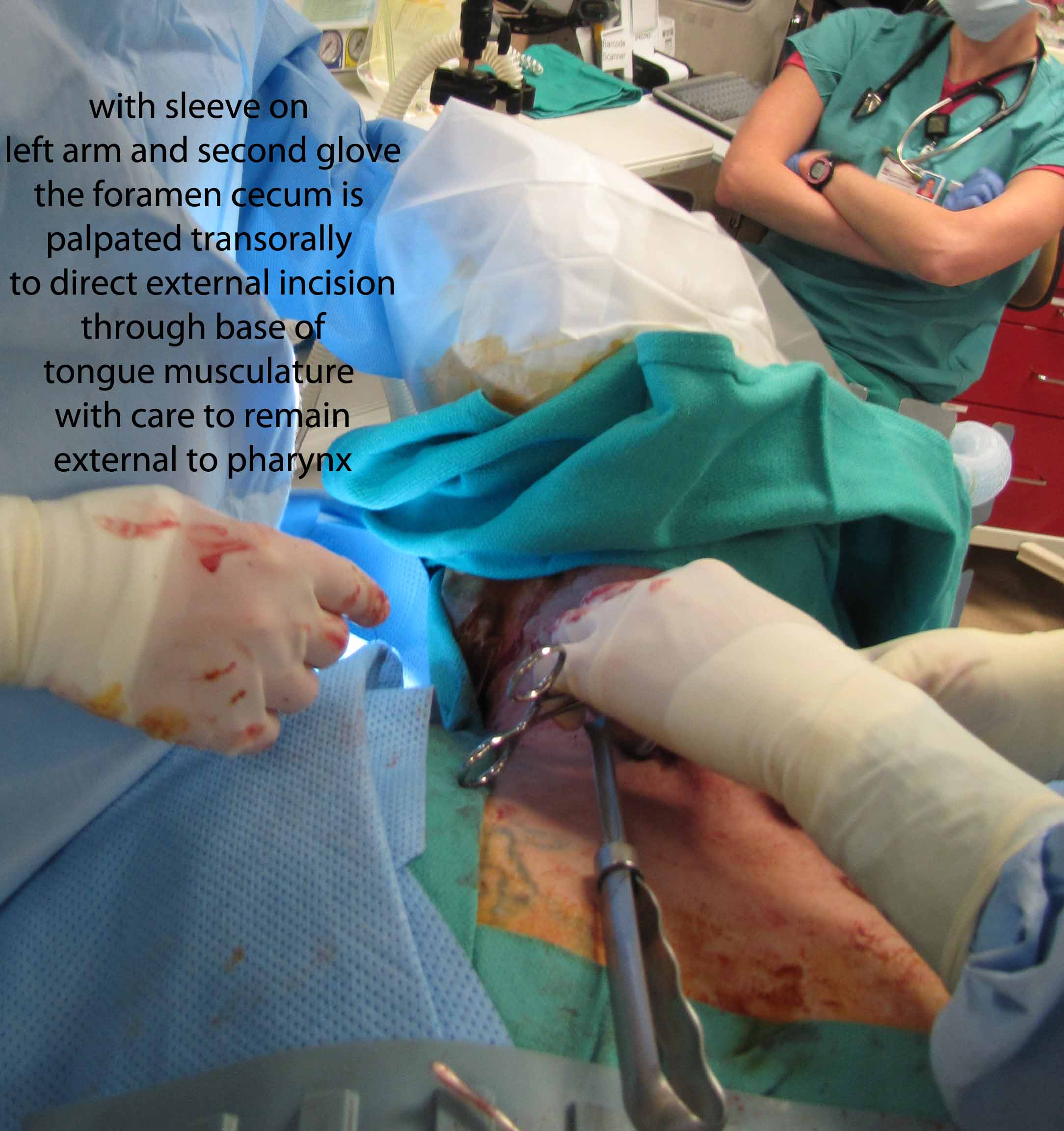
From above, surgeon reached into the mouth and palpated the foramen cecum with the left hand and arm protected with a sterile sleeve and second glove - placed to permit later removal from the contaminated oral cavity to permit continued sterile dissection in a sterile field. With anatomic control directed by palpation intra-orally with concurrent dissection of the open neck, clips were placed to mark the region of the undersurface of the base of tongue where the TGD cyst was to be severed. Final cuts with the bovie were similarly directed both by intra-oral palpation and extra-oral inspection.
Frozen section was taken from the superior most part of the tract - revealing no evidence of a tract. Had there been a tract identified, further dissection (potentially communicating intraorally) would have been done where the hemoclips had been placed above the hyoid (see also: Case example thyroglossal duct cyst with tract through to oropharynx.)
The defect was closed by approximation of tongue base musculature (with care to remain extra-oral) buried 3-0 Vicryl stitches. The strap muscles were reapproximated with 3-0 Vicryl stitches and the wound was copiously irrigated with multiple bulbs of irrigation with normal saline. The platysma was then closed with buried 3-0 Vicryl stitches. This was after a fully perforated Jackson-Pratt drain was placed in the wound and brought out centrally and secured with 3-0 nylon. The platysmal layer was closed with buried 3-0 Vicryl. The dermis was approximated with interrupted 4-0 Monocryl and then a subcuticular closure was performed with a running 4-0 Monocryl. Skin closure was supplemented with several interrupted 5-0 nylon stitches.

Followup 4 months postop