return to: Otology - Neurotology; Vertigo
Characteristics
- Clinical syndrome associated with a specific set of symptoms
- Pathologically described as endolymphatic hydrops
- Chronically progressive, destructive disorder involving both the cochlea and labyrinth
- Permanent hearing loss and vestibular injury
- Can affect both ears
- Relapsing, remitting course
Etiology
- Idiopathic
- Genetics and environmental exposure play a role in its development
Pathophysiology
- Accumulation of endolymph in the cochlear duct and vestibular organs (endolymphatic hydrops)
Symptoms
- Episodes lasting 30 minutes to several hours of:
- Spontaneous vertigo
- Unilateral fluctuating sensorineural hearing loss (SNHL)
- Tinnitus
- Aural fullness
- Natural History
- Vertigo symptoms more common at beginning of disease
- Hearing loss and vestibular hypofunction vary greatly between patients
- Hearing loss fluctuates spontaneously in the first few years
- After repeated attacks hearing loss may progress and become permanent
- Triggers tend to develop later in the disease as the result of advanced hydrops bringing the membranous labyrinth in close proximity to the stapes foot plate
- International Classification of Vestibular Disorders (ICVD) Criteria
- Definite Meniere's Disease
- > 2 episodes of spontaneous vertigo lasting 20 minutes to 12 hours
- Audiometrically documented low- to medium frequency sensorineural hearing loss in one ear, defining the affected ear on at least one occasion before, during or after one of the episodes of vertigo
- Fluctuating aural symptoms (hearing, tinnitus or fullness) in the affected ear
- Not better accounted for by another vestibular diagnosis
- Probable Meniere's Disease
- > 2 episodes of vertigo or dizziness, each lasting 20 minutes to 24 hours
- Fluctuating aural symptoms (hearing, tinnitus or fullness) in the affected ear
- Not better accounted for by another vestibular diagnosis
- Definite Meniere's Disease
- Triggers - often occur later in disease
- Tullio's Phenomenon
- Episodes of vertigo lasting seconds to minutes triggered by high intensity and low frequency sounds
- Dietary
- Excessive consumption of salt or caffeine
- Changes in Pressure
- Tullio's Phenomenon
Differential Diagnosis
- Transient Ischemic Attack (TIA)
- Vestibular migraine
- Vestibular paroxysmia
- Recurrent unilateral vestibulopathy
- Vestibular schwanomma
- Endolymphatic sac tumor
- Autoimmune disease
- Human Immunodeficiency Virus (HIV)
- Syphilis
Diagnosis
- History
- < 50 y.o. ask about migraine headaches
- Snoring (association with sleep apnea)
- Vascular factors
- Smoking
- Diabetes mellitus
- Vasculitis
- Myocardial infarction (MI)
- Stroke
- Family History
- Familial Meniere's Disease - at least one other relative (first or second degree) fulfills all the criteria of definite or probable MD
- 8%–9% of sporadic cases in populations of European descent
- Genetic heterogeneity, and mitochondrial and recessive inheritance patterns
- Mutations in DTNA and FAM136A genes
- Familial Meniere's Disease - at least one other relative (first or second degree) fulfills all the criteria of definite or probable MD
- MRI - rule out structural cause
- Electrocochleography (ECoG)
- Auditory brain stem response (ABR)
- Electronystagmogram (ENG)
- Audiometry
Management
- Surgical
- Ablative Procedures - greater vertigo control rates compared to non-ablative procedures but require vestibular compensation to limit post-treatment disequilibrium
- Gentamicin middle ear injections
- Labyrinthectomy - most reliable
- Permanent Hearing Loss
- Removal of all of the vestibular neuroepithelium
- Vestibular Nerve Section
- Vestibular division of CN VIII is selectively divided to remove vestibular function from affected side
- Approaches:
- Middle fossa
- Retrolabyrinthine
- Retrosigmoid
- Translabyrinthine
- Complications
- Facial paralysis
- Hearing loss
- CSF leak
- Persistent disequilibrium
- Non-ablative Procedures
- Endolymphatic shunt (see Sham Surgery Trial by Thomsen et al, 1981)
- shunting - placement of synthetic shunt to drain endolymph
- drainage - incision of the sac to allow endolypmh drainage
- decompression - improve sac function of endolymph absorption
- Intratympanic steroid perfusion
- Endolymphatic shunt (see Sham Surgery Trial by Thomsen et al, 1981)
- American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS) on Reporting of Vertigo Control in Meniere's Disease
- 18-24 months following treatment: divide number of episodes per 6 months by the number of episodes in the 6 months prior to treatment
- Grade A: complete control (0%)
- Grade B: Substantial control (1% - 40%)
- Grade C: Partial control (41% - 80%)
- Grade D: No control (80% - 120%)
- Grade E: Worse (>120%)
- Grade F: Secondary treatment required due to disabling vertigo
- 18-24 months following treatment: divide number of episodes per 6 months by the number of episodes in the 6 months prior to treatment
- Ablative Procedures - greater vertigo control rates compared to non-ablative procedures but require vestibular compensation to limit post-treatment disequilibrium
- Pharmacologic
- Vestibulosuppressants
- Meclizine [Antivert]
- Droperidol [Inapsine]
- Prochlorperazine [Compazine]
- Benzodiazepines
- Diazepam [Valium]
- Lorazepam [Ativan]
- Alprazolam [Xanax]
- Diuretics
- Hydrochlorothiazide and triamterene [Dyazide]
- Hydrochlorothiazide [Aquazide]
- Acetazolamide [Diamox]
- Methazolamide [Neptazane])
- Steroids
- Routes of Administration: orally, intramuscularly, intratympanically
- Aminoglycosides
- Vestibulosuppressants
- Lifestyle
- Low salt diet (< 2g/day)
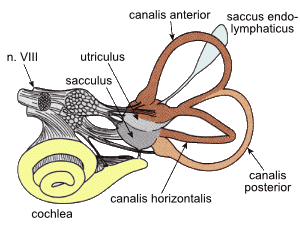
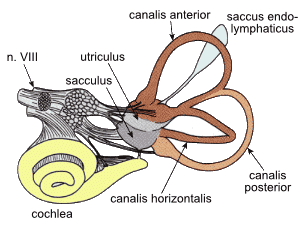
image from wikicommons with permission By VestibularSystem.png: *VestibularSystem.gif: user:Thomas.haslwanterderivative work: Ortisa (talk)derivative work: Icewalker cs (talk) - VestibularSystem.png, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=16880697
References
American Academy of Otolaryngology - Head and Neck Surgery. (2017). Meniere's Disease. http://www.entnet.org/content/menieres-disease
Lopez-Escamez J. A., Carey J., Chung W.-H., Goebel J. A., Magnusson M., Mandalà M., et al. . (2015). Diagnostic criteria for Menière's disease. J. Vest. Res. 25, 1–7. 10.3233/VES-150549
Scholes M. A., Ramakrishnan V. R. (2016). ENT Secrets Fourth Edition. Elsevier. 246, 293-294.
Thomsen J, Bretlau P, Tos M, Johnsen N J. Placebo effect in surgery for Ménière's disease. A double-blind, placebo-controlled study on endolymphatic sac shunt surgery. Arch Otolaryngol. 1981;107(05):271–277.