


Return to: Arytenoid Adduction Combined with Medialization Laryngoplasty through Type I Gore Tex Thyroplasty; Medialization Laryngoplasty- Type I Thyroplasty with ePTFE (Gore-Tex); Injection Laryngoplasty for Vocal Fold Paralysis and Glottic Incompetence
Modified Operative Note
Female with history of glomus tumor resected in July 2009. Since that time has had left vocal cord paralysis along with dysarthria (hypoglossal nerve paralysis) and velopharyngeal incompetence (palatal weakness).
Procedure Details:
After informed written consent was obtained, the patients identity confirmed and a brief time-out effected. The patient was placed in the supine position and monitors were placed. The patient was intubated with 4-0 MLT endotracheal tube.
We began with the direct laryngoscopy using an anesthesia MAC blade. Cords were visualized and the arytenoid was palpated to confirm its mobility on the right and left sides. Next flexible gastroscope was placed transorally with visualization of the glottis. This was taped in place with visualization of the glottis on the television screen throughout the course of the case. Next, the neck was prepped and draped in the usual sterile fashion with injection of 1% lidocaine, 1: 100,000 epinephrine along the planned incision.
Laryngeal landmarks were palpated and marked. A transverse incision just lateral to midline approximately 3 cm was made over the thyroid cartilage. Dissection exposed the strap muscle. The upper aspect of the left sternothyroid muscle was partially transected with the bovie. The perichondrium was sharply incised in the midline, and superior border permitting elevation of soft tissue from the left thyroid alar cartilage in a subperichondrial plane.
The oblique line was identified on the lateral aspect of the thyroid cartilage. The constrictor muscle was freed from thyroid cartilage. The posterior aspect of the cartilage was identified. Starting at the inferior aspect, the thyroid cornu was identified and medial blunt dissection curved around the posterior border of the cartilage (Padget and Woodson elevators) to ensure the dissection avoided entry into the piriform sinus.
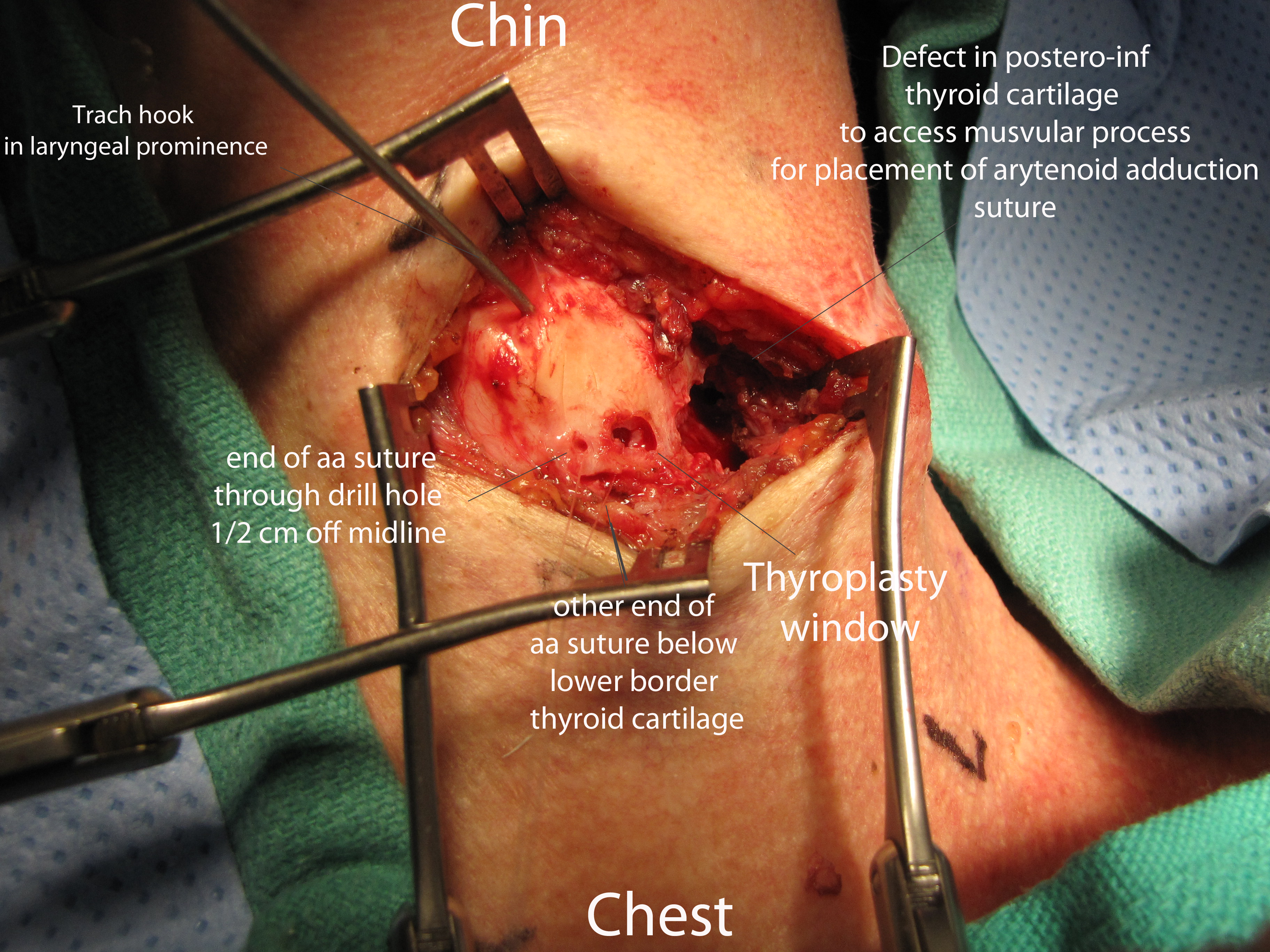
A Kerrison rongeur was used to remove portions of cartilage from the posterior aspect of the thyroid lamina with care to leave the attachment of the inferior cornu to the cricoid intact. The broadly based fan shaped PCA muscle was identified and traced supero-medially to its attachment to the muscular process of the arytenoid.
A 4-0 Prolene (or, in the example, clear nylon) suture was placed through the PCA muscle at its attachment to the muscular process. With superior traction on the two ends of the suture, a second pass was made with the needle through the muscular process with the figure of eight suture (two passes) tied.
The thyroplasty window was created with a small cutting burr. A second fenestration in the anterior thyroid cartilage was made 0.5 cm from the midline and 0.3-0.5 cm above the lower border with a #2 cutting burr (as low along the lower border of the cartilage as can reliably preserve a solid inferior strut).
A slightly bent Keith needle was placed retrograde through the small anterior fenestration, visualized through the thyroplasty window, and positioned adjacent the muscular process where the free end of the 'aa’ suture was threaded into the needle. The needle was then pulled forward delivering the suture through the fenestration.
The second end of the 'aa’ suture (still with needle attached) was placed (dull end first) into the thyroplasty window, then (sharp end first) under the lower border of the thyroid cartilage (through the cricothyroid membrane).
Alternate pulling and releasing on the two sutures demonstrated appropriate ab- and ad- duction of the vocal process seen on the video monitor.
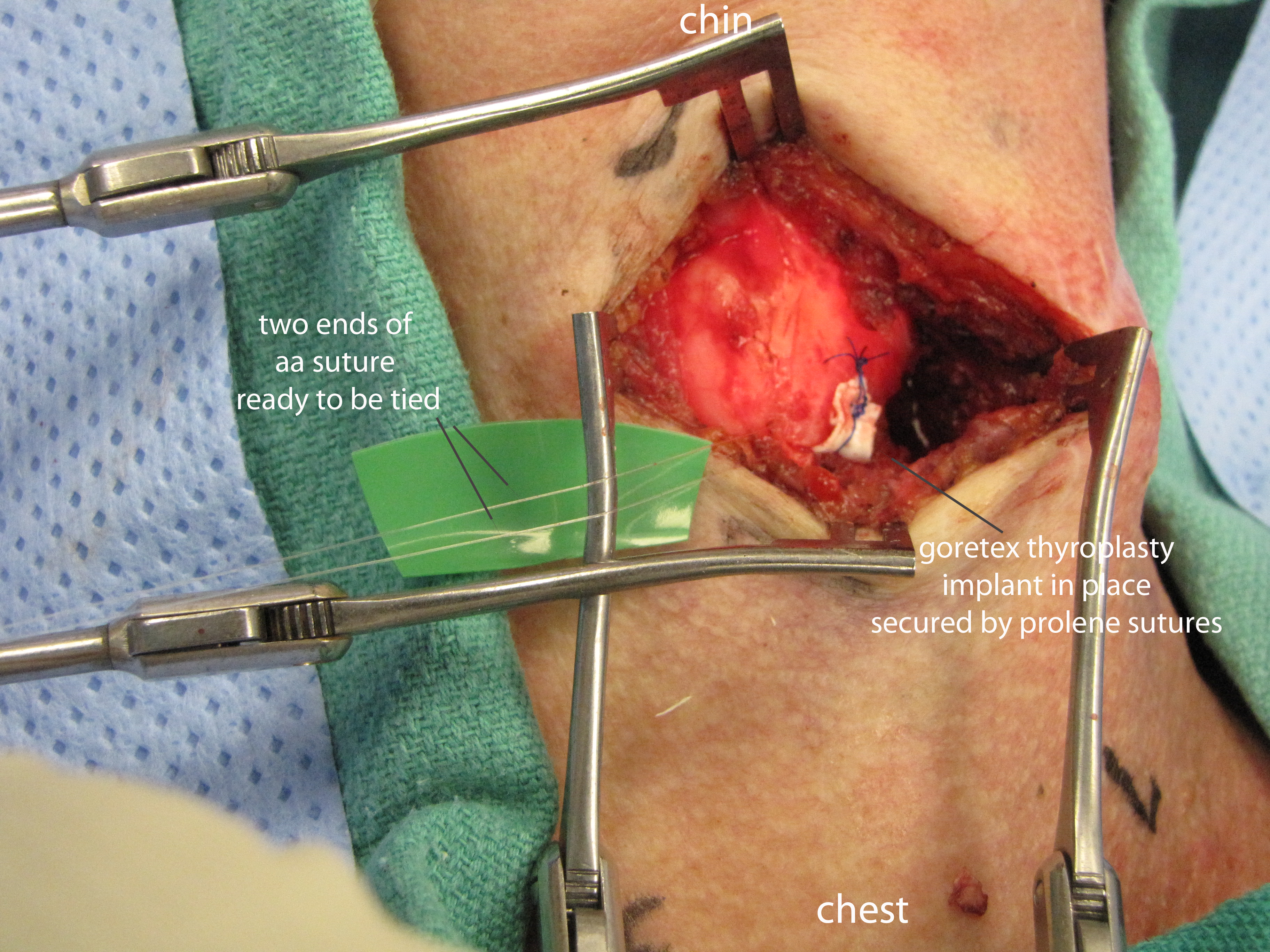
The Gore-Tex was placed in the paraglottic space through the thyroplasty window from an inferior approach and positioned (with visual monitoring of the vocal cord position) by manipulations with the sharp end of a Woodson elevator through the thyroplasty window. The implant was superficial (lateral) the the 'aa’ sutures.
The implant was then trimmed and was sutured in place with a 5-0 Prolene suture passed around through the implant around the lower border of the thyroplasty window. A second prolene suture was used to further secure the implant with placement through the thyroid cartilage above the window.
With direct monitoring via the esophagoscope, gentle traction on the 'aa’ suture ends then permitted tying them together.
Next, the area was washed with copious amounts of saline irrigation. The strap muscles were reapproximated with 4-0 Vicryl sutures. Deep tissue was reapproximated with 4-0 Vicryl sutures and a Penrose was placed to drain the wound. The skin was closed with interrupted 4-0 nylon sutures.
Next, our attention was turned back to the airway where the gastroscope was removed. Using a MAC blade to perform a laryngoscopy, we sprayed approximately 3 cc of 4% lidocaine onto the vocal cords as the patient was awakening and extubated her safely. She was an easy mask airway and she was transferred to the PACU in stable condition.
Videos pre/intra/post are below: