return to: Injection Laryngoplasty for Vocal Fold Paralysis and Glottic Incompetence; Cymetra Injection to Paralyzed Vocal Cord In the Clinic Technical Points for Percutaneous Injection; Injectable substances for injection laryngoplasty
see also: Laryngeal Needle Localization with Transillumination; Transilluminating Obturator
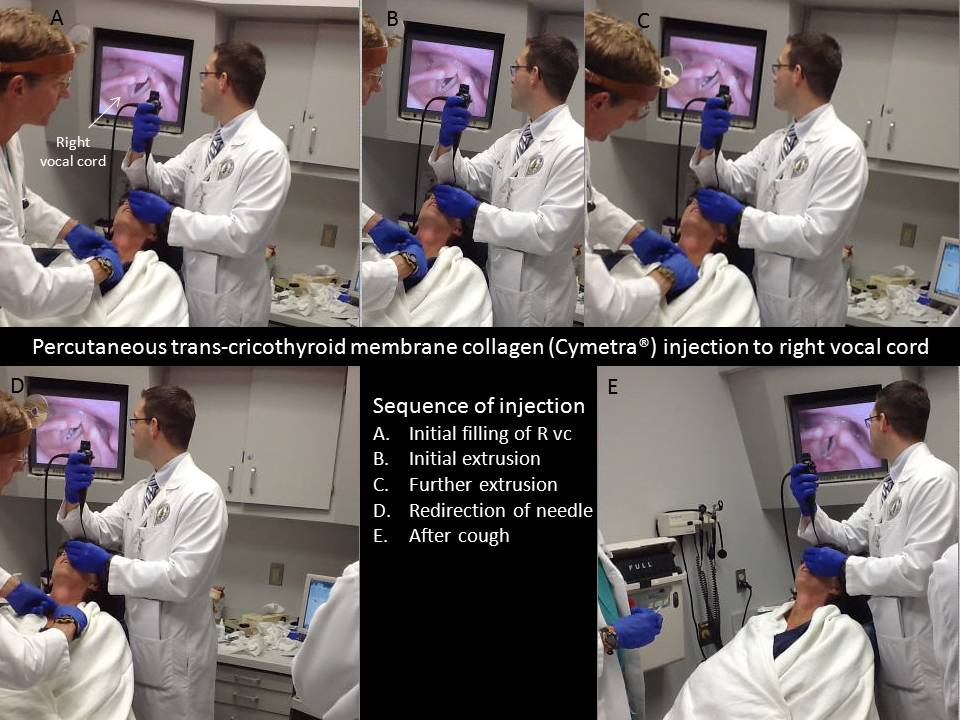
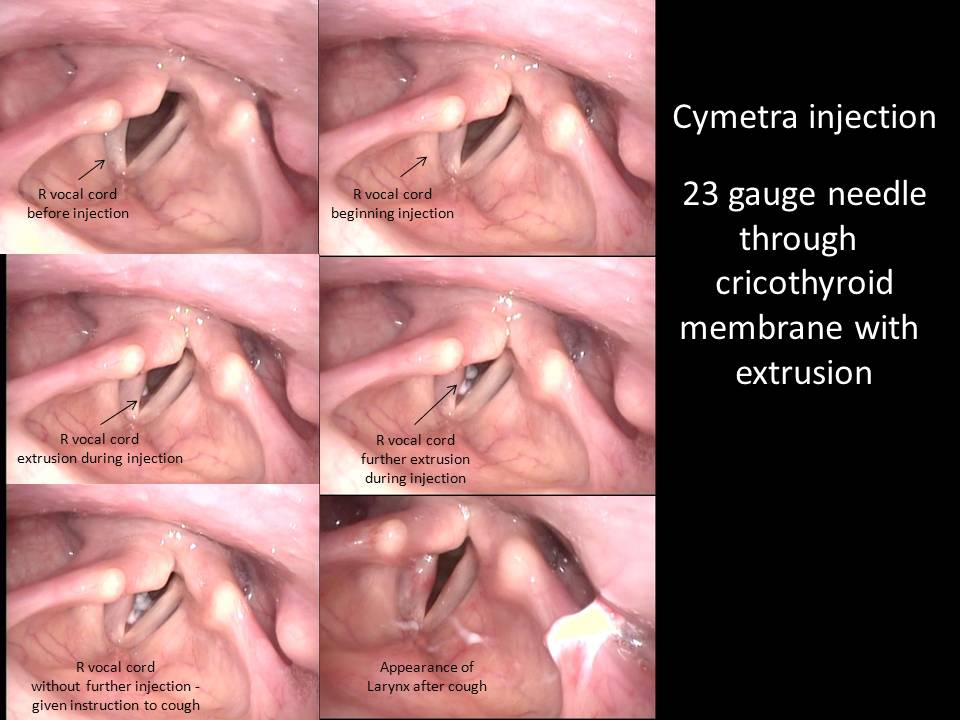
An effective way to access the paraglottic space, Reinke's space, and the muscles in between (thyroarytenoid = TA and lateral cricoarytenoid = LCA) is a percutaneous technique through the cricothyroid membrane. Experience in palpating landmarks makes this approach useful for botox injection (with location confirmed by EMG) and for injection of the 'forgiving' substances such as collagen - wherein precise localization of the needle tip before injection is not mandatory. Other injectables (ie calcium hydroxy apatite) may require more precise needle tip location to prevent extrusion of material or its localization into undesirable areas (ie Reinke's space). The case portrayed identifies a favorable result despite extrusion of collagen – a 'forgiving substance' - that tends to be molded into appropriate location during the process of laryngeal closure. Further refinement to accurately position the needle tip in the course of injection laryngoplasty may be offered by the technique of transillumination (see: Transilluminating Obturator).
Still images of injection to paretic (small amount of arytenoid movement) right vocal paralysis followed by video demonstrating preop voicing, injection, and postop results:
Transnasal imaging of right vocal cord paralysis treated with Cymetra injection |
|
|---|---|
|
|
Video below shows sequence following April 2 2013: Thyroidectomy
Sept 12 2013: Voice Clinic Evaluation (G2R0B2A2S0) (5 months after thyroidectomy)
Oct 1 2013: In-clinic percutaneous Cymetra® injection
April 24 2014: Voice Clinic Evaluation (G0R0B0A0S0) (7 months after injection; 12 months after thyroidectomy)
Click to play video:
Modified Operative Note
PREOPERATIVE DIAGNOSIS:
Right vocal fold paralysis with dysphonia.
POSTOPERATIVE DIAGNOSIS:
Right vocal fold paralysis with dysphonia.
PROCEDURE PERFORMED:
Transnasal fiberoptic laryngoscopy with concurrent percutaneous transcricothyroid membrane, injection laryngoplasty with Cymetra (0.6 mL instilled, estimated 0.35-0.4 mL retained).
ANESTHESIA:
Topical to the nose Afrin followed by lidocaine Neo-Synephrine, 1% lidocaine with 1:100,000 epinephrine in the skin overlying the cricothyroid membrane. Premedication with Augmentin.
DESCRIPTION OF THE PROCEDURE:
Following identification of the patient and informed consent, Cymetra was diluted with 1% lidocaine plain with 1.7 mL of lidocaine with the packet of Cymetra® (lot number B495578). The patient was positioned semisupine with a fiberoptic scope placed anteriorly for transnasal imaging of the larynx and then handed to the resident standing behind her to allow access to the neck, which was wiped clean with an alcohol swab with a 23-gauge slightly bent needle placed percutaneously through the cricothyroid membrane with initial injection showing initial filling in ideal mid membranous spot with further instillation identifying some extrusion in the subglottis allowing for replacement of the needle and further instillation to a volume of 0.6 mL (estimated 0.35-0.4 mL retained). The patient was observed in clinic for a half hour afterwards with repeated exams and discharged home with followup targeted in 6 months with the Voice Clinic with the understanding an earlier visit a call from her if she wished to have a repeat injection or an alternative therapy offered.
Click to see video of voice 10 minutes after injection:
Click to open example of Cymetra injection extending outside vocal cord: