




click on image above to enlarge; advance with cursor over lateral border
see also: Segmental and Rim Mandibulectomy; Fixation of Vascularized Bone Flap
(Updated protocol pending employing computer planning)
Case History
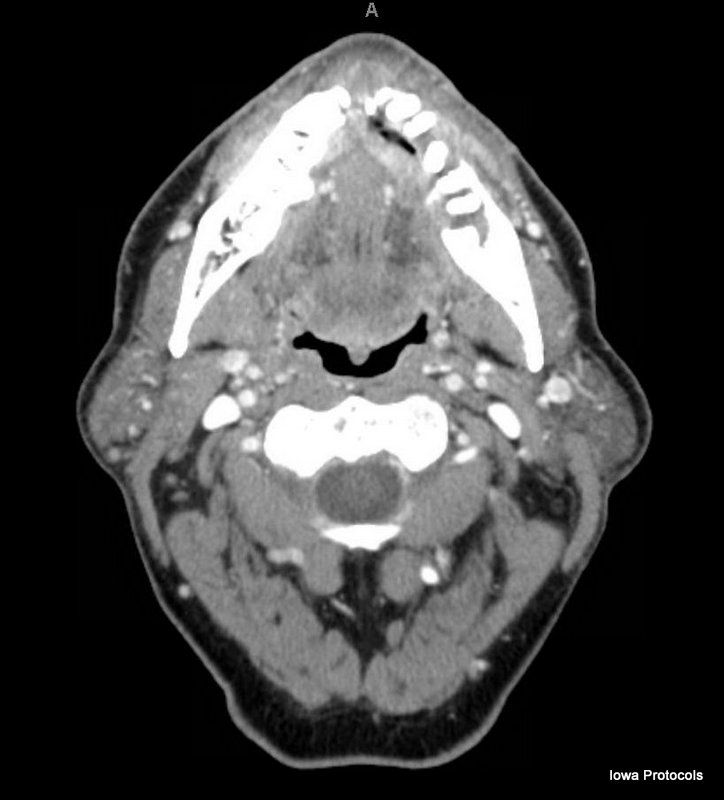
Patient with a T4N0 squamous cell carcinoma of the mandible. Physical exam demonstrates an ulcerative mass extending from the right parasymphysis to the left retromolar trigone with involvement of the floor of mouth but no obvious tongue or lip involvement. CT and Panorex imaging correlates with clinical exam. Patient has strong palpable pulses in the legs bilaterally and vascular studies demonstrate adequate flow in all three lower extremity vessels.
Consent
Risks including but not limited to bleeding, infection, fistula, loss of limb or limb function, flap loss and need for salvage procedures. Discuss impact of this procedure on speech and swallowing as well as external appearance, possible malocclusion and nerve injury. Discuss the general timeline for surgery and recovery as well as timing of future procedures such as osseointegrated dental implants.
Procedure
Tracheotomy, lip split, segmental mandibulectomy, bilateral neck dissection, fibular free flap, split thickness skin graft.
- 11.5 cm x 4cm composite defect including mandible, gingiva, and floor of mouth
- Left fibula free flap harvest with 13cm x 4cm skin paddle with single (oblique) perforator
- 2 osteotomies to create 3.3cm segment for right mandibular segment, and 5.3cm and 2.3cm segments for left mandibular body
- Lateral fixation with 2.3mm KLS locking recon plates; midline fixation with 1.5mm KLS miniplates x2
- Anastomosis of peroneal artery to right facial artery, one vena comitant to the right facial vein with a 4mm venous coupler
- STSG harvest from left thigh
Implants
- KLS Maxillofacial Implant
- Locking mandibular recon angle lt 26H 2.3MM
- Screw locking max drive 2.3MM DIA X 7MM, 11MM, 13MM
- Mini 2.0MM
- Screw cross-drive drill-free mini 2.0MM X 7MM
- Synovis
- Coupler micro 4.0MM
Procedure Note
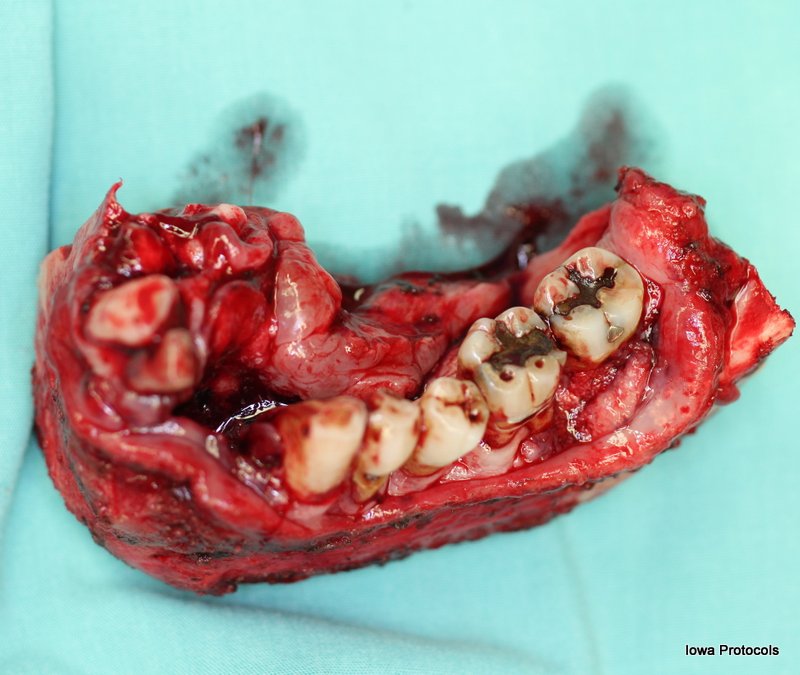
After mandible resection, a 11.5cm x 4cm segmental mandibular defect from the left mandibular angle to the right parasymphysis including the anterior floor of mouth mucosa was present. A fibula free flap was considered adequate for repair of this defect. A left fibula was harvested in order to have the pedicle extend anteriorly into the right neck. The leg was raised and a thigh tourniquet was placed and inflated to 350 mg mercury. The anterior flap incision was made on the lateral aspect of the leg extending from 6 cm inferior to the fibular head to 8 cm superior to the lateral malleolus, with a small backcut made inferiorly. The incision was carried down to and through the fascia overlying the peroneus longus/brevis muscles. Allis clamps were used to retract the fascia posteriorly and dissection continued in a subfascial plane peeling the muscle away from the fascia. One obliquely oriented septo-cutaneous perforator was noted in the distal third of the fibula. The peroneus longus and brevis muscles were elevated off of the medial aspect of the fibula bone with the Kerwen bipolar forceps. Dissection proceeded deeper and the extensor hallucis muscle fascia and inter-osseus membrane were divided with a stab incision into the fascia and continuation along the fibula with the Stevens scissors. The posterior incision was made through the skin and soleus fascia, and the skin paddle raised subfacially until the perforator was seen. Blunt finger dissection was used to identify in the avascular plane along the flexor hallicis muscle, and the fascia of the muscle incised to separate the posterior tibial neurovascular bundle anteriorly. The peroneus vascular pedicle was identified distally and suture ligated with a stick-tie. The common peroneal nerve was identified superiorly and preserved. The periosteum overlying the fibula 6 cm inferior to the fibular head and 8 cm superior to the lateral malleus was raised circumferentially with a right-angle clamp. A Gigli was used to cut the fibula at these points (Note: sagittal saw may also be used). The fibula bone was retracted laterally and the pedicle was traced proximally, dividing the tibialis posterior muscle at the apex of the chevron with a Harmonic scalpel and clipping larger vessels. The flap was eventually pedicled solely on the peroneus vessels including two venae comitantes and a single artery. An arterial and venous branch to the soleus muscle were ligated to increase pedicle length. The tourniquet was released with final ischemic time of 112 minutes and the flap washed with warm saline and allowed to reperfuse for greater than 15 minutes. The superior pedicle was divided and the flap prepared for inset.
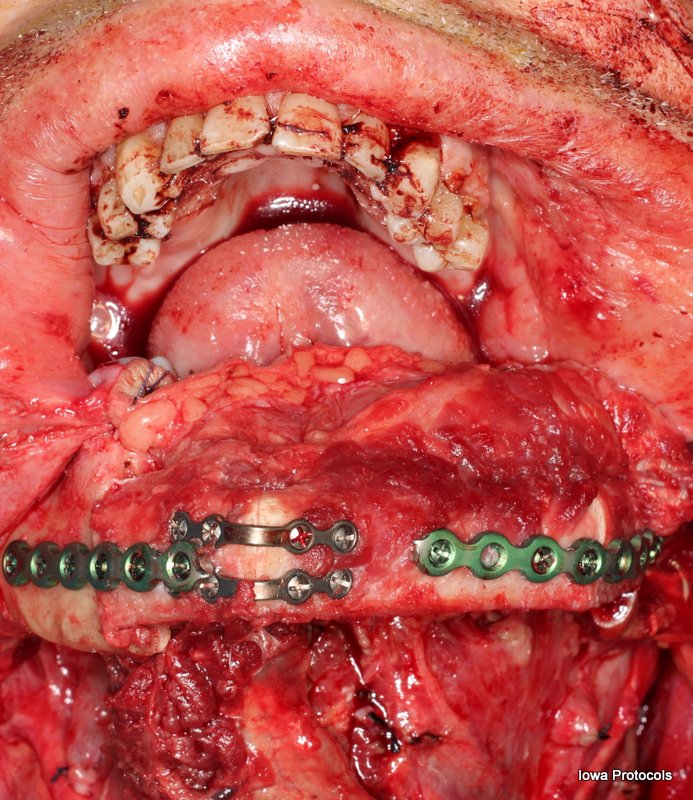
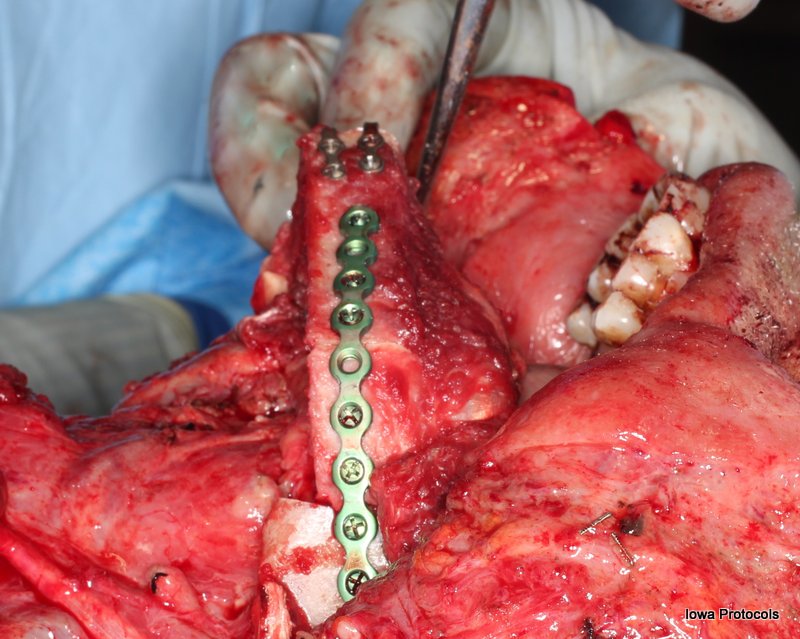
The periosteum of the flap was stripped to match the dimensions of the mandibular defect. A Silastic template was made from the tumor specimen, and two osteotomies planned. The periosteum was raised in these areas and a thin dental malleable used to protect the pedicle while bone cuts were made with the sagittal saw. The excess bone at the ends was removed. The flap was placed into the oral cavity. The skin paddle was inset into the oral cavity defect with interrupted 3-0 Vicryl in horizontal mattress fashion. The anterior osteotomy was secured with two 1.5mm miniplates in a tension and compression band fashion. A right mandibular torus was burred off to enable flap inset and sharp bony edges smoothened. The previously bent reconstruction plate was divided in order to utilize the lateral portions with corresponding 2.3mm locking screws, using monocortical screws on the flap, and bicortical screws on the native mandible. Bone pate used to fill a small gap in the posterior neo-symphysis.
The flap vessels as well as right facial artery and right facial vein were freed from the surrounding tissue and the adventitia trimmed. An arterial anastomosis was performed using the frame and running 9-0 nylon. A venous anastomoses was performed using a 4mm venous coupler system. The flap was reperfused and noted to be bleeding appropriately from the skin edges.
Hemostasis was achieved in the wound bed with bipolar cautery. JP drains were placed and secured with silk suture. The anterior flap skin paddle was inset to the buccal and lip mucosa with horizontal 3-0 Vicryl sutures. The wet lip was closed with Vicryl and dry with with 4-0 chromic. The platysma was closed in interrupted fashion with 3-0 vicryl. The skin was closed in running fashion with 4-0 nylon.
A split thickness skin graft was harvested from the left thigh with a Zimmer dermatome. The skin graft was sutured into the donor skin paddle defect and secured with 4-0 chromic suture. A wound VAC was placed. The leg was wrapped in web-roll and a plaster splint placed followed by an ACE bandage.
The Rusch tube was exchanged for a #6 Shiley tracheostomy and sutured.
References
Sink J, Hamlar D, Kademani D, Khariwala SS. Computer-aided stereolithography for presurgical planning in fibula free tissue reconstruction of the mandible. J Reconstr Microsurg. 2012 Jul;28(6):395-403. doi: 10.1055/s-0032-1315762. Epub 2012 Jun 18. PMID: 22711196.
Sozzi D, Filippi A, Canzi G, De Ponti E, Bozzetti A, Novelli G. Surgical Navigation in Mandibular Reconstruction: Accuracy Evaluation of an Innovative Protocol. J Clin Med. 2022 Apr 6;11(7):2060. doi: 10.3390/jcm11072060. PMID: 35407667; PMCID: PMC8999643.
Kirke DN, Owen RP, Carrao V, Miles BA, Kass JI. Using 3D computer planning for complex reconstruction of mandibular defects. Cancers Head Neck. 2016 Dec 9;1:17. doi: 10.1186/s41199-016-0019-4. PMID: 31093346; PMCID: PMC6460653.