









Click on image above to enlarge; advance with cursor over border
Return to: Parotidectomy with Facial Nerve Dissection
Video below of post-op day 6 (weakness to marginal mandibular nerve) followed by postop 3 months showing resolution of lip weakness with all symptoms resolved on last followup 9 months postop
Modified Operative Note
Procedure: Left subtotal parotidectomy (including deep lobe) with facial nerve dissection and preservation with left level IIa selective neck dissection.
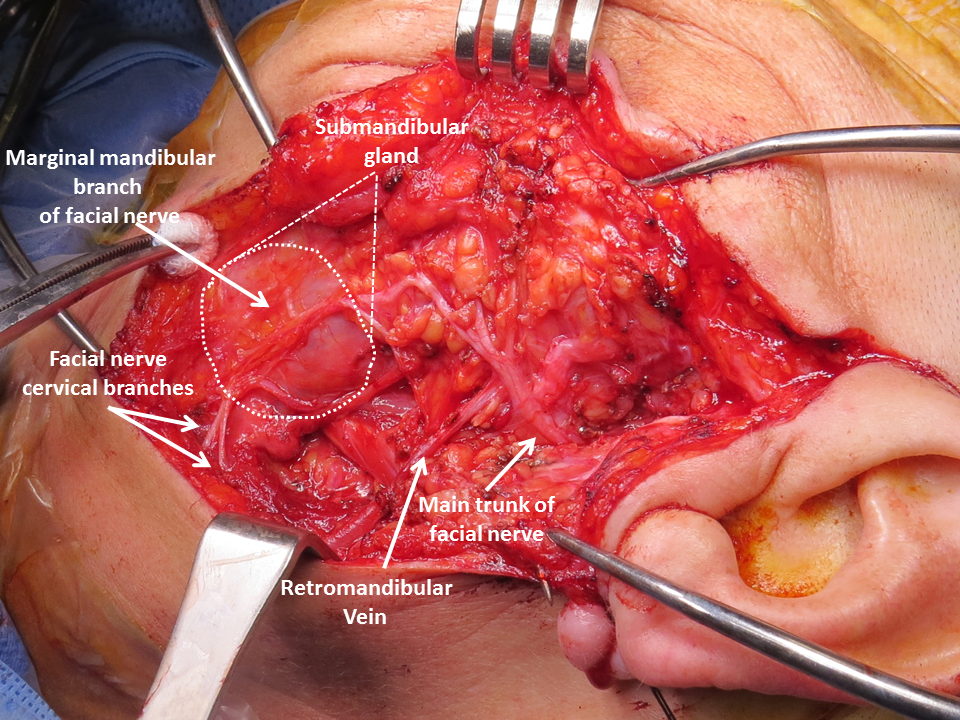
Findings: Large tumor encapsulated had displaced and elongated the facial nerve trunk inferiorly - addressed by retrograde dissection of the marginal mandibular nerve to pes then main trunk with tumor dissected (with a plan intact) off the upper division with overlay it
Tumor taken out with gross margins intact - the upper attachment to skull base (underlying posterior zygoma) was firm and a frozen section taken showing the margin to be clear but close with multiple carcinoma forms within compressed parotid tissue and more bland (pleomorphic adenoma-like) tumor - including squamous cell carcinoma appearing - but, as per pathology, deferring to permanent section - the potential for it to represent 'carcinoma in situ' in carcinoma-ex-pleomorphic adenoma thought possible hence effects to more conclusively confirm clear marings involved sending for permanent section a region marked with hemoclip 'deep lobe above main trunk' (marked again with large hemoclip) - which would represent the most inferior of the hemoclips placed (one at skull base where other frozen section analysis taken) with two other hemoclips placed on veins.
Estimated Blood Loss: None/Minimal
Modified Operative Report:
Informed consent was reviewed and the patient was brought to the operating suite. After general anesthesia with endotracheal tube placement (requiring video assisted 'glide-scope' for exposure of anteriorly positioned larynx) the table was turned with the head 180 degrees away from anesthesia. NIMS facial nerve monitoring was set up at this point and used for the duration of the case. The proposed injection site was injected with 6 cc of 1:100,000 epinephrine. The patient was prepped and draped employing an incise drape to separate the mouth and nose from the surgical field but maintain view of the entire hemi-face.
A modified Blair incision was made with a slight anterior extension with a scalpel through the dermis with incision of the platyma permitting identification of the marginal mandibular nerve overlying the submandibular gland (employing facial nerve stimulator to assist).
Retrograde dissection of the marginal mandibular nerve was initiated to identify the facial nerve anterioriorly away from the tumor mass that had modified the location of the upper division and pes. he tail of the parotid gland was separated from the anterior border of the sternocleidal mastoid muscle using the Shaw hemostatix scalpel (220 degrees) with identification and preservation of the external jugular vein and the greater auricular nerve - requiring sacrifice of the anterior branches of the great auricular nerve with preservation of the posterior branches.
Dissection anterior to the superior sternocleidomastoid muscle identified the posterior belly of the digastric muscle. The fascial attachments between the parotid gland and the cartilage of the EAC were divided (employing loup magnification) to mobilize the parotid gland.
Due to the large size of this parotid tumor adjacent the pes anserinus and main trunk, we returned to retrograde dissection of the facial nerve in anticipation of distorted anatomic relationships of the facial nerve location due to tumor near the trunk of the nerve.
Continued retrograde dissection of the marginal mandibular nerve permitted its separation from the tumor without violating the capsule leading to safe exposure of the pes anserinus along with a superior divisions. Deformation of the main trunk of the facial nerve was observed (elongated and displaced inferiorly) persumably due to the tumor's mass-effect.
The tumor was separated from the facial nerve with mobilization of the upper division overlying the tumor with sufficient space to access the tumor facilitated by the elongated nature upper division (presumably longer than standard due to slow continued tumor growth).
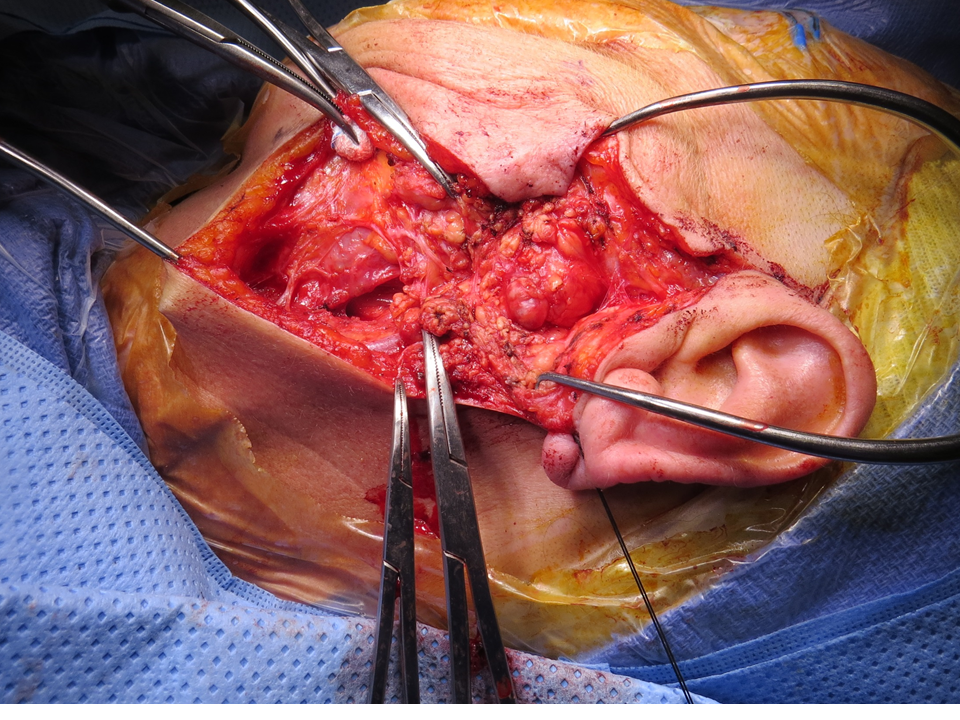
Following dissection and preservation of all branches of the facial nerve we divided the fascial attachments of the deep lobe of the parotid to the parapharyngeal space using bipolar cautery and excised the tumor.. At its attachment to the skull base, on the undersurface of the posterior zygoma, a cuff of healthy feeling parotid tissue was left in place. However, on the specimen the tissue was firm and for this reason biopsy was taken from the specimen for frozen section. This was positive for pleomorphic adenoma. After further resection of a cuff of parotid tissue (sent for permanent pathology) a hemoclip was placed as a marker.
At the completion of the parotidectomy, we stimulated the nerve at 2 mA and noted complete movement of the face.
Next we performed a level IIa neck dissection. We dissected several lymph nodes away from the external jugular vein and included them in her resection. Level 2A was resected by skeletonizing the posterior belly of the digastric muscle and anterior border of the sternocleidomastoid muscle with the Shaw hemostatix scalpel. We bluntly dissected down to the floor the neck. We bluntly dissected to identify and skeletonized the spinal sensory nerve. The lymph node packet was elevated off of the floor the neck and andterior to the spinal accessory nerve using blunt dissection and bipolar cautery. The specimen was excised and sent for permanent pathology as a level 2a.
The wound was copiously irrigated with saline. Hemostasis was verified with Valsalva maneuver. A # 10 mm fully perforated Jackson-Pratt drain was placed through the skin of the posterior neck flap and into the area of the neck dissection. Closure of the wound was effected - the platysmal layer and SMAS layers were reapproximated using interrupted Vicryl suture. The skin was closed with a 4-0 running nylon suture on the neck and a 5-0 running nylon suture on the face.
Prior to leaving the operating room a pressure dressing was placed over the wound. The patient tolerated this procedure well without complication.
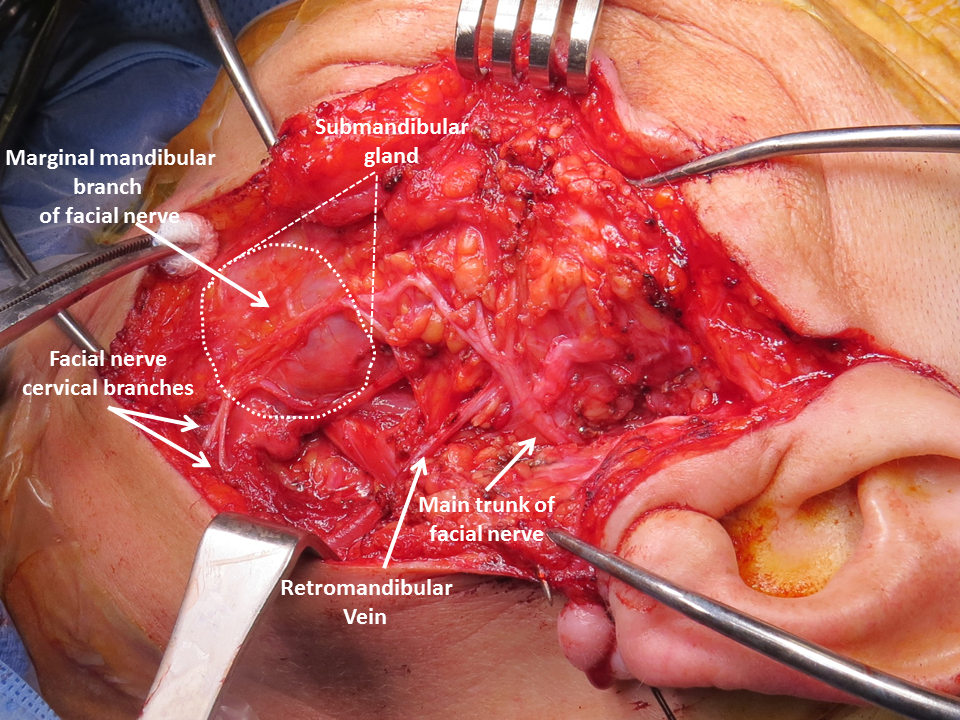
Note the variability in anatomic relationships between the retromandibular vein and facial nerve. As per Mahore et al (Mahore 2018), the retromandibular vein has been reported as passing lateral to the facial nerve in 12.5% of cases with other anatomic studies identifying the retromandibular vein lateral to the facial nerve in 17% (Kim 2009), 28% (Toure 2010), and 10% ( Kopuz 1995). In rare cases the facial nerve may be encircled by a venous ring formed by the retromandibular vein.
References
Mahore D, Mangalgiri AS, Namdev LN, Kapre M.Variations of Retromandibular Vein and Its Relation to Facial Nerve Within Parotid Gland. Indian J Otolaryngol Head Neck Surg. 2018 Sep;70(3):395-397. doi: 10.1007/s12070-018-1389-1. Epub 2018 May 8.
Kim DI, Nam SH, Nam YS, Lee KS, Chung RH, Han SH The marginal mandibular branch of the facial nerve in Koreans. Clin Anat 22:207–214 (2009)
Toure´ G, Vacher C (2010) Relations of the facial nerve with the retromandibular vein: anatomic study of 132 parotid glands. Surg Radiol Anat 32:957–961
Kopuz C, Ilgi S, Yavuz S, Onderog˘lu S (1995) Morphology of the retromandibular vein in relation to the facial nerve in the parotid gland. Acta Anat 152(1):66–68