


Click on images above to enlarge and advance with cursor over border
return to: Unilateral Laryngeal Paralysis or Vocal Cord Paralysis
see also: Laryngeal Reinnervation
Ansa cervicalis to recurrent laryngeal nerve
GENERAL CONSIDERATIONS
- Anatomical Considerations:
- Ansa cervicalis
- innervates 3 out of 4 of the strap muscles, including the omohyoid, the sternohyoid, and the sternothyroid muscles. This nerve arises from a small loop between C1 and C2 to join fibers of the hypoglossal nerve for a few centimeters to descend in front of the internal and common carotid arteries as the superior root. This nerve loops to the inferior root of the ansa (formed by C2 and C3) which descends posterior to the carotid sheath, winding laterally to join the superior root either lateral to the internal jugular vein or between it and the common carotid artery. The nerve innervates the inferior portion of these muscles.
- Of note, some nerve fibers from C2, also traveling with the hypoglossal nerve continue to travel with this nerve after the superior root branches off to innervate the thyrohyoid and geniohyoid muscles.
- innervates 3 out of 4 of the strap muscles, including the omohyoid, the sternohyoid, and the sternothyroid muscles. This nerve arises from a small loop between C1 and C2 to join fibers of the hypoglossal nerve for a few centimeters to descend in front of the internal and common carotid arteries as the superior root. This nerve loops to the inferior root of the ansa (formed by C2 and C3) which descends posterior to the carotid sheath, winding laterally to join the superior root either lateral to the internal jugular vein or between it and the common carotid artery. The nerve innervates the inferior portion of these muscles.
- Relevant anatomy of the recurrent laryngeal nerve (RLN)
- The anatomy of the recurrent laryngeal nerve is most constant near the cricothyroid joint. This can be easily identified just adjacent to the tubercle of Zuckerkandl (If the thyroid gland is present), with medial reflection. The joint is palpated, and identified through careful spreads along the path of the nerve. The right RLN's course in a more obtuse approach ranging from 0-45 degrees, while the left takes a more paratracheal path at 0-30 degrees.
- Approaching the nerve distally is also very safe, and effective. The inferior segment of the RLN will be located posterior and deep to the inferior thyroid artery the majority of the time with 30% coursing anteriorly. Due to this unpredictable relation, it may be difficult to identify the nerve in this location. Additionally, if the nerve was transected in a distal location around the area of the thyroid, following the nerve from this location may not be of utility.
- Ansa cervicalis
OPERATIVE PROCEDURE
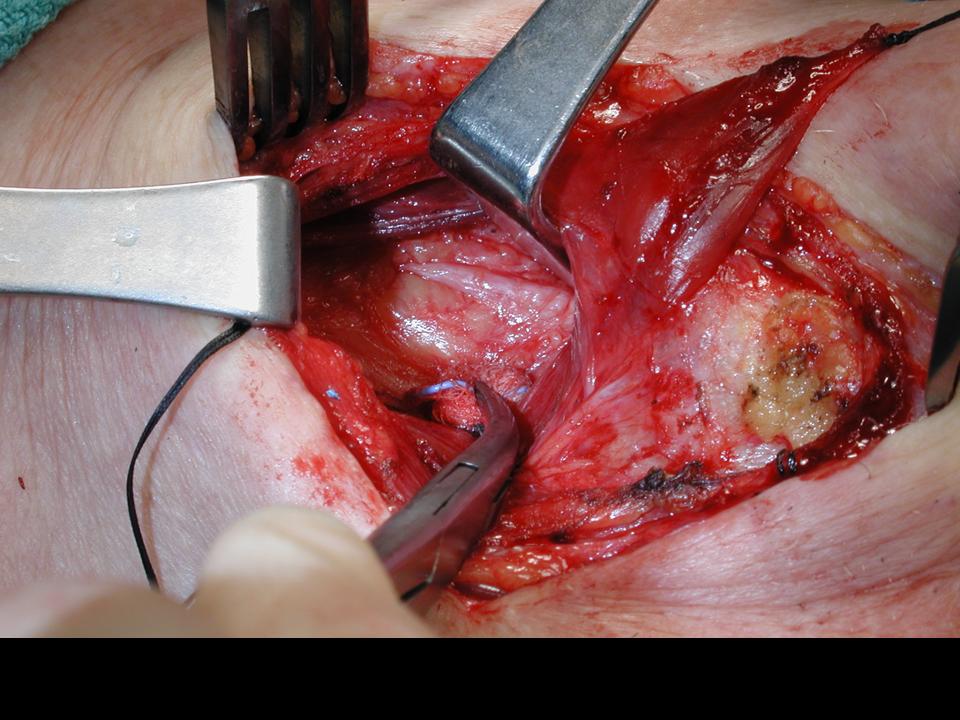
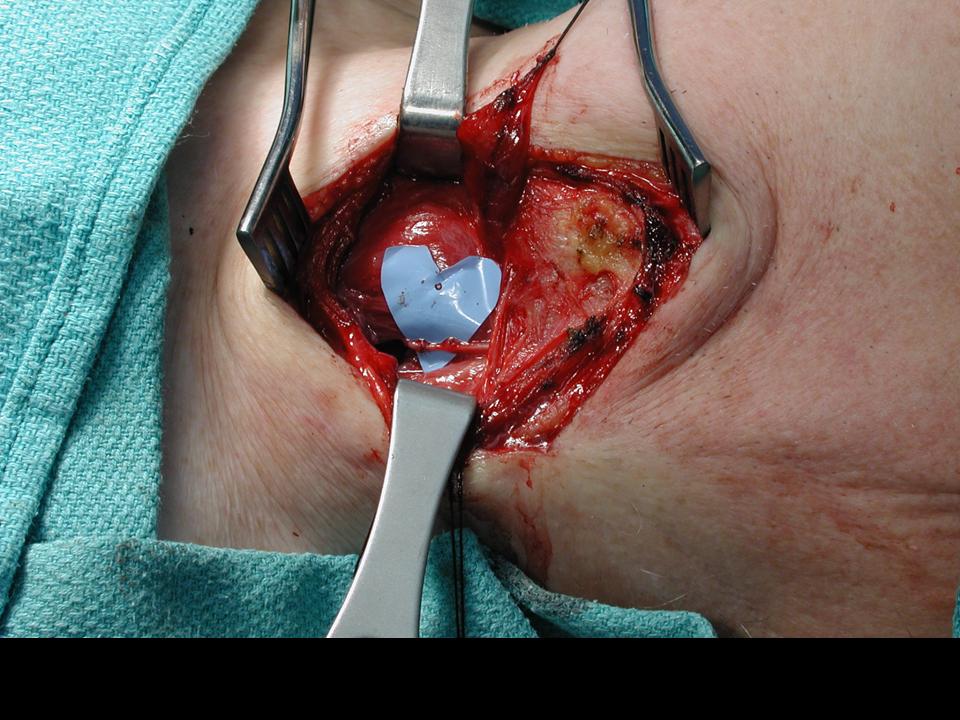
- A transverse collar incision within skin crease approximately 2 cm above the suprasternal notch, at the level of the cricoid. Alternatively, if a previous surgical procedure has been performed, utilizing this incision is preferred. The incision is carried down through the level of the platysmal muscle and the sternocleidomastoid muscle is identified. The sternohyoid muscle is carefully exposed, and the internal jugular vein is visualized.
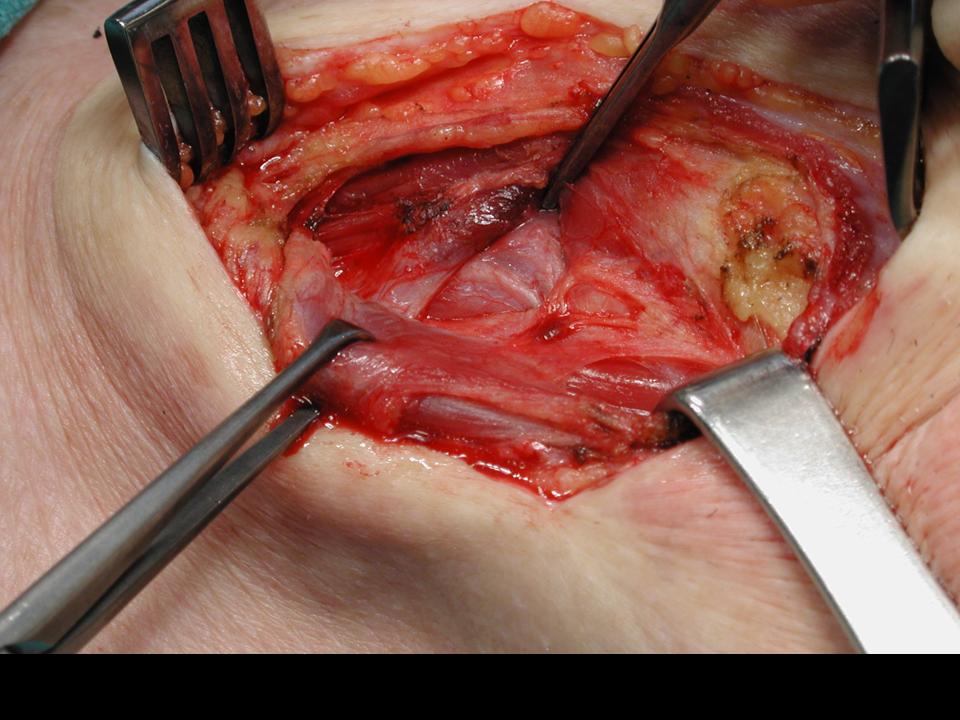
- Dissection continues inferiorly along the SCM until the omohyoid muscle is visualized. A branch of the ansa cervicalis may be visualized entering this muscle on the superior lateral border to provide innervation.
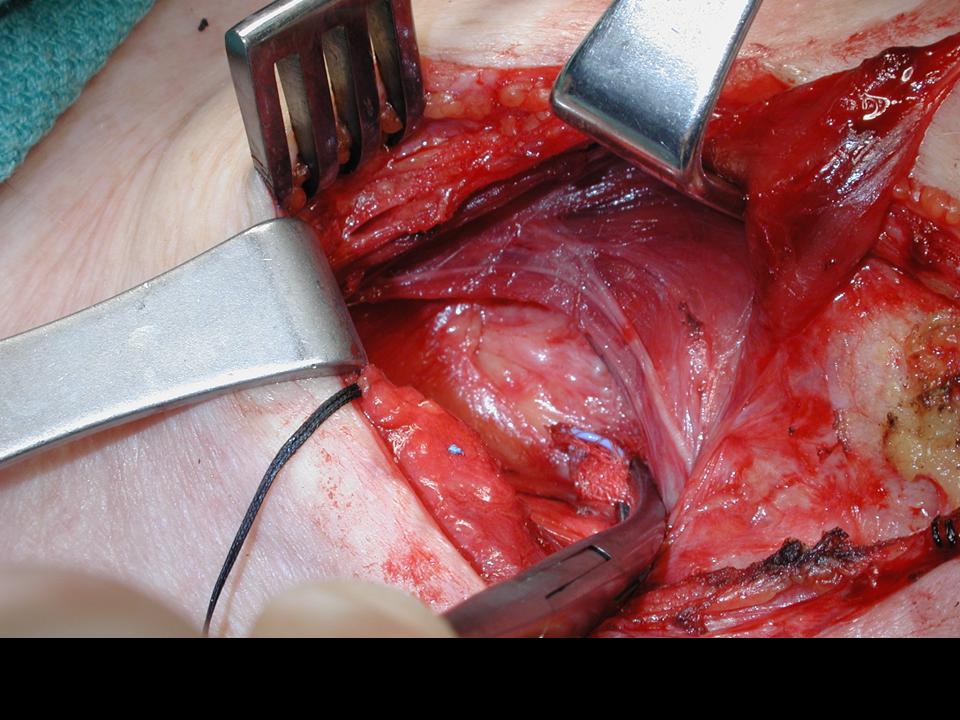
- The ansa cervicalis is identified through the fascia looping over the jugular vein or the carotid. The nerve is traced distally to the main branch which is then transected.
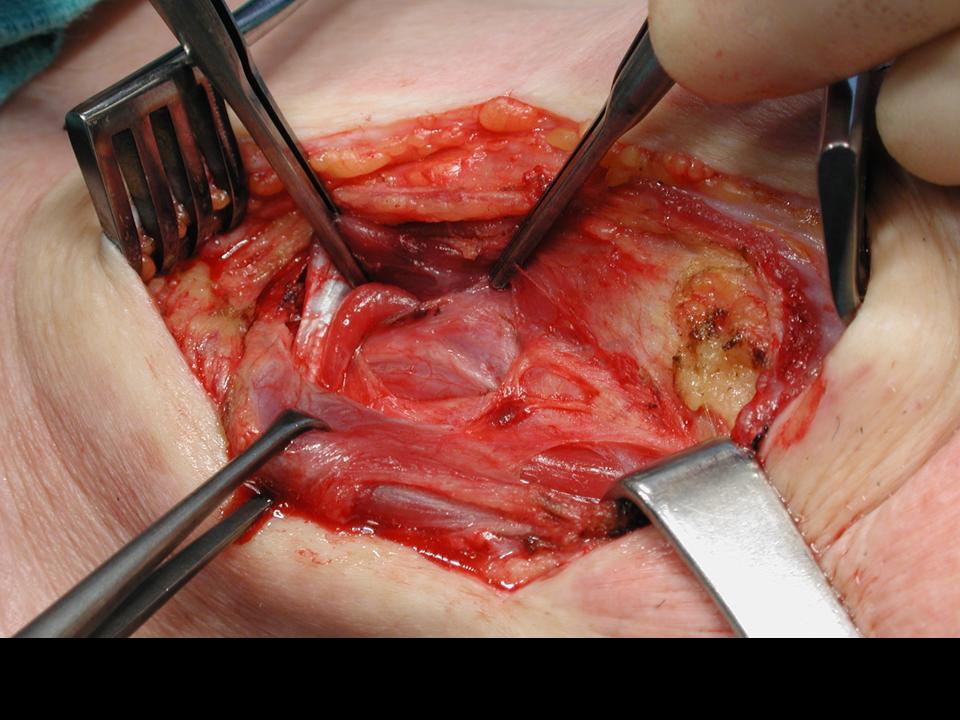
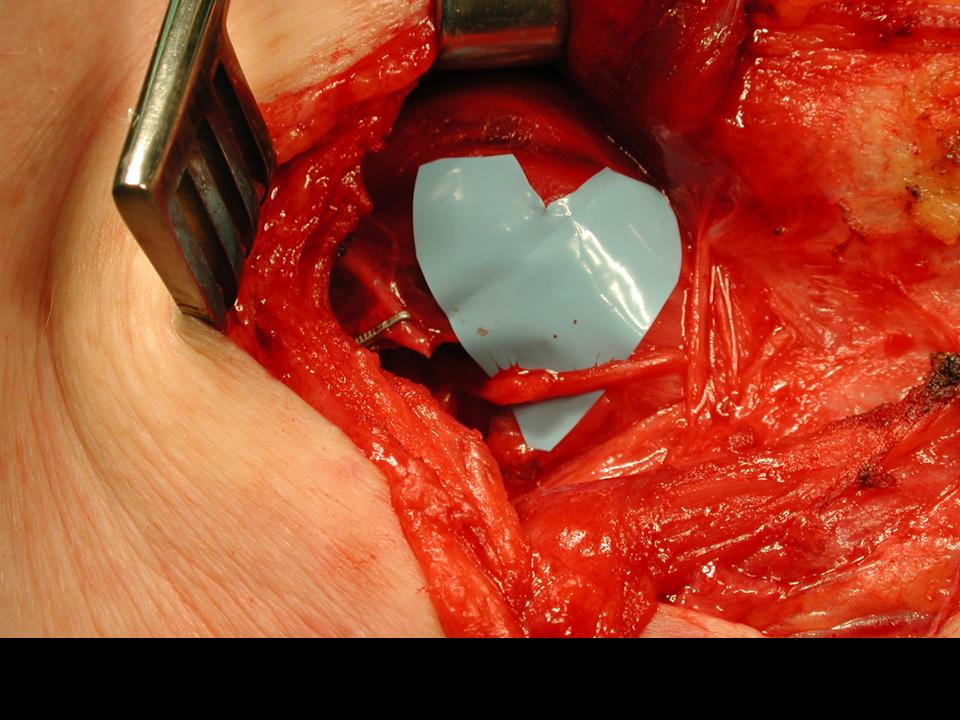
- The nerve endings of the distal RLN stump is prepared with resection of the scarred nerve back to the level of the fascicles. Trimming this nerve promotes early innervation.
- The prepared stump of the RLN is anastomosed to the main branch of the ansa cervicalis using 3-5 epineural interrupted sutures of 9-0 Nylon. Care is taken not do disrupt the fascicles.
- Platysmal closure is performed using 3-0 Vicryl sutures, following by deep closure of the tissue in an interrupted fashion. A 4-0 Monocryl suture is then used to close the superficial layer in a subcutaneous manner. Dermabond is placed over the wound bed.
- If indicated, the patient may be placed into suspension with subsequent injection of the true vocal folds to provide further medialization of the cord.
ADDITIONAL MODIFIED OPERATIVE NOTE (FROM OTHER CASE)
- The ansa cervicalis was identified along the internal jugular vein and traced inferiorly.
- The omohyoid was skeletonized and divided over the internal jugular vein.
- The lateral aspect of the other strap muscles was identified, and the strap muscles were reflected medially.
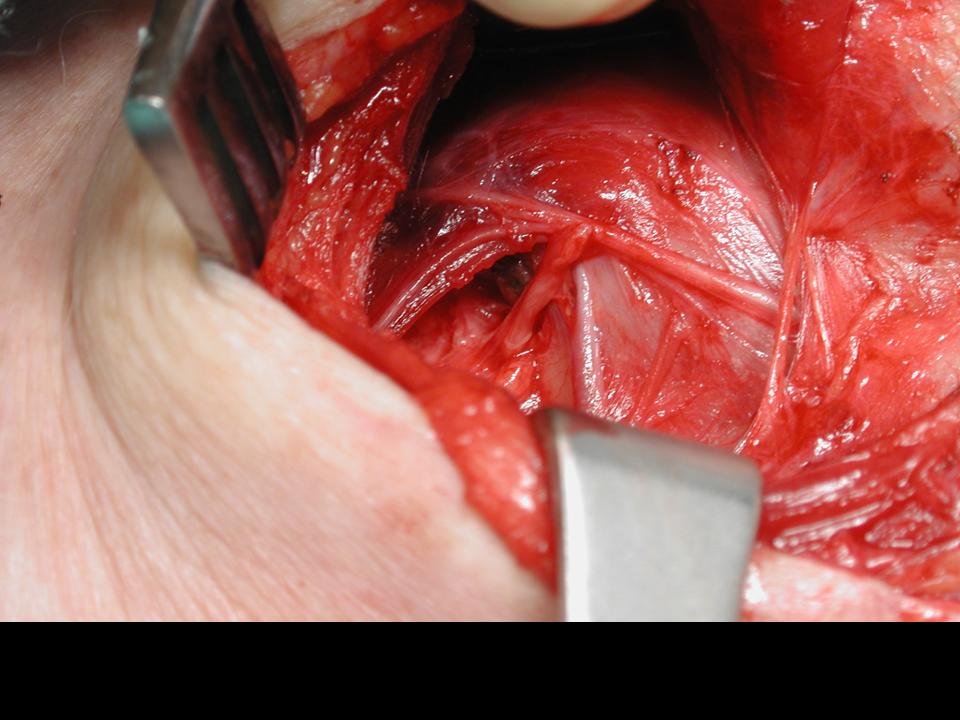
- The posterior edge of the right thyroid gland was identified, grasped with a babcock retractor and drawn medially.
- Blunt dissection was used to identify the recurrent laryngeal nerve.
- The recurrent laryngeal nerve was skeletonized to mobilize it and prevent tension on the anastomosis.
- The recurrent laryngeal nerve and ansa cervicalis were sharply divided.
- The recurrent laryngeal nerve was further prepared by removing a small volume of neural tissue within the epineurium (to permit accurate epineurial reapproximation)
- 8-0 nylon suture was used to perform a neurorrhaphy with epineurial sutures.
- The omohyoid muscle was reapproximated with Vicryl suture.
POSTOPERATIVE CONSIDERATIONS
- Videostroboscopy can be performed post-operatively with final improvement noted at 2 years. Glottic closure, vocal fold edge, vocal fold position, phase symmetry and regularity are expected to improve.
- As er Van Lith-Bijl and Desuter (van Lith-Bijl 2020) offered a contemporary review of laryngeal rerinnervation and identified:
- Re-anastomosis of a severed recurrent laryngeal nerve (RLN) identifiied that: "RLN repairs are incapable of producing cyclic abductionor adduction. If the synkinesis is a balanced activity of adductor and abductor fibers, the voice results may be adequate, but adverse effects of paradoxical activity mus be considered"
- Reinnervation of the extralaryngeal RLN main trunk with 'foreign nerves' has been successful employing the ansa cervicalis to RLN nerve transfer with good voice results (citing Lee 2007, Lorenz 2008, Wang 2011)
- No active mobility was achieved
- Patients developed muscle tonus in adductor musculatrure and 'satisfactory improvement in the voice'
- Paradoxical motion is prevented with a weak activity parttern or a basic tone.
REFERENCES
Maisie L. Shindo, MD, James C. Wu, MD, and Eunice E. Park, MPH. Surgical Anatomy of the Recurrent Laryngeal Nerve Revisited. Otolaryngology--Head and Neck Surgery (2005) 133, 514-519* Nerve Revisited
Lorenz RR, Esclamado RM, Teker AM, Strome M, Scharpf J, et al. (2008) Ansa cervicalis-to-recurrent laryngeal nerve anastomosis for unilateral vocal fold paralysis: experience of a single institution. Ann Otol Rhinol Laryngol 117:40--45.cervicalis-to-recurrent laryngeal nerve anastomosis for unilateral vocal fold
Wang W, Chen D, Chen S, Li D, Li M, Xia S, Zheng H. Laryngeal reinnervation using ansa cervicalis for thyroid surgery-related unilateral vocal fold paralysis: a long-term outcome analysis of 237 cases. PLoS One. 2011 Apr 29;6(4):e19128.paralysis: experience of a single institution. Ann Otol Rhinol Laryngol 117:40--45.
van Lith-Bijl JT, Desuter GRR. Laryngeal Reinnervation: The History and Where We Stand Now. Adv Otorhinolaryngol. 2020;85:98-111. doi: 10.1159/000456688. Epub 2020 Nov 9. PMID: 33166981.
Lee WT, Milstein C, Hicks D, Akst LM, Esclamado RM: Results of ansa to recurrent laryngeal nerve reinnervation. Otolaryngol Head Neck Surg 2007;136:450– 454.
Lorenz RR, Esclamado RM, Teker AM, Strome M, Scharpf J, Hicks D, Lee WT: Ansa cervicalis-to-recurrent laryngeal nerve anastomosis for unilateral vocal fold paralysis: experience of a single institution. Ann Otol Rhinol Laryngol 2008;117:40–45.
Wang W, Chen D, Chen S, Li D, Li M, Xia S, Zheng H: Laryngeal reinnervation using ansa cervicalis for thyroid surgery-related unilateral vocal fold paralysis: a long-term outcome analysis of 237 cases. PLoS One 2011;6:e19128.