
Click on image to enlarge advance with cursor over right border |
|---|
return to: Laryngeal Fracture Plating
Modified Operative Note
Oto Staff Note
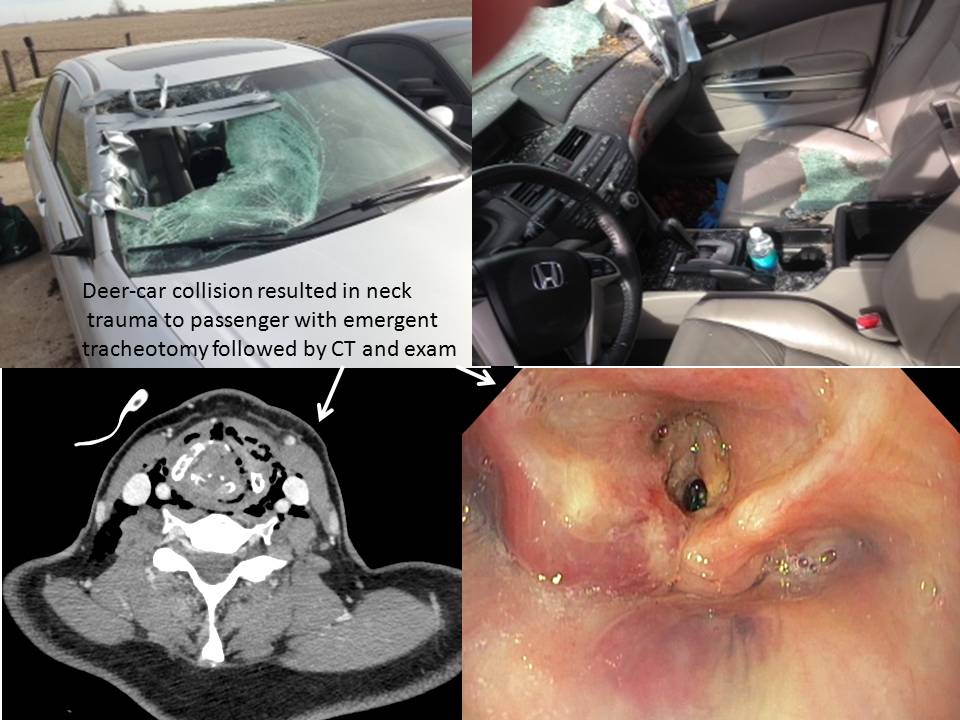
I met with Ms X, her husband and her son as well as her chaplain in the SICU at 12:45 before her transfer to the OR. I related I had conferred with Dr. X, Dr. Y and Dr. Z about her clinical course which her husband was able to identify as well: a deer came through the windshield of the car he was driving with her in the passenger seat - striking her neck and right hand - without significant injury to him. She was immediately hoarse and had progressive difficulty in breathing warranting the ambulance trip to the UIHC and 'class A' transfer to the OR where an emergency tracheotomy was performed under local anesthesia.
I related to them that I reviewed her CT and offered a likely scenario (pending confirmation with Dr. X) of microdirect laryngosocpy, possible endoscopic suturing, possible stent placement, possible open approach to the fracture, with potential for NG tube placement with esophagoscopy. I reiterated the indications, technique alternatives and risks to the aforementioned and all affirmed they understood and wished to proceed. I also related potential need for future interventions."
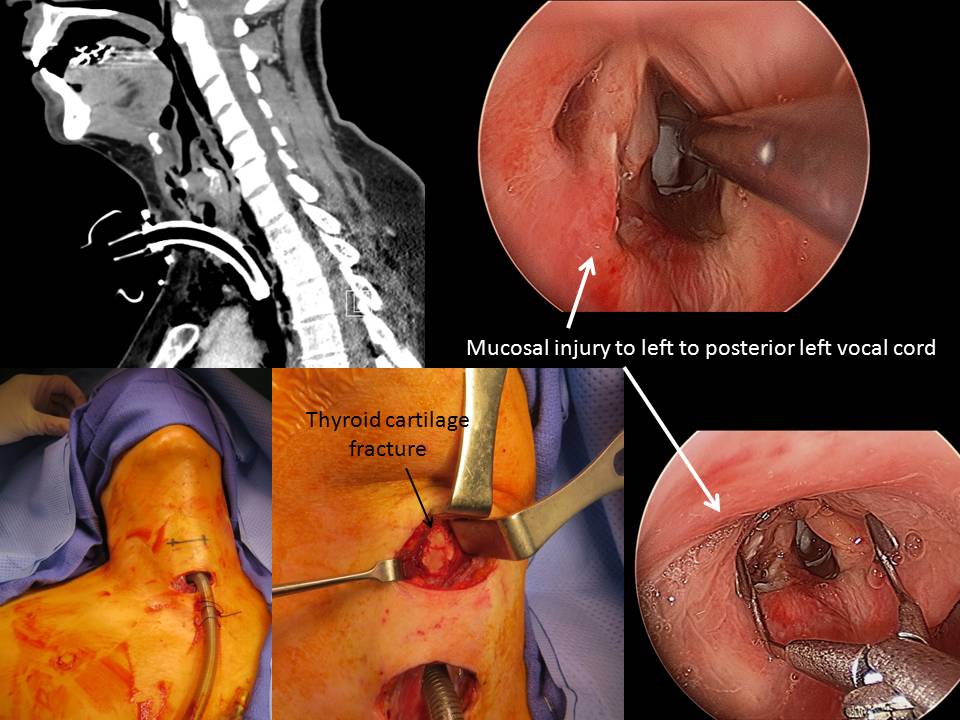
I conferred with Dr. C (radiology) on the phone after our initial microdirect laryngoscopy. We concurrently viewed thin cut axial images of the larynx over EPIC - identifying difficulty in clearly delineating the difference between un-ossified thyroid cartilage and disruption in the cartilage (fracture) - he identified an inbuckling of the left thyroid ala near the midline with a likely fracture that warranted exploration with likely reduction and fixation.
Staff Op Note
Preop Dx: Airway obstruction from blunt laryngeal trauma requiring emergent tracheotomy last evening now with CT evidence of thyroid cartilage fracture
Postop Dx: Same
Procedure: Microdirect laryngoscopy
Esophagoscopy
Placement of NG (dobhoff) tube
ORIF laryngeal fracture (thyroid cartilage)
Surgeons: A,B,C
Anesthesia: General via pre-existing tracheotomy
Findings:
MicroDL: base of tongue, valleculua epiglottis posterior pharynx normal
right vocal cord with volitional movement (seen before full relaxation administered)
Left arytenoid edematous - similar volitional movement not seen, but both right and left arytenoids mobile to palpation w/o evidence for dislocation or subluxation
Right FVC with abrasion extending to involve posterior dorsal left vocal cord
Membranous vocal cords edematous but o/w normal with intact anterior commissure
Subglottis down to tracheotomy unremarkable
Esophagoscopy: unremarkable
Neck exploration: midline approach separating straps identified three-part displaced fracture addressed with elevation of posterior segment to approximate edges - KLS drill from 1.5 plating system used to place drill holes in each of the segments then approximated with placement of 2-0 prolene (use of retrograde keith needle technique) with ties between sutures coapting each of the segments.
Penrose drain placed. Photos as per above.