








Complication From Lip Biopsy for Sjogrens with Mucocele Formation (Granulation Tissue); Plunging Ranula Transoral Resection (Sublingual Gland) Aided With Sialendoscopy with Histopathology; Therapeutic Agents for Oral Mucosal Disease Treatment Strategies
Pemphigus vulgaris of the larynx, pharynx, and oral cavity; Bechet's Syndrome (Neuro-Beçhet) Rythmic Myoclonus Laryngeal - Pharyngeal
protocol by Eyas Alzayadneh, Chris Jensen, and Henry Hoffman (initiated Feb 2023)
Definitions
Confusing terminology (mucocele vs mucus retention cyst) - 'extravasation versus retention':
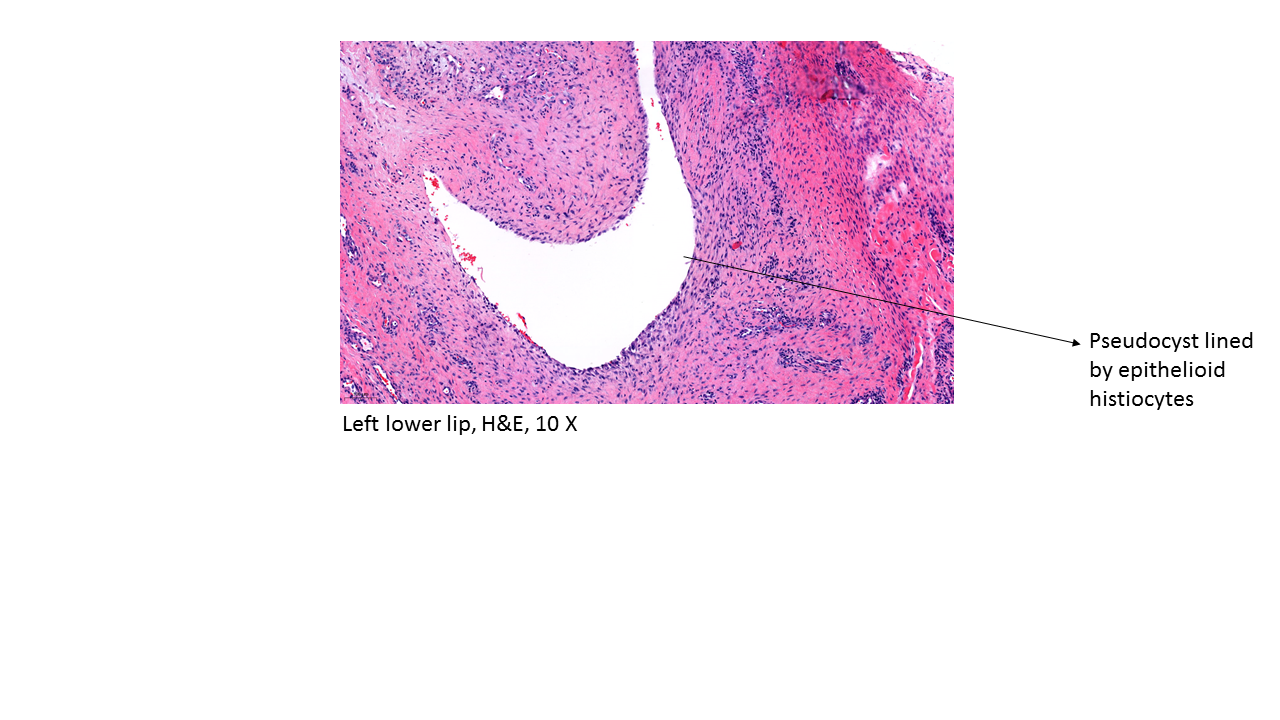
- Mucocele: lesion resulting from the rupture of a duct of the salivary gland with extravasation ('spillage') of mucus into the surrounding connective tissue without an epithelial lining (Chi 2010)
- Mucoceles represent a "mucus excape reaction" and "mucus extravasation phenomenon" (Miranda 2022)
- Mucus retention cyst (also known as "sialocyst" or "mucus duct cyst" are cysts lined by salivary ductal epithelium (Chi 2010)
- Mucus retention cysts develop from mucus buildup behind blocked glandular ducts - more commonly in cheek (buccal) or palate areas (Bowers 2021)
Background
Symptoms:
- Lower lip mucoceles are frequently asymptomatic but can be attended by interference with chewing, eating, and speech as well as altering cosmetic appearance (Bowers 2021).
Prevalence:
- Barros et al through a 10 year retrospective review ending 2016, 587 lip lesions (of which 76% occurred on the lower lip) - identified in a single institution in Brazil were identified - with mucocele being the most common diagnosis (25% of cases) (Barros 2020)
Etiology:
- mucoceles rare in upper lip with Chi et al contemplating that the cause for this discrepancy is due to a greater number and density of salivary glands in lower lip - combined with greater force applied to the lower lip along with "parafunctional habits" such as lip biting (Chi 2010)
- 'constant trauma' to the lower lip was implicated by Barros et al as a cause for the frequent occurrence of mucoceles (Barros 2020)
- 'damage to minor salivary glands or ducts' (Bowers 2021)
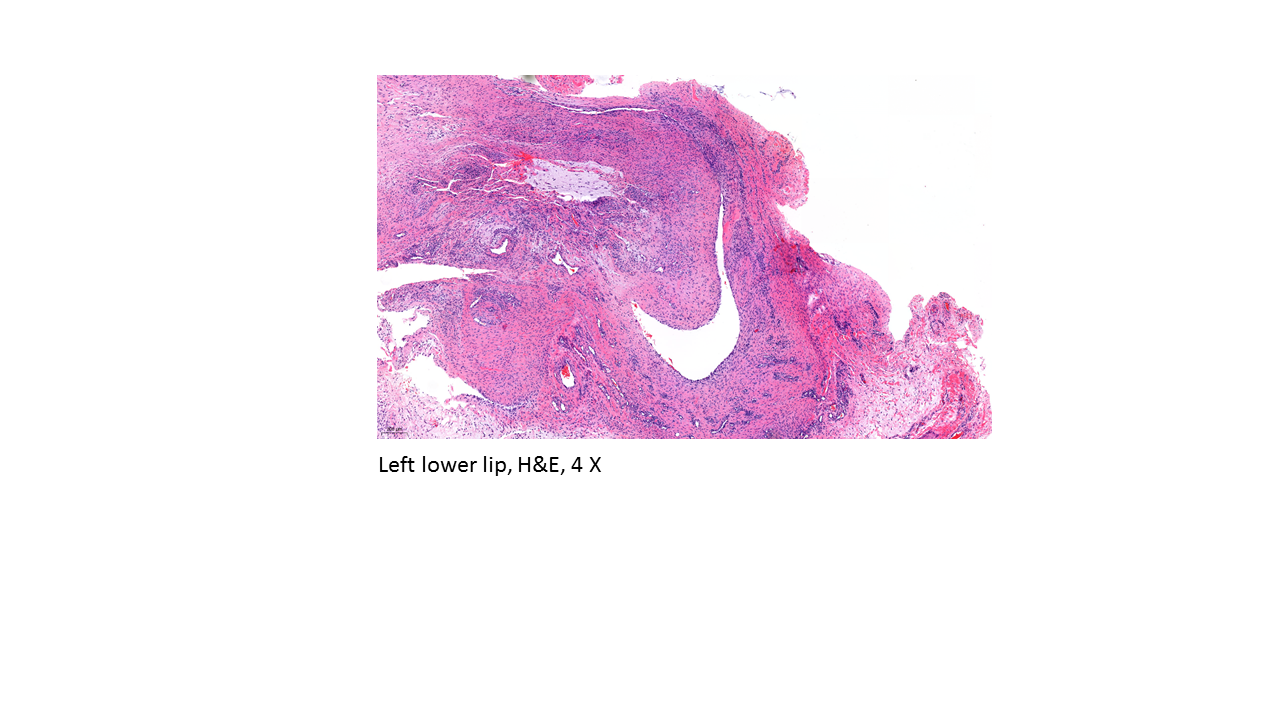
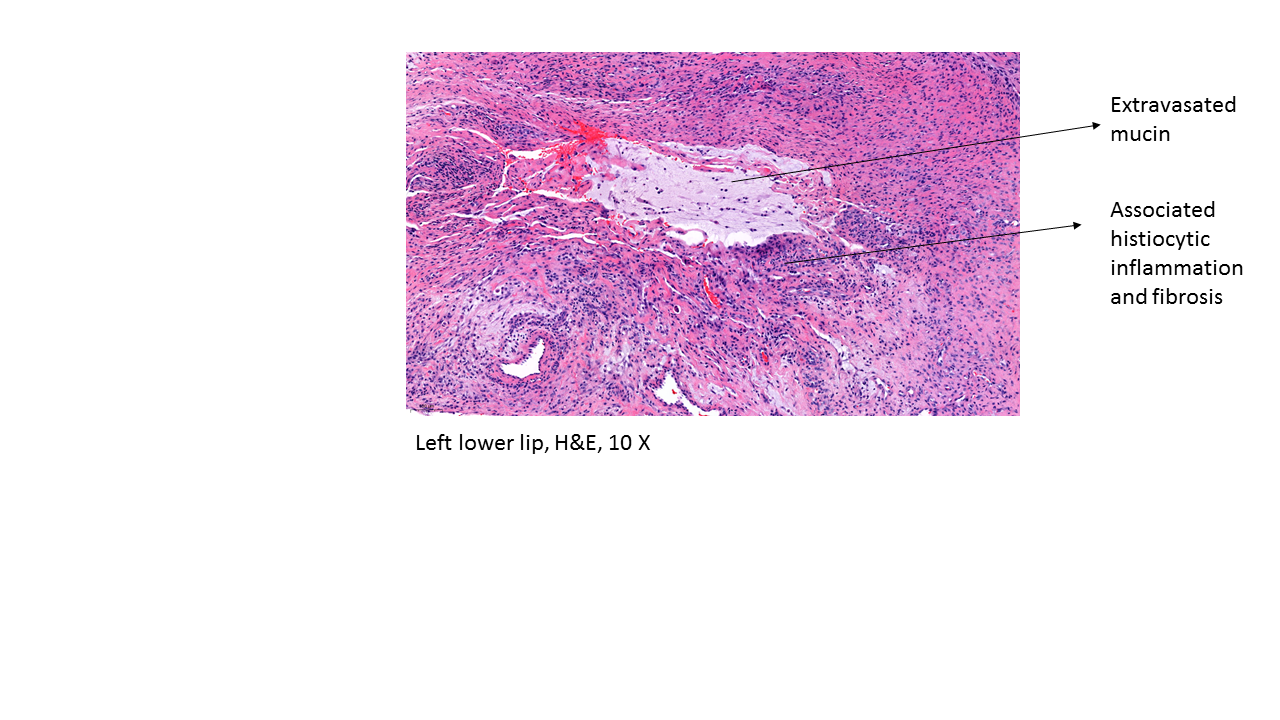
Histopathology: mucus extravasation ('spillage') with and associated inflamed granulation tissue response - without an true cystic epithelial lining
- variants reported: mucoceles with myxoglobulosis ('collagenous spherulosis'); mucoceles with papillary synovial metaplasia-like change
Differential Diagnosis of Lower Lip Lesions:
- mucocele, traumatic fibroma (tissue tag); papilloma; pyogenic granluoma; hemangioma, varix (vascular lesion); nonspecific inflammation/irritation; lichen planus; lymphangioma; nevus; neoplasm; vsiculobullous condition (Chi 2010)
- reactive/inflammatory lesions (including mucocele) (43.4%); infectious lesions (2.7%), benign neoplasms (5.6%), malignant neoplasms (3.6%), oral potential malignant disorders (33.1%), other (11.6%) in a study by Barros et al (2020)
Management of lower lip mucoceles
- observation without intervention; surgical excision with removal of minor salivary gland; marsupialization; 'micromarsupialization" (Delbem 2000), CO2 laser ablation, cryotherapy, intralesional steroid injection (reported to have high rates of recurrence by Bowers and Schaitkin 2021), sclerosing agents
- potential complications from surgical treatment reported: lip disfigurement, damage to adjacent minor salivary gland ducts ('recurrence'), lip numbness and scarring
Case Example: Clinical Course and Histopathology
Presentation:
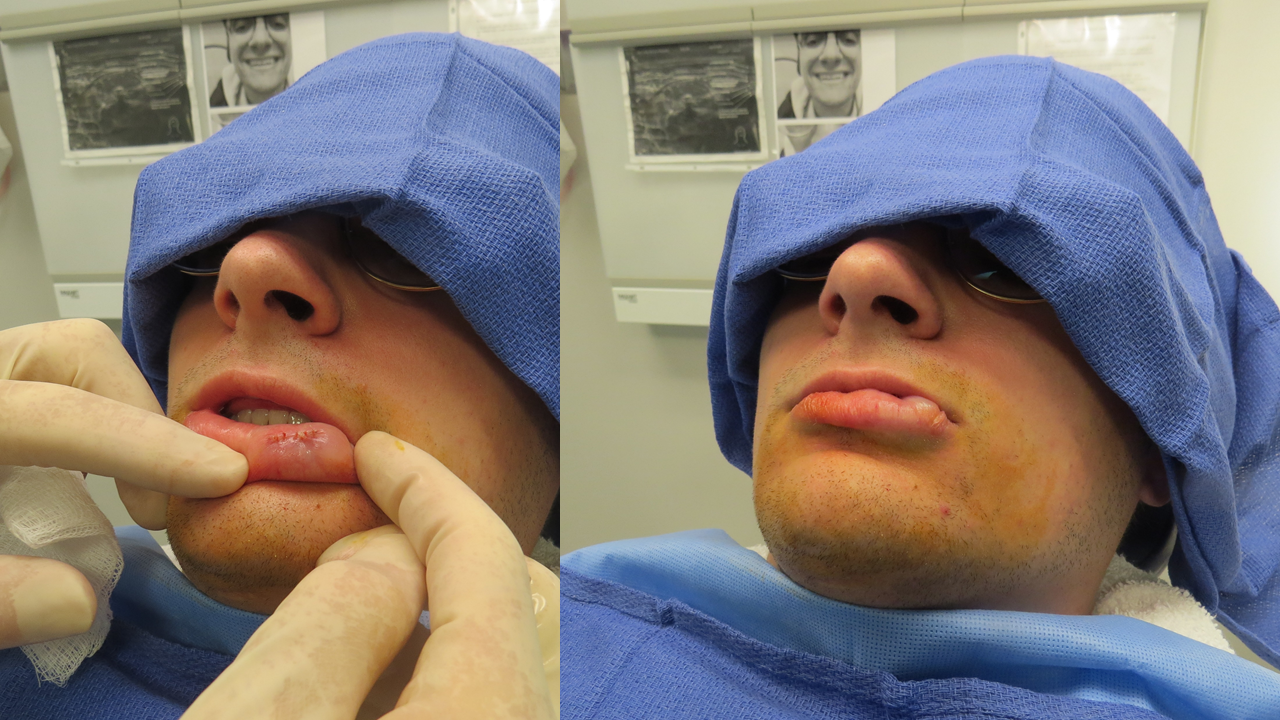
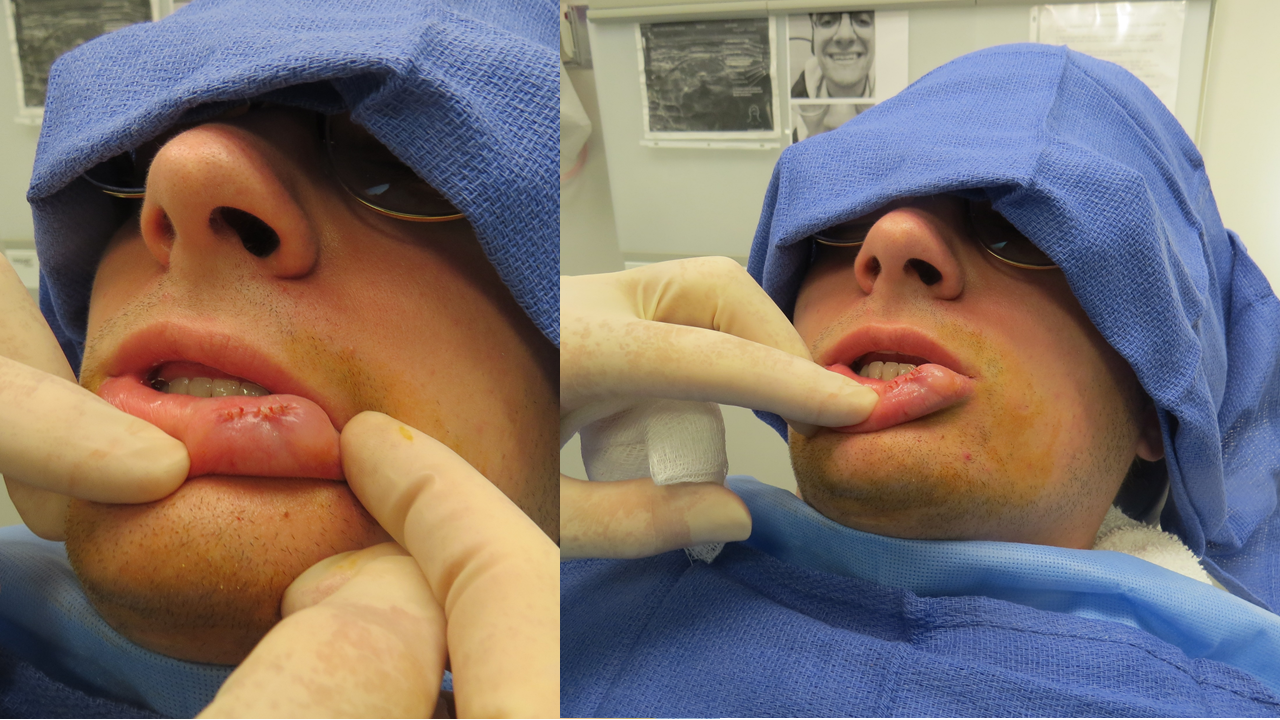
22 year old healthy man who developed painless swelling in the left lower lip without recollection of any instigating features .
The lip lesion enlarged over a few days and has been stable since – bothering him occasionally by striking it when chewing or biting. It has never drained or been drained.

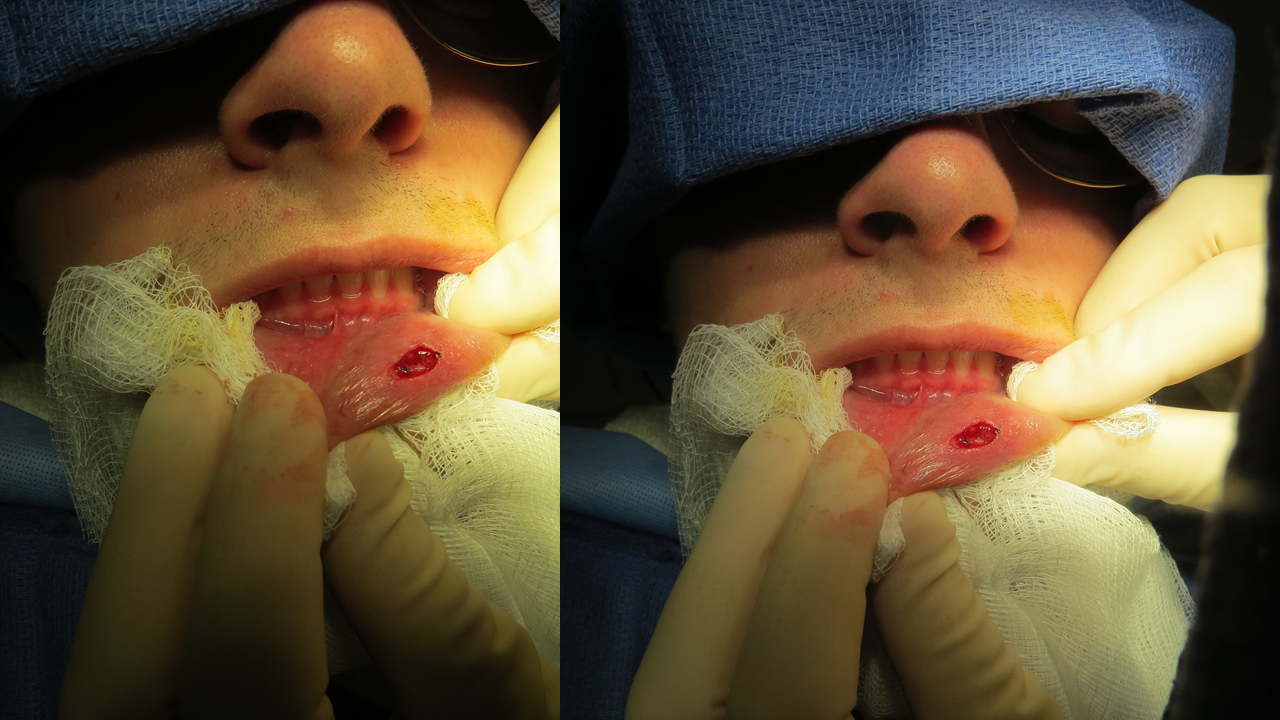
Modified Operative Note:
Procedure: Resection of left lower lip lesion 1-1/2 cm x 1 cm
Preop Diagnosis: Left lower lip lesion possible mucocele versus traumatic fibroma
Postop Diagnosis: Left lower lip mucocele (confirmation by path pending)
Anesthesia: 2% lidocaine with 1-100,000 epinephrine injected to the left lower lip to a volume of 1-1/2 cc
Description of Procedure: Following identification the patient informed consent and a brief timeout as well as the above-mentioned anesthesia the region was prepped and draped in a sterile fashion using Betadine swabs and the lip was put on stretch with retraction having placed images from previous photography from the clinic showing the location of the left lower lip mass prior to injection to corroborate with the findings at the time of injection allowing for a fusiform incision 1-1/2 x 1 cm made parallel to the vermilion to encompass the mass on the wet portion of the left lower lip. Dissection was carried deeper down to muscle as an inflamed minor salivary gland was identified filling the space between mucosa and underlying muscle was identified. An adjacent more normal appearing second salivary gland removed along with the enlarged gland. Closure was effected by way of 6 separate 5-0 Vicryl sutures the first 3 of which incorporated underlying muscle to obliterate dead space.

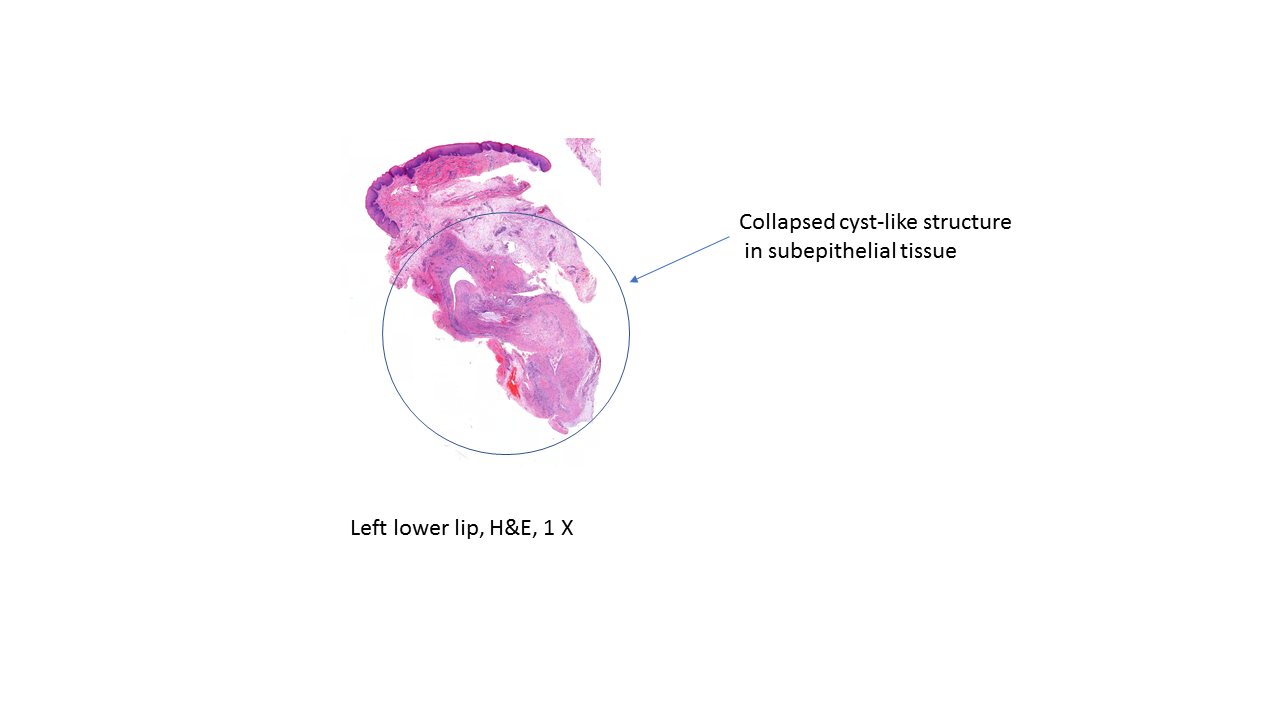
Histopathology:
Left lower lip lesion: Extravasated mucin with associated fibrosis and histiocytic inflammation consistent with mucocele.

References
Miranda GGB, Chaves-Junior SC, Lopes MP, Rocha TBD, Colares DF, Ito FA, Cavalcante IL, Cavalcante RB, Andrade BAB, Nonaka CFW, Alves PM, Albuquerque-Júnior RLC, Cunha JLS. Oral mucoceles: A Brazillian Multicenter Study of 1,901 Cases. Braz Dent J. 2022 Sep-Oct;33(5):81-90. doi: 10.1590/0103-6440202204965. PMID: 36287502; PMCID: PMC9645162.
Chi AC, Lambert PR 3rd, Richardson MS, Neville BW. Oral mucoceles: a clinicopathologic review of 1,824 cases, including unusual variants. J Oral Maxillofac Surg. 2011 Apr;69(4):1086-93. doi: 10.1016/j.joms.2010.02.052. Epub 2010 Aug 12. PMID: 20708324.
Barros CC, Medeiros CK, Rolim LS, Cavalcante IL, Santos PP, Silveira ÉJ, Oliveira PT. A retrospective 11-year study on lip lesions attended at an oral diagnostic service. Med Oral Patol Oral Cir Bucal. 2020 May 1;25(3):e370-e374. doi: 10.4317/medoral.23390. PMID: 32040463; PMCID: PMC7211370.
Bowers EMR, Schaitkin B. Management of Mucoceles, Sialoceles, and Ranulas. Otolaryngol Clin North Am. 2021 Jun;54(3):543-551. doi: 10.1016/j.otc.2021.03.002. PMID: 34024482.
Delbem AC, Cunha RF, Vieira AE, Ribeiro LL. Treatment of mucus retention phenomena in children by the micro-marsupialization technique: case reports. Pediatr Dent. 2000 Mar-Apr;22(2):155-8. PMID: 10769864.
Ohta N, Fukase S, Suzuki Y, Aoyagi M. Treatment of salivary mucocele of the lower lip by OK-432. Auris Nasus Larynx. 2011 Apr;38(2):240-3. doi: 10.1016/j.anl.2010.07.003. Epub 2010 Aug 19. PMID: 20727698.
Huang IY, Chen CM, Kao YH, Worthington P. Treatment of mucocele of the lower lip with carbon dioxide laser. J Oral Maxillofac Surg. 2007 May;65(5):855-8. doi: 10.1016/j.joms.2006.11.013. PMID: 17448832.
Sadiq MSK, Maqsood A, Akhter F, Alam MK, Abbasi MS, Minallah S, Vohra F, Alswairki HJ, Abutayyem H, Mussallam S, Ahmed N. The Effectiveness of Lasers in Treatment of Oral Mucocele in Pediatric Patients: A Systematic Review. Materials (Basel). 2022 Mar 26;15(7):2452. doi: 10.3390/ma15072452. PMID: 35407784; PMCID: PMC8999795.
More, C.B.; Bhavsar, K.; Varma, S.; Tailor, M. Oral mucocele: A clinical and histopathological study. J. Oral Maxillofac. Pathol. 2014, 18 (Suppl. S1), S72
Cecconi, D.R.; Achilli, A.; Tarozzi, M.; Lodi, G.; Demarosi, F.; Sardella, A.; Carrassi, A. Mucoceles of the oral cavity: A large case series (1994–2008) and a literature review. Med. Oral Patol. Oral Y Cir. Bucal 2010, 15, e551–e556
Romeo, U.; Palaia, G.; Tenore, G.; Del Vecchio, A.; Nammour, S. Excision of oral mucocele by different wavelength lasers. Indian J. Dent. Res. 2013, 24, 211.
Graillon N, Mage C, Le Roux MK, Scemama U, Chossegros C, Foletti JM: Mucoceles of the anterior ventral surface of the tongue and the glands of Blandin-Nuhn: 5 cases. J Stomatol Oral Maxillofac Surg. 2019, 120:509-512. 10.1016/j.jormas.2019.04.005
De Falco D, Di Venere D, Maiorano E (March 28, 2020) Diode Laser Excision of Blandin-Nuhn Mucocele. Cureus 12(3): e7441. doi:10.7759/cureus.7441