








return to: Parotidectomy with Facial Nerve Dissection
see also: Case example - neck apocrine cystadenoma presenting clinically similar to lipoma
Lipoma Radiology; Liposarcoma Radiology
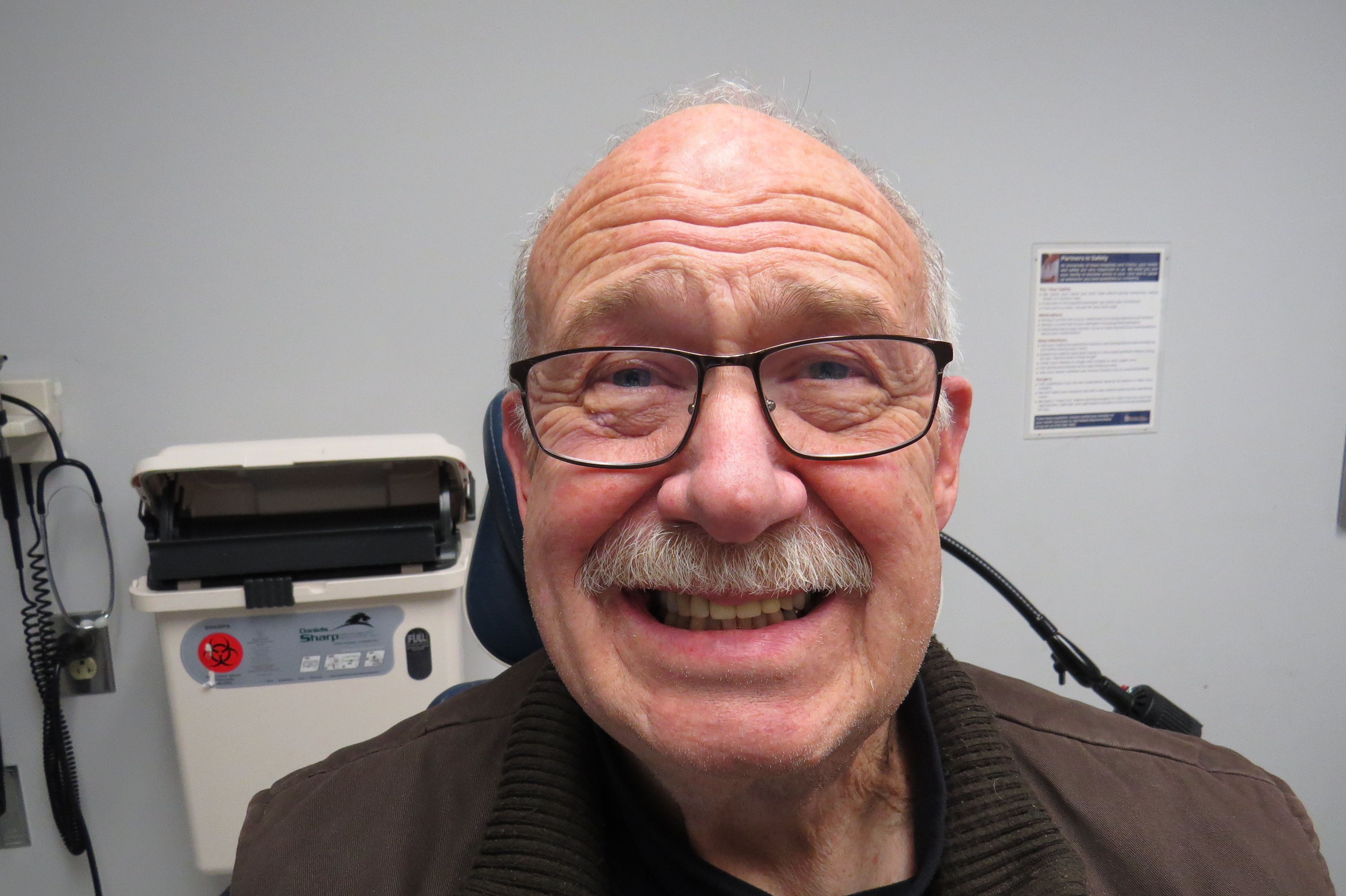
Followup 10 years later:



Presentation Nov 2008 with 'salivary swelling (left parotid):
it 'comes and goes' - 'has been somewhat responsive to antibiotics and
conservative measures such as massage, but it never completely goes away'
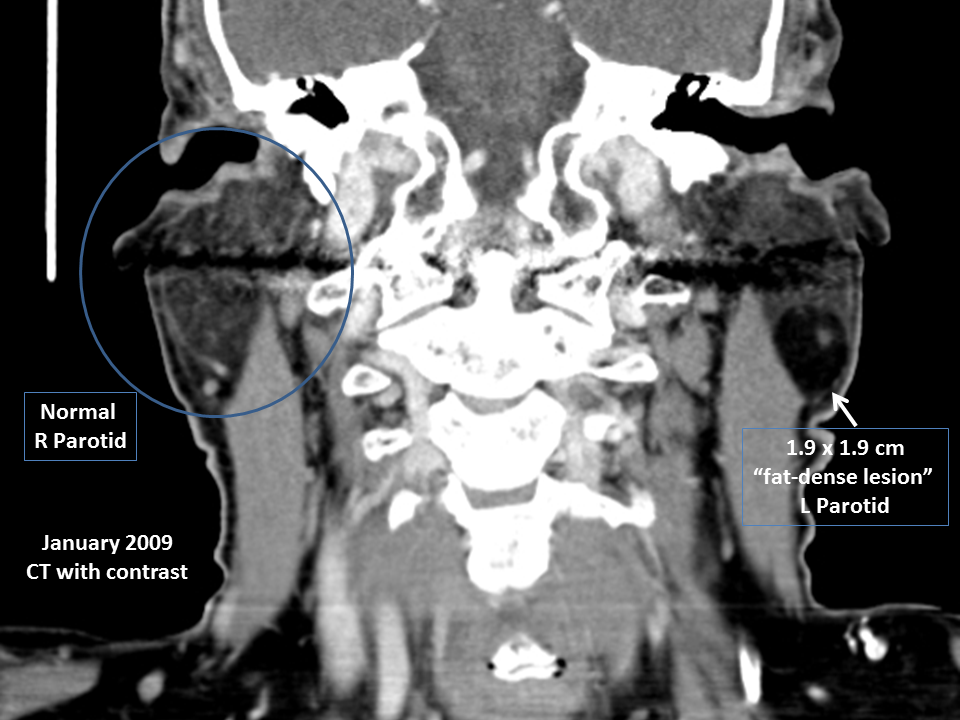
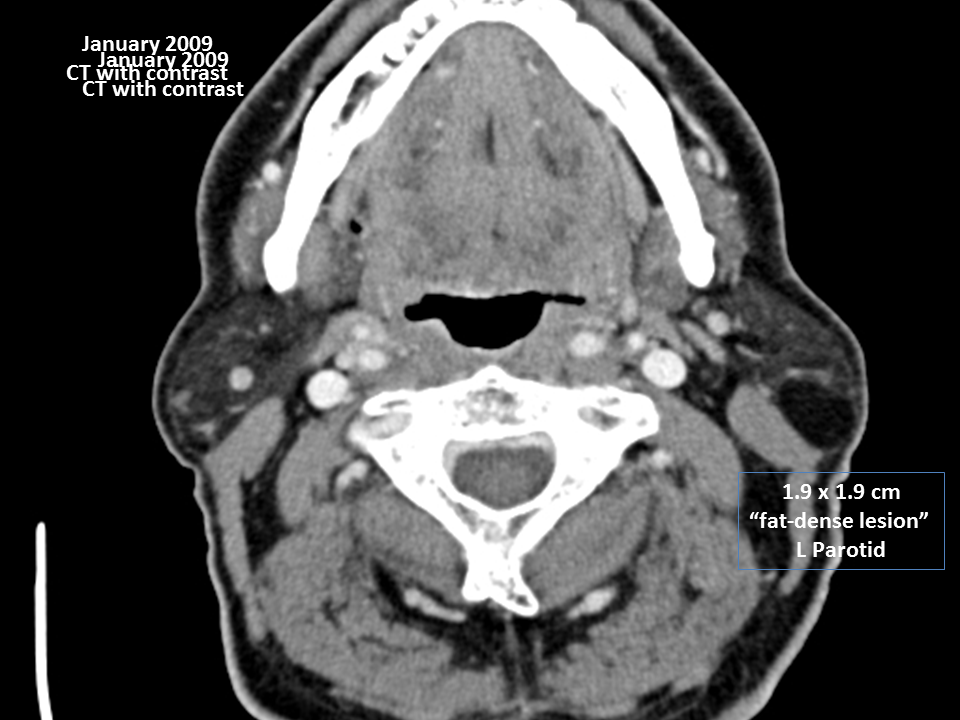
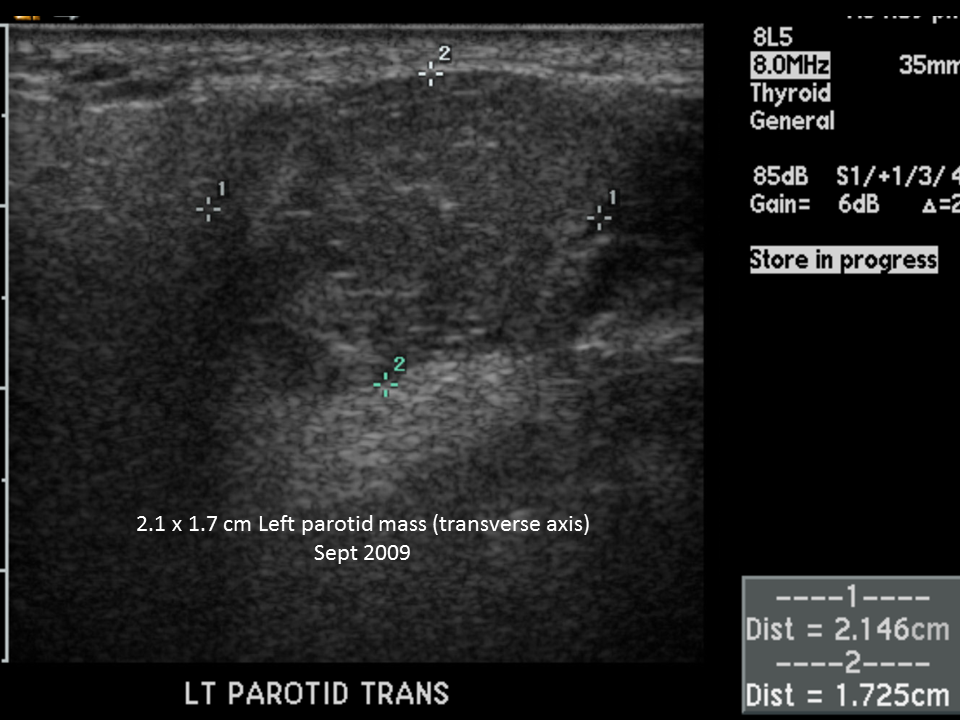
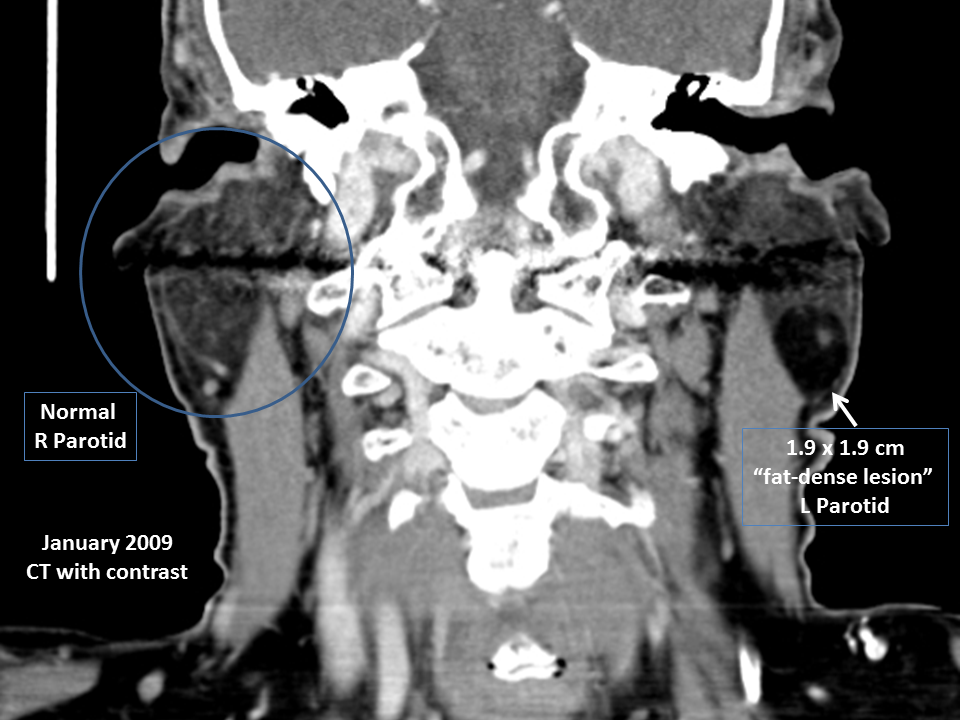
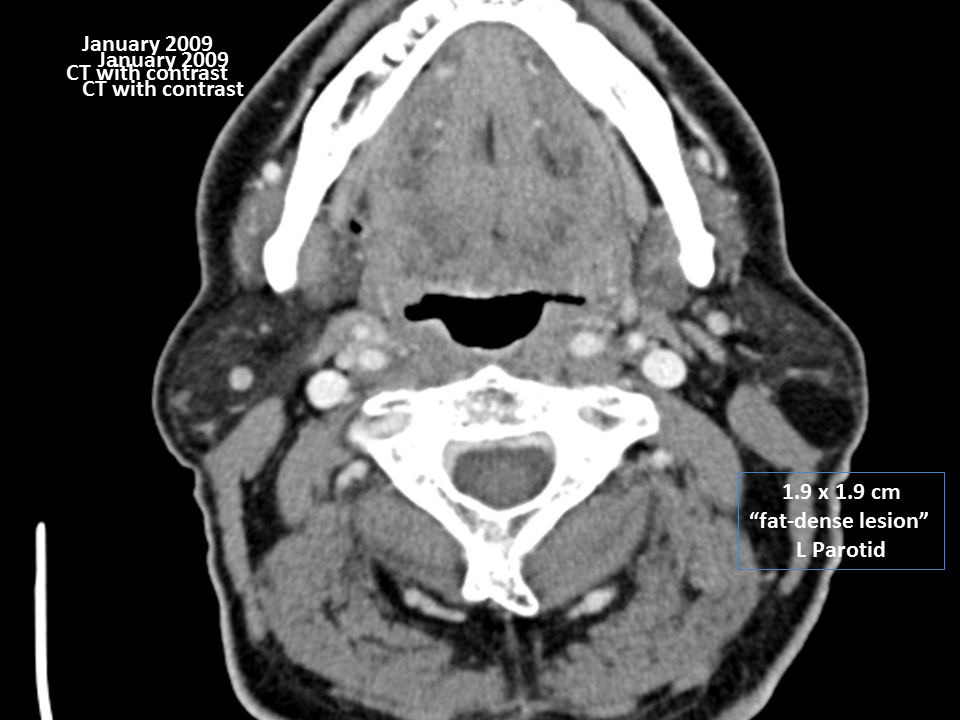
January 2009 CT: Well circumscribed fatty dense lesion in the left parotid gland.
This could represent lipomatous tumor such as lipoma.
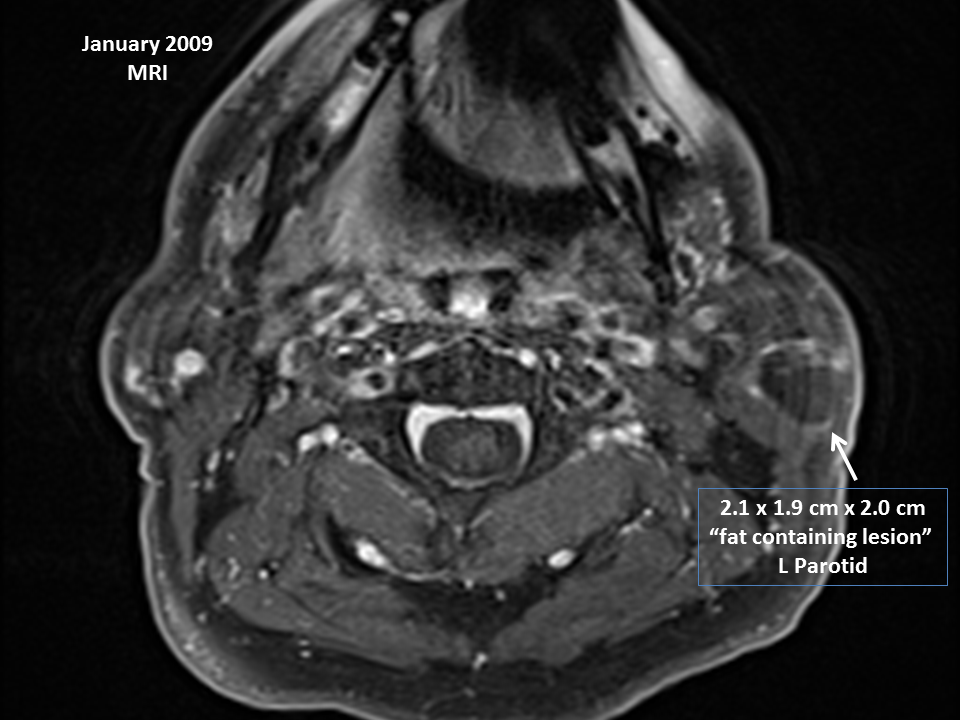
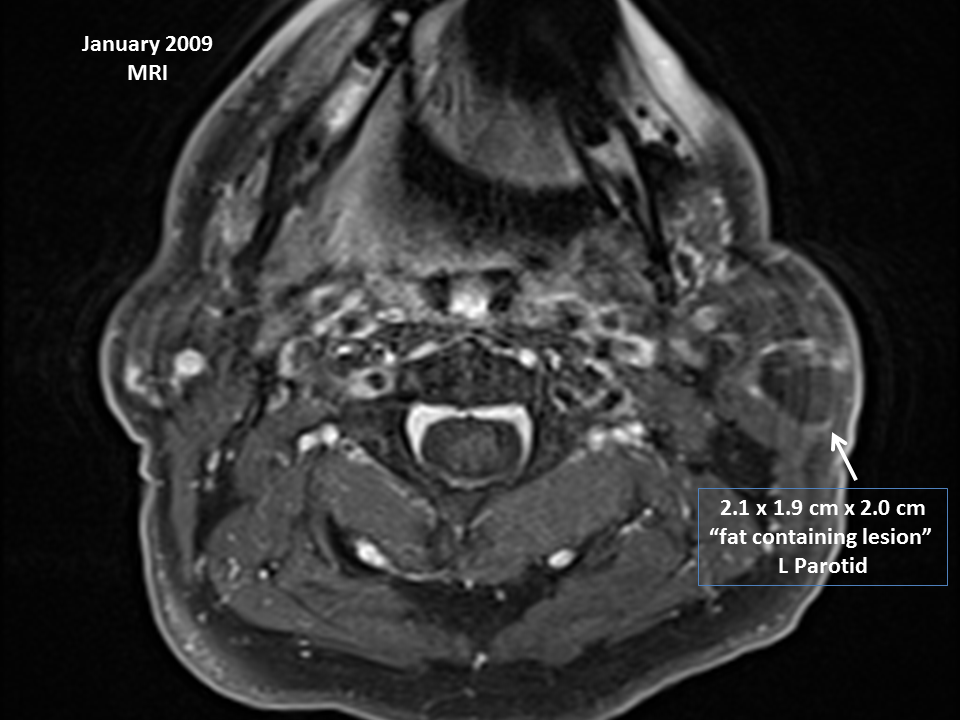
Preop MRI: Left parotid lipomatous tumor, containing small enhancing lesion
with differential of vascular structure versus solid lesion. Repeat
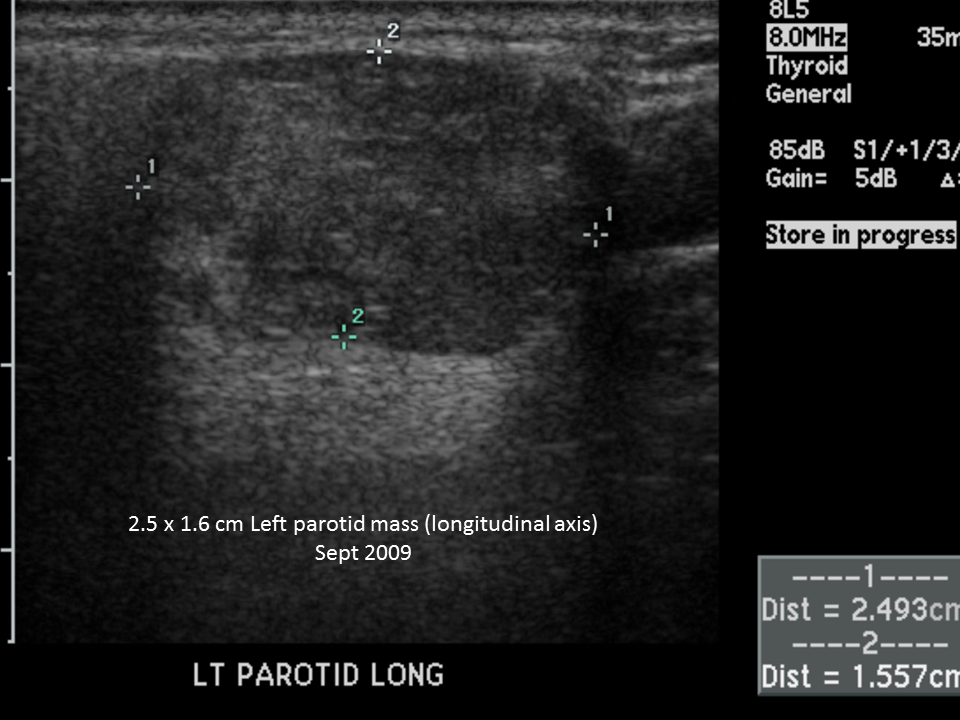
ultrasound to further define the possible vasculature is recommended.
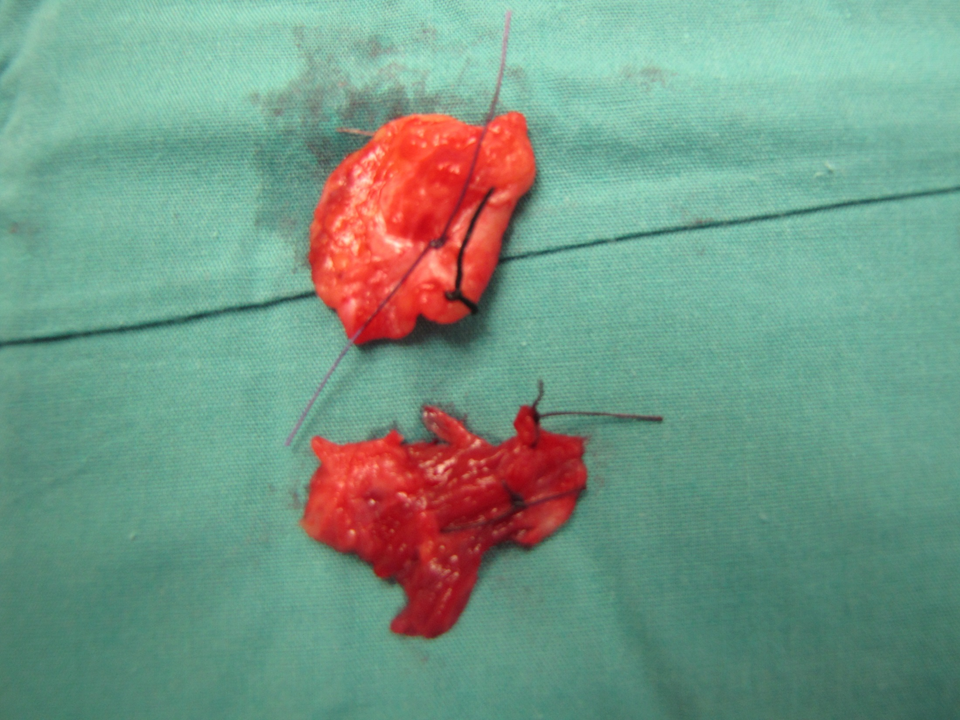
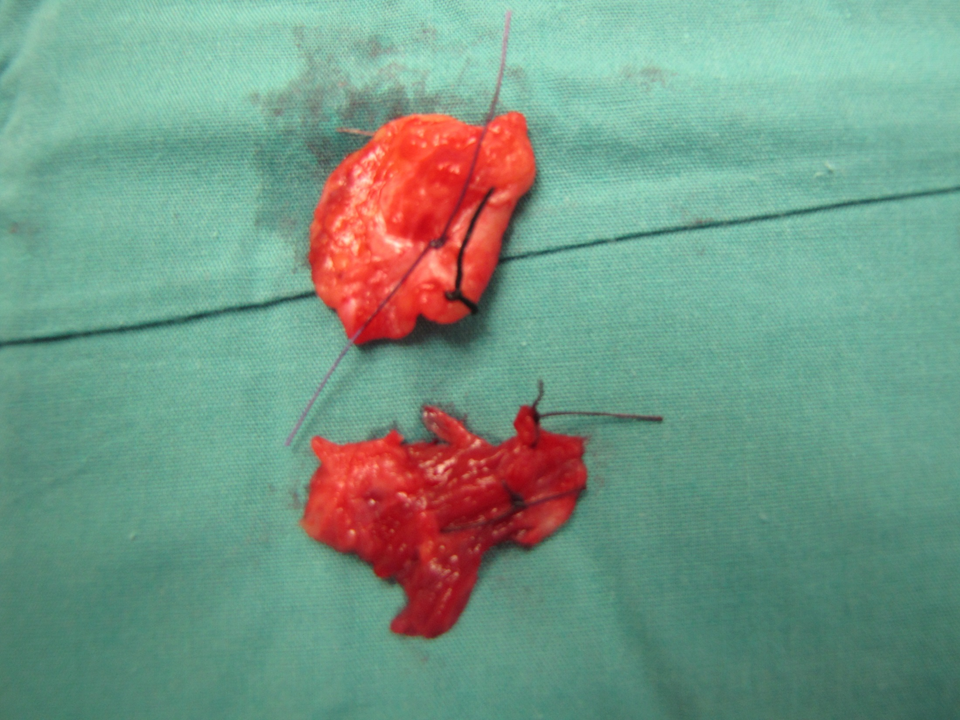
Diagnosis: (path report after first resection)
- Atypical lipomatous neoplasm, favor well differentiated, lipoma-like
liposarcoma, 2.3 cm in greatest dimension, abutting the lateral surgical resection margin.
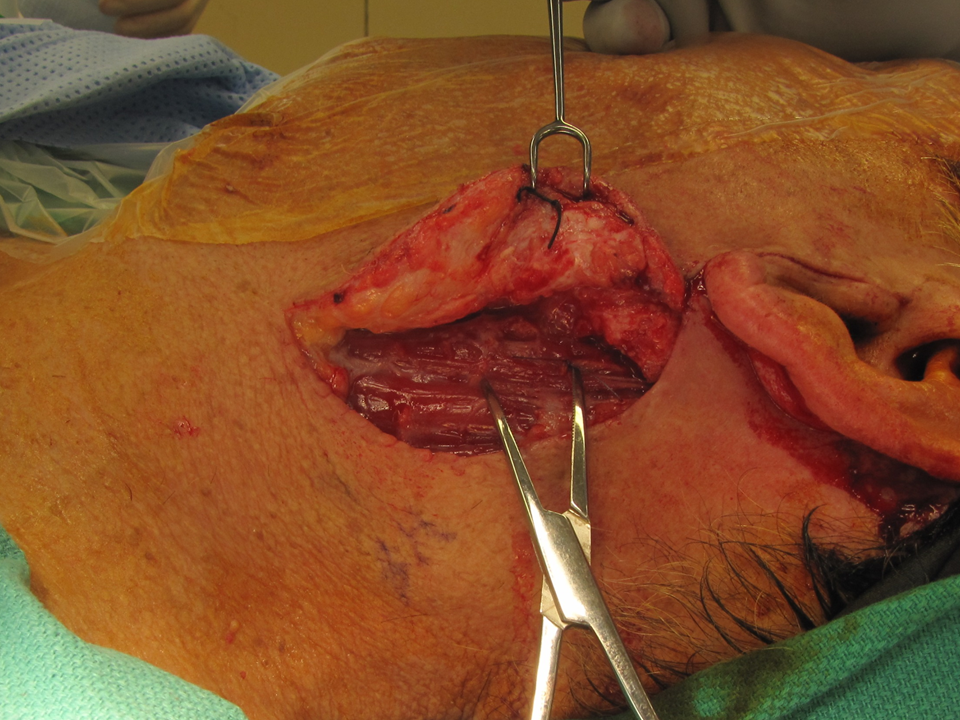
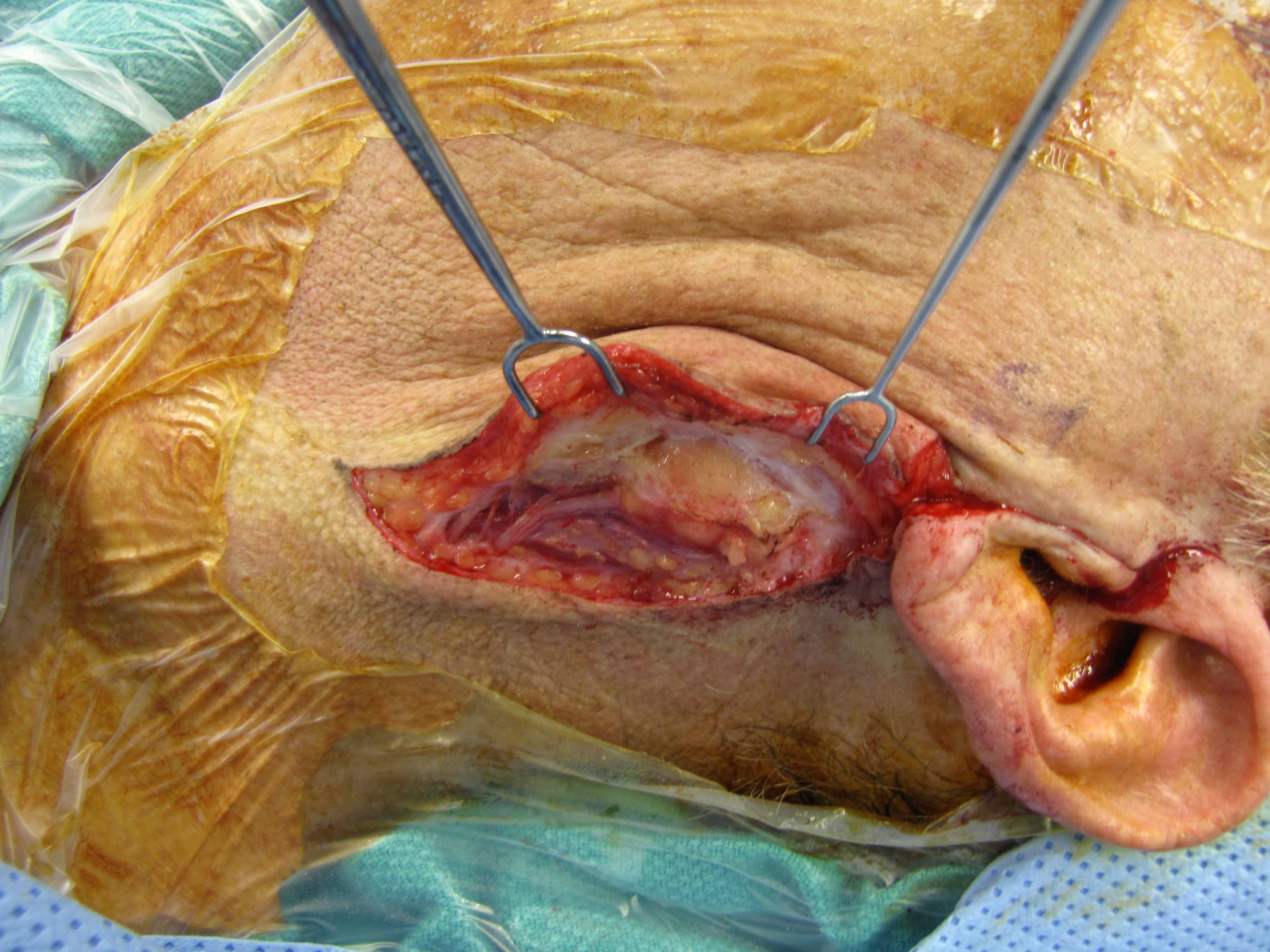
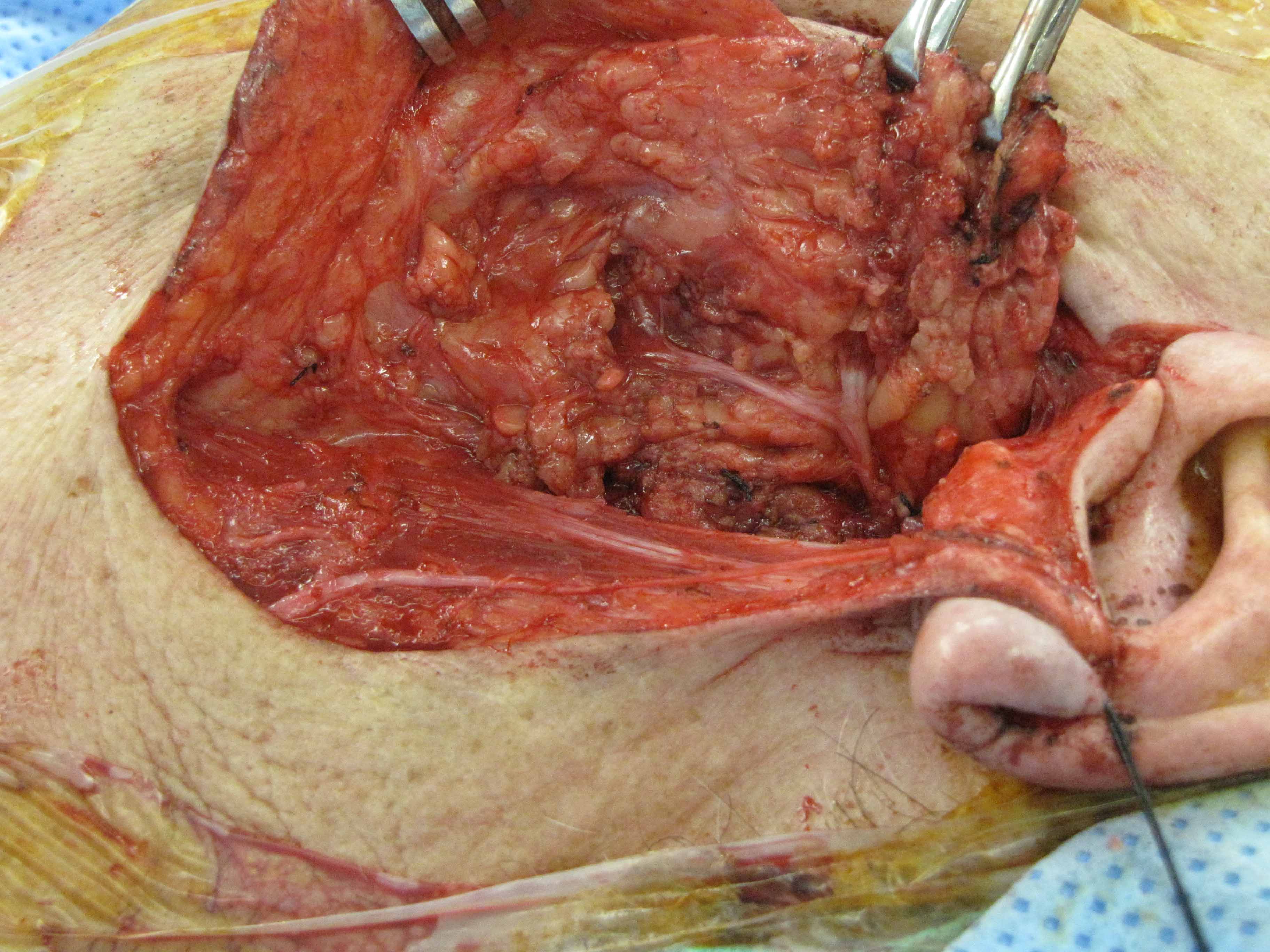
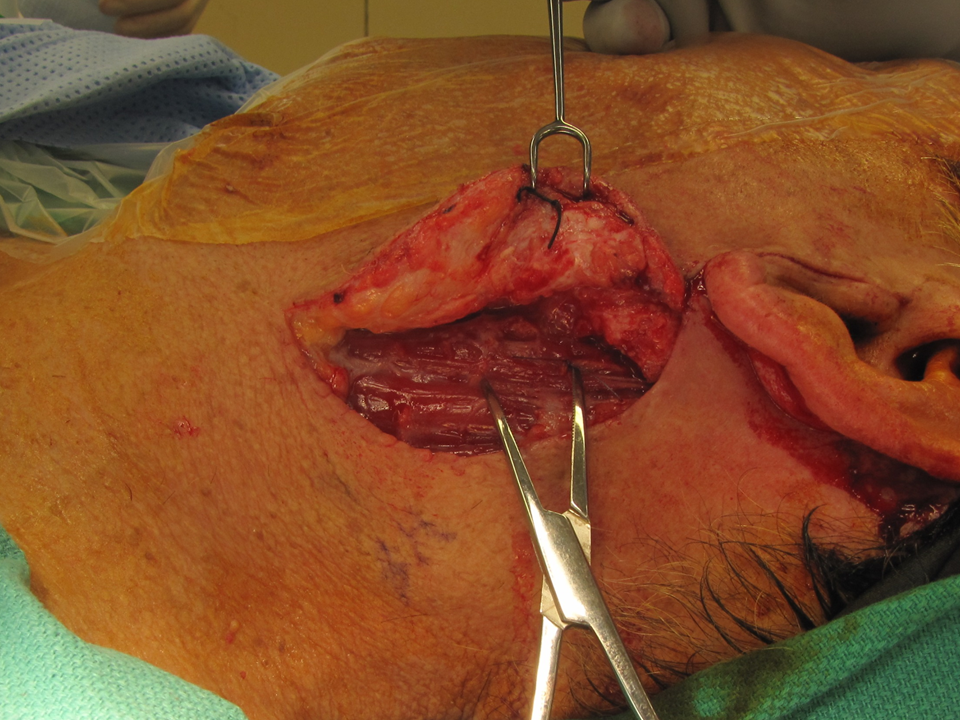
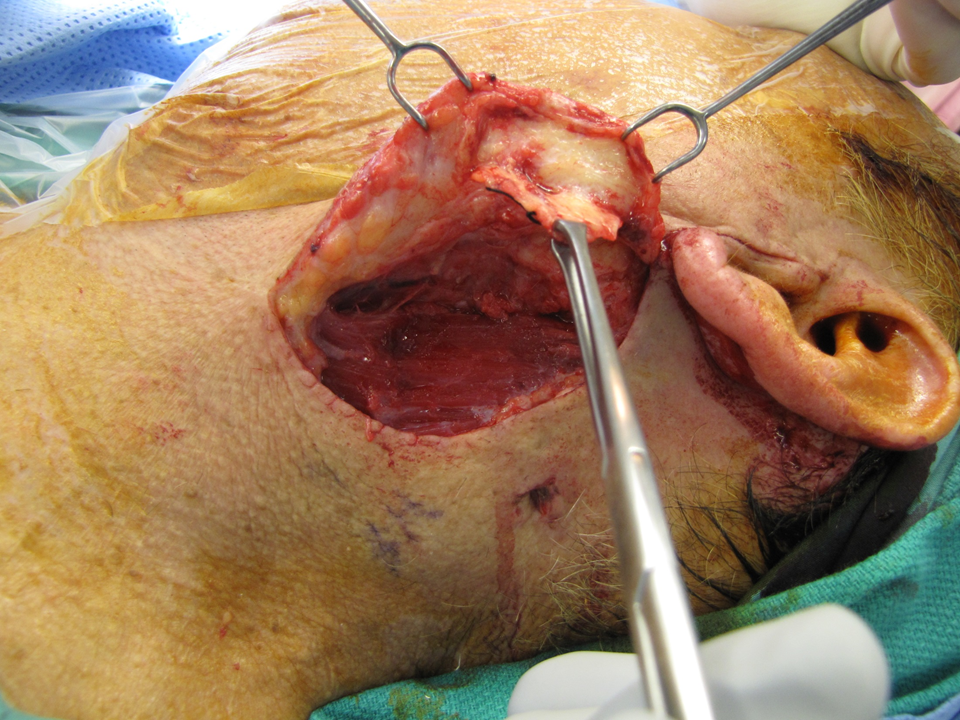
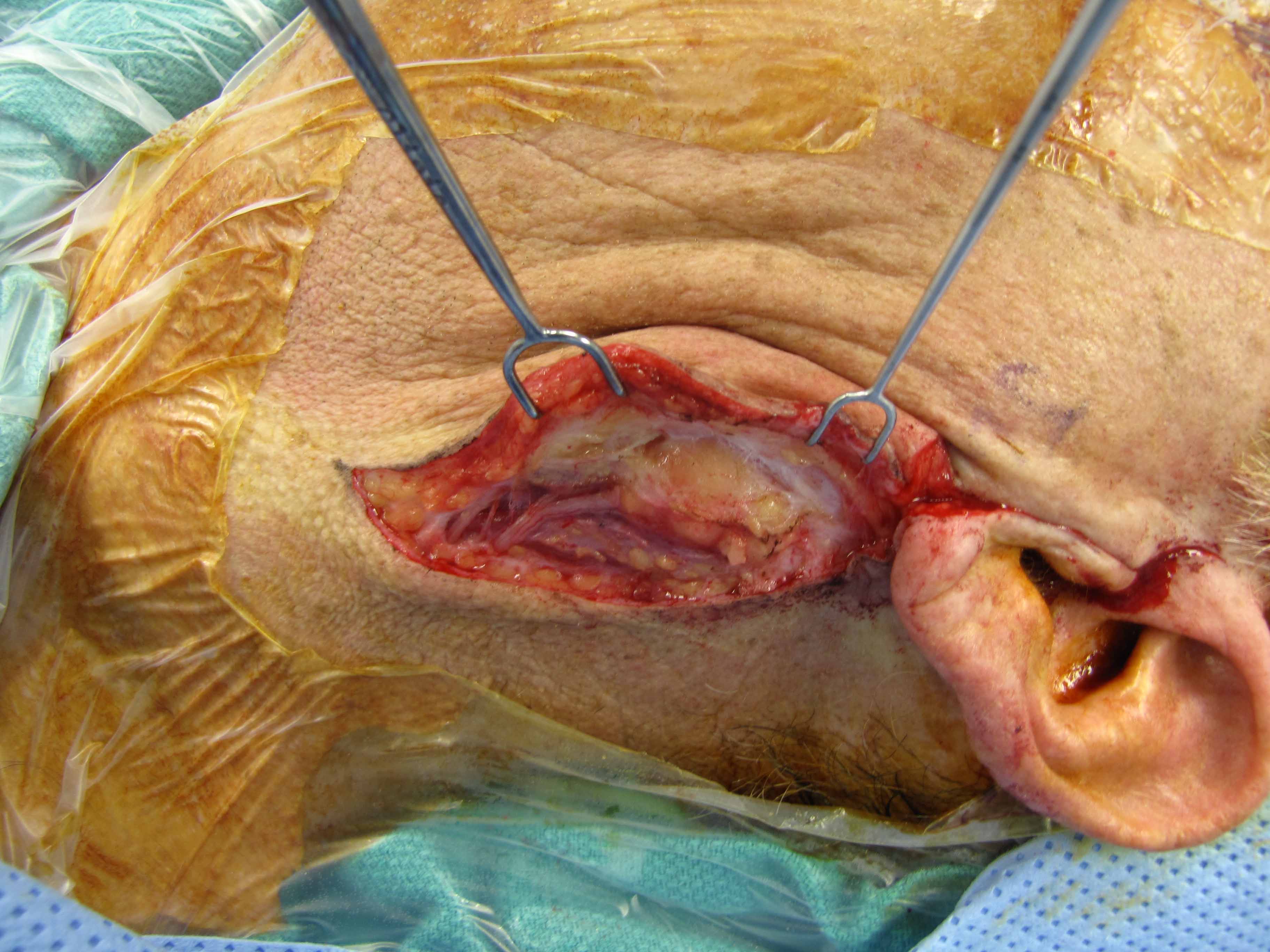
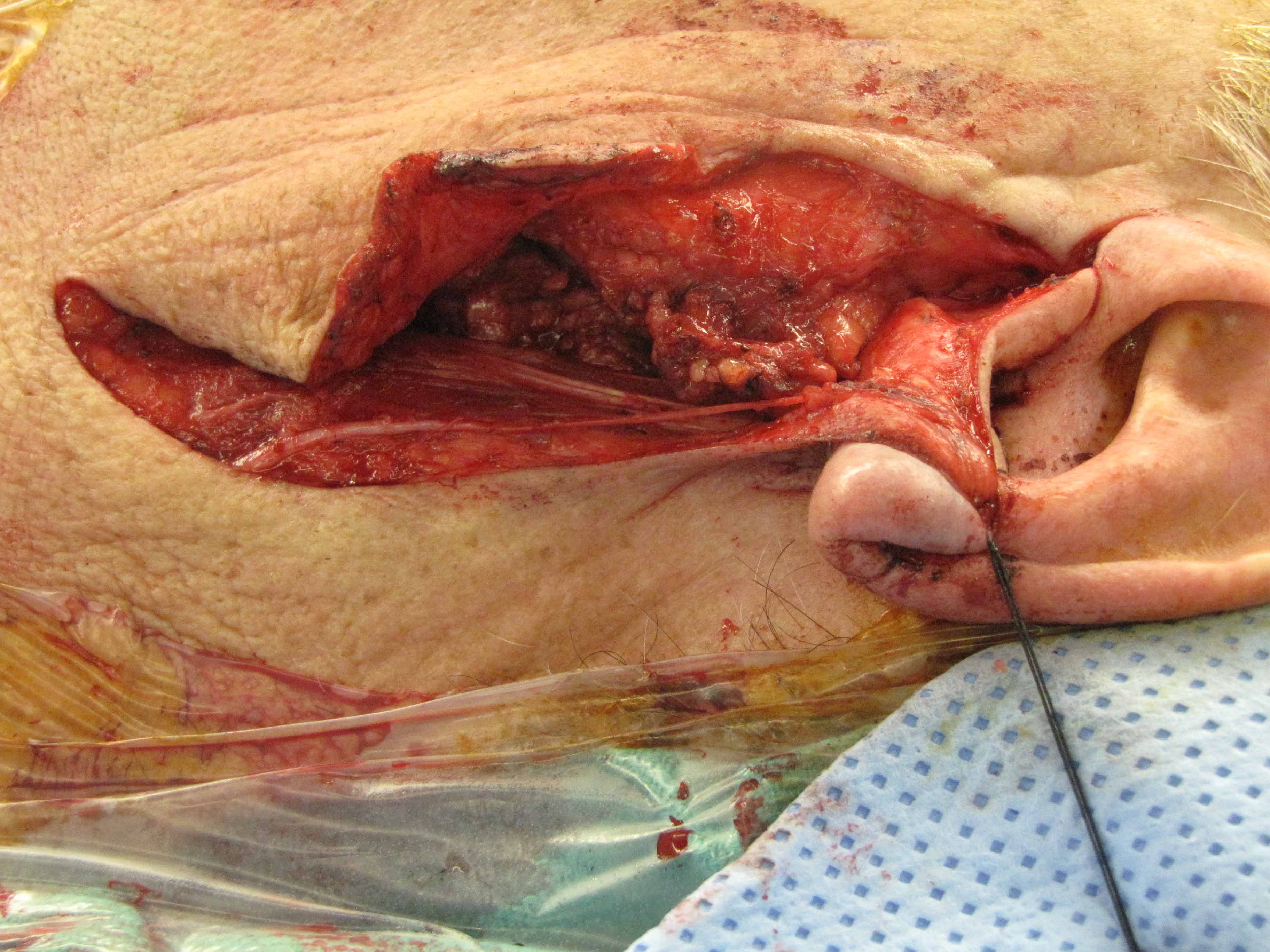
1st Resection (Parotidectomy with facial nerve dissection,
preservation of great auricular nerve):




Comment: This lipomatous tumor shows nuclear pleomorphism and irregularity, and
given the sub-fascial location, the tumor is best interpreted as
lipoma-like liposarcoma. This low-grade tumor may have a small risk of
local reoccurrence given the close lateral margin. Spindle cell lipoma was
also a consideration, however the CD34 stain is negative.
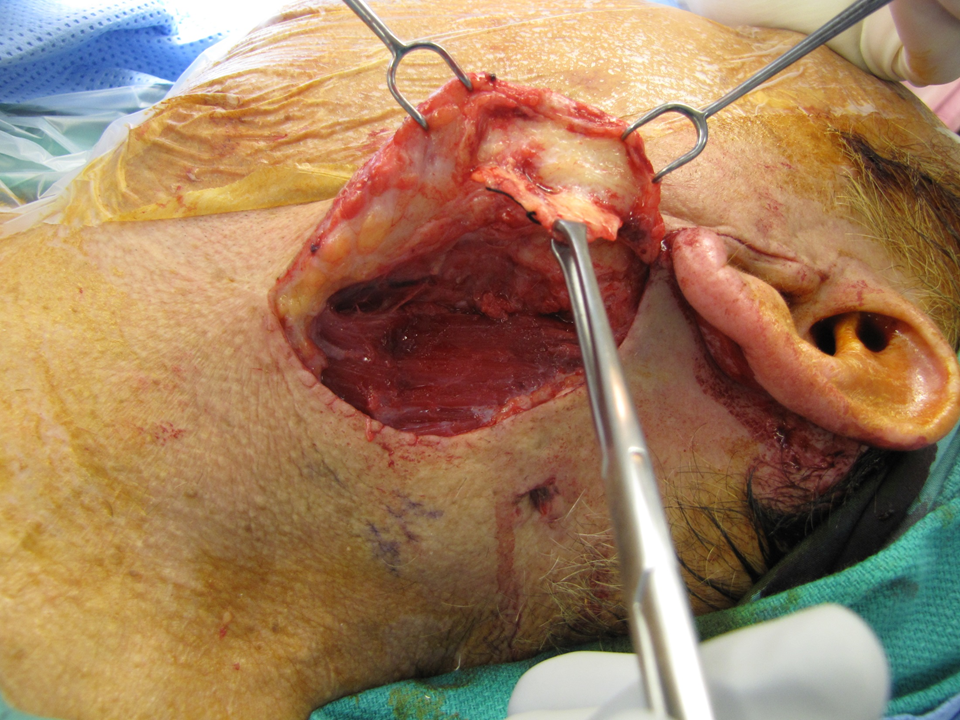
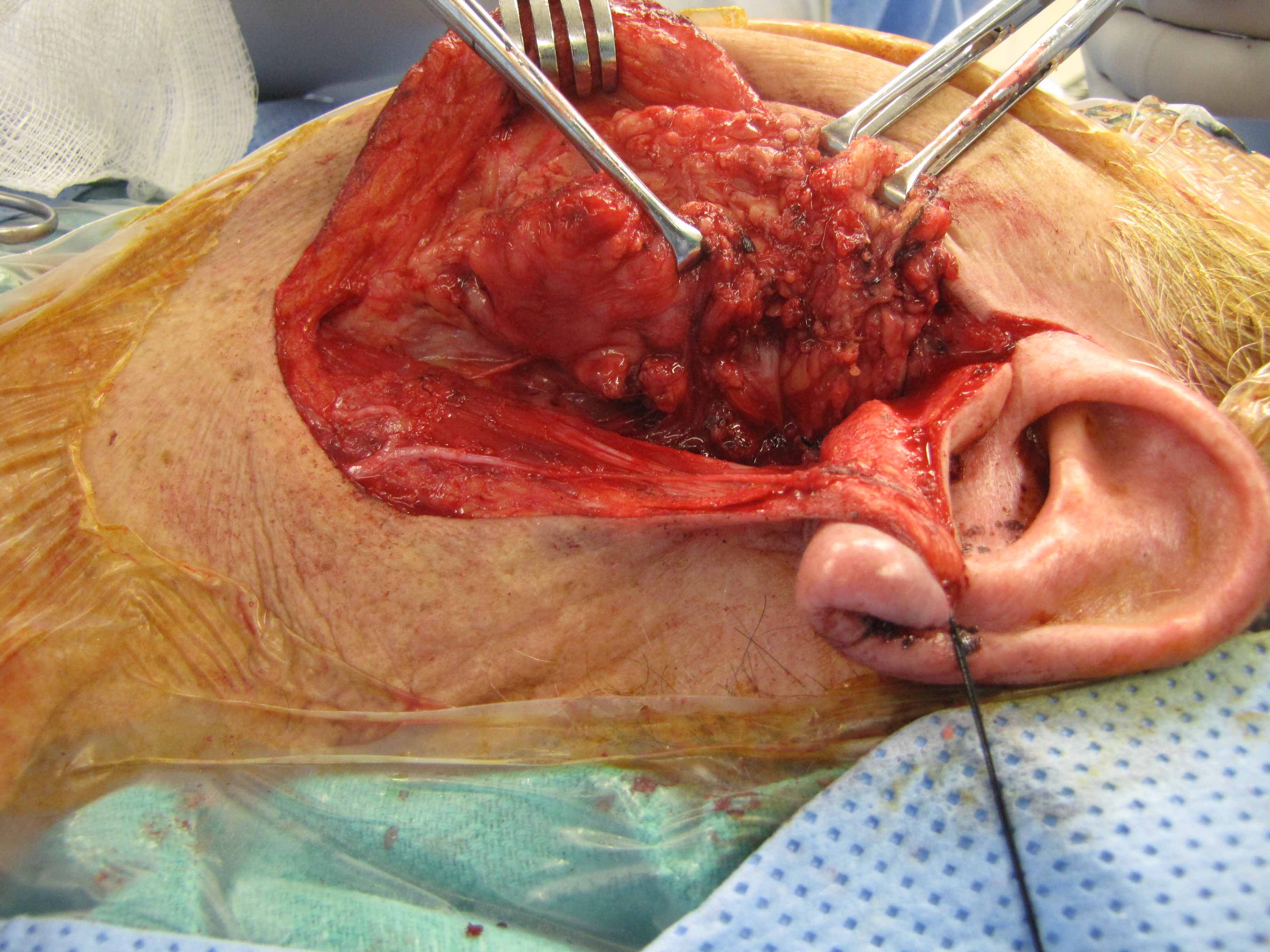
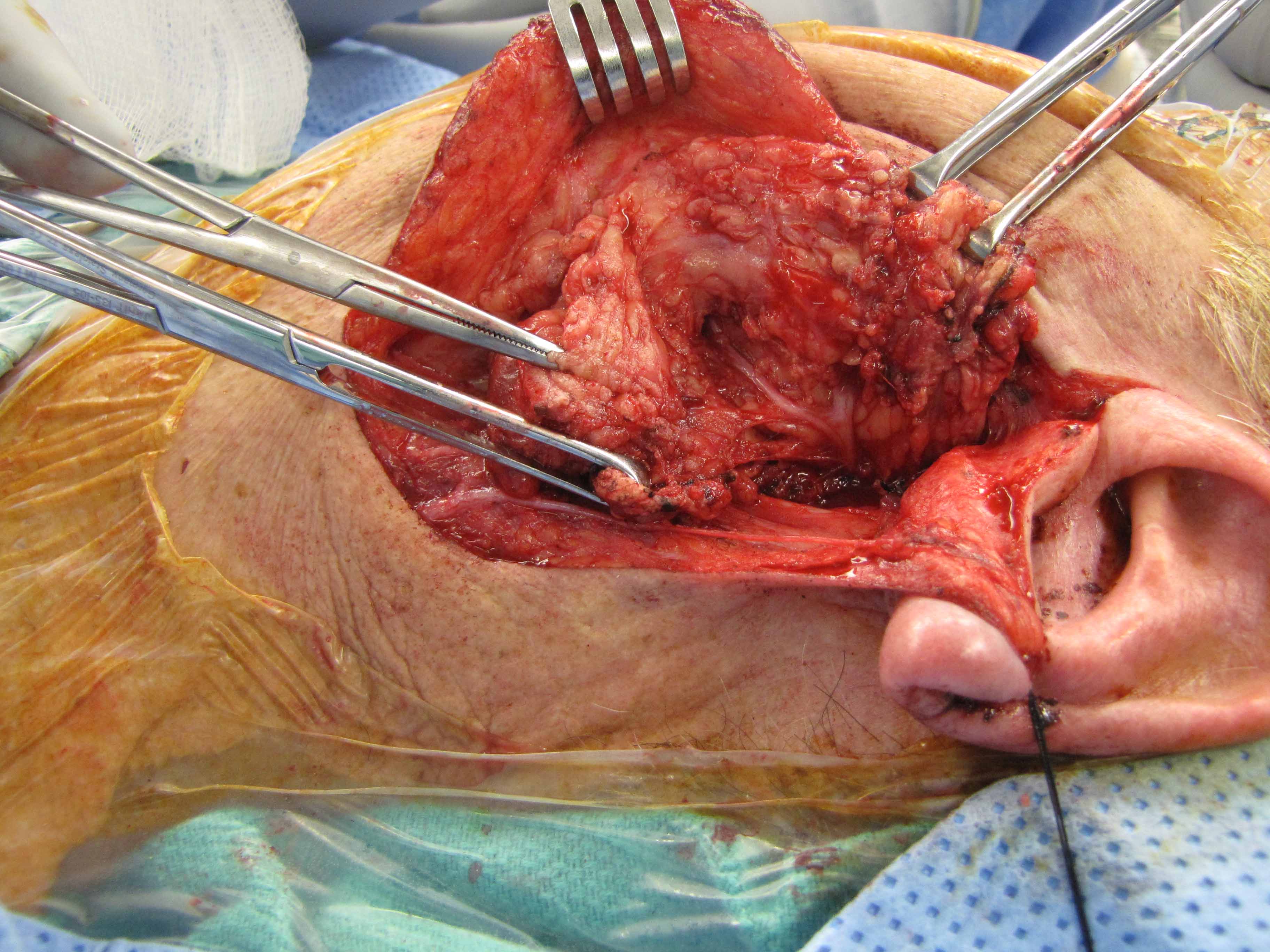
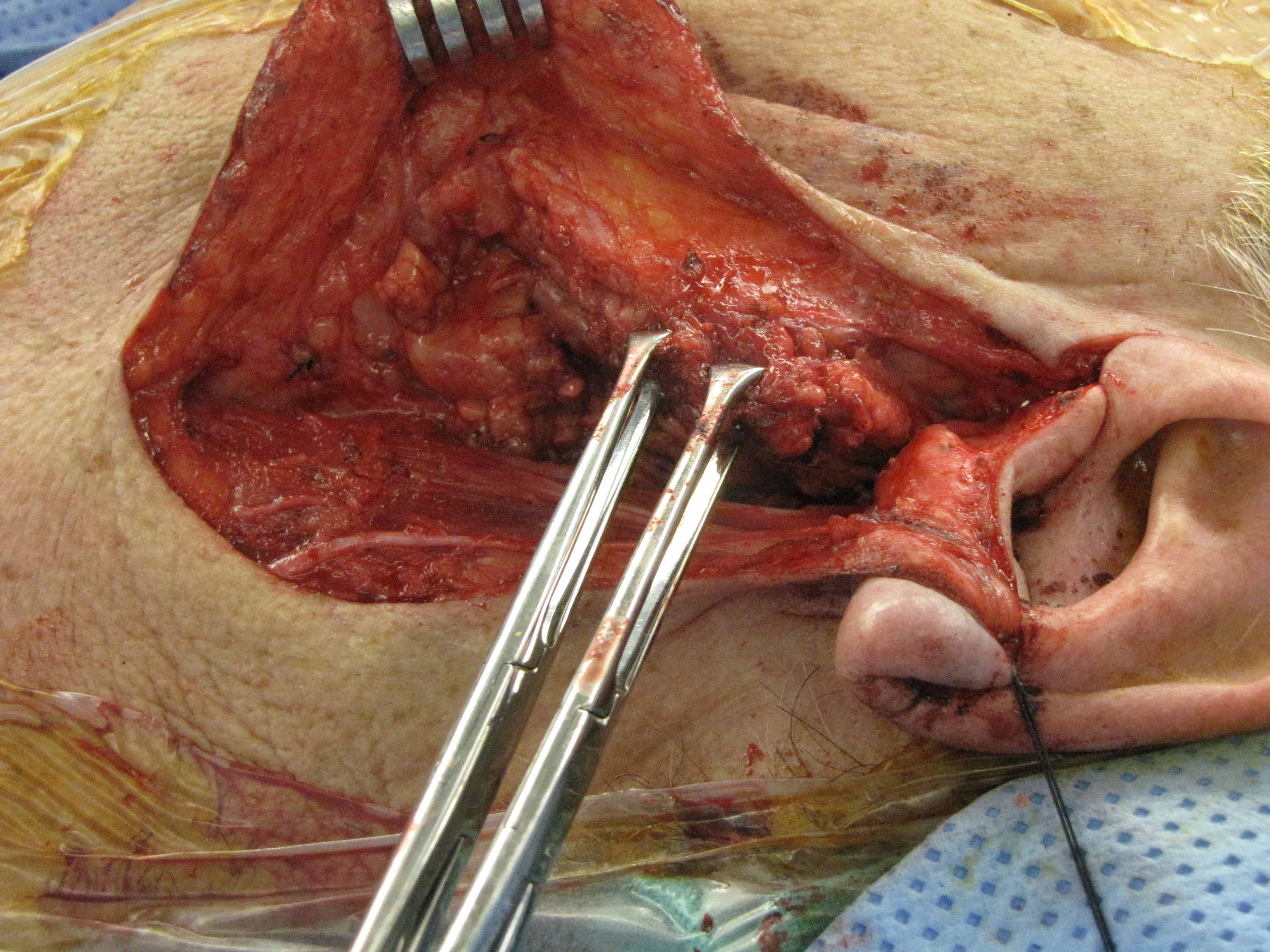
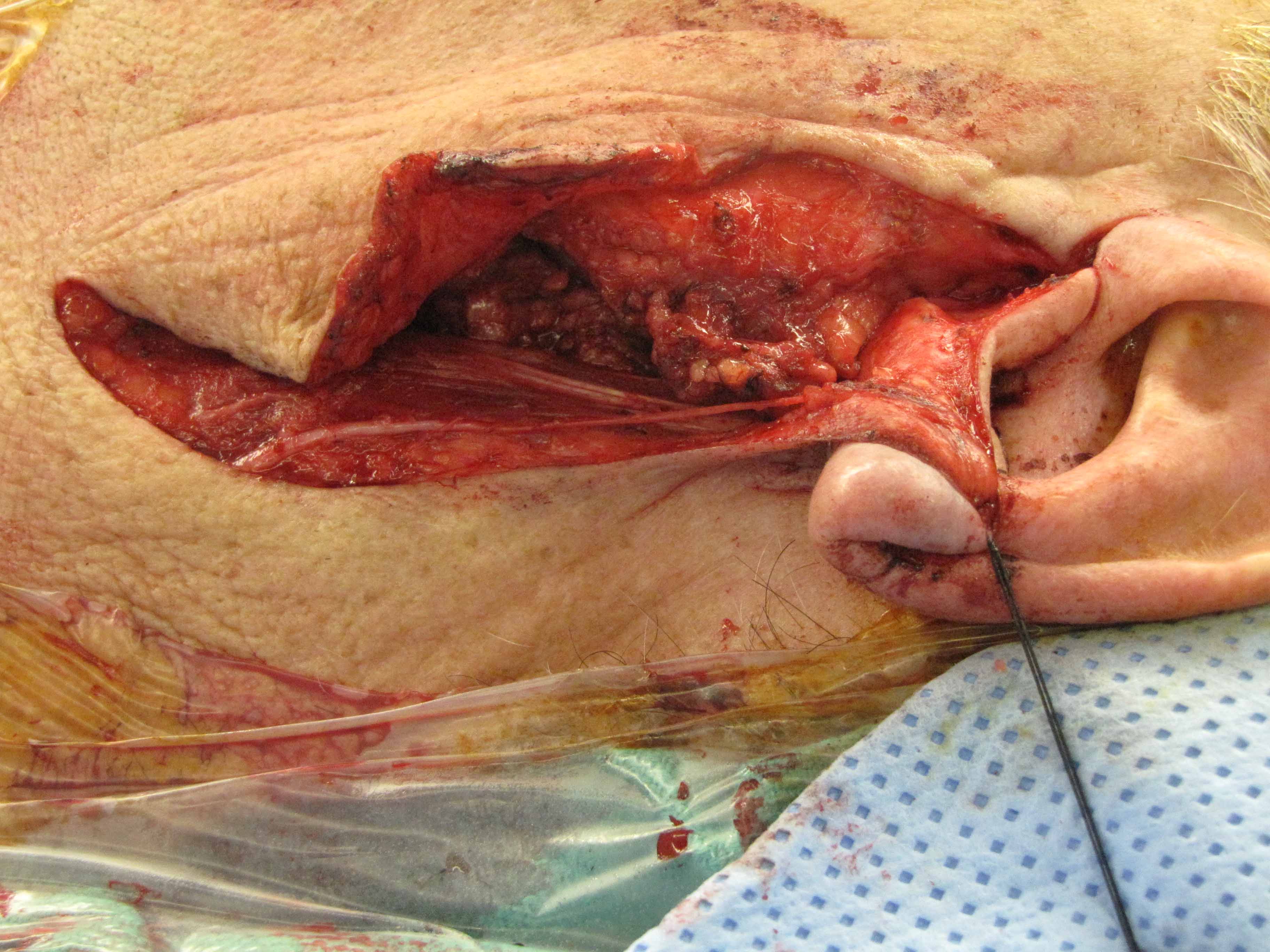
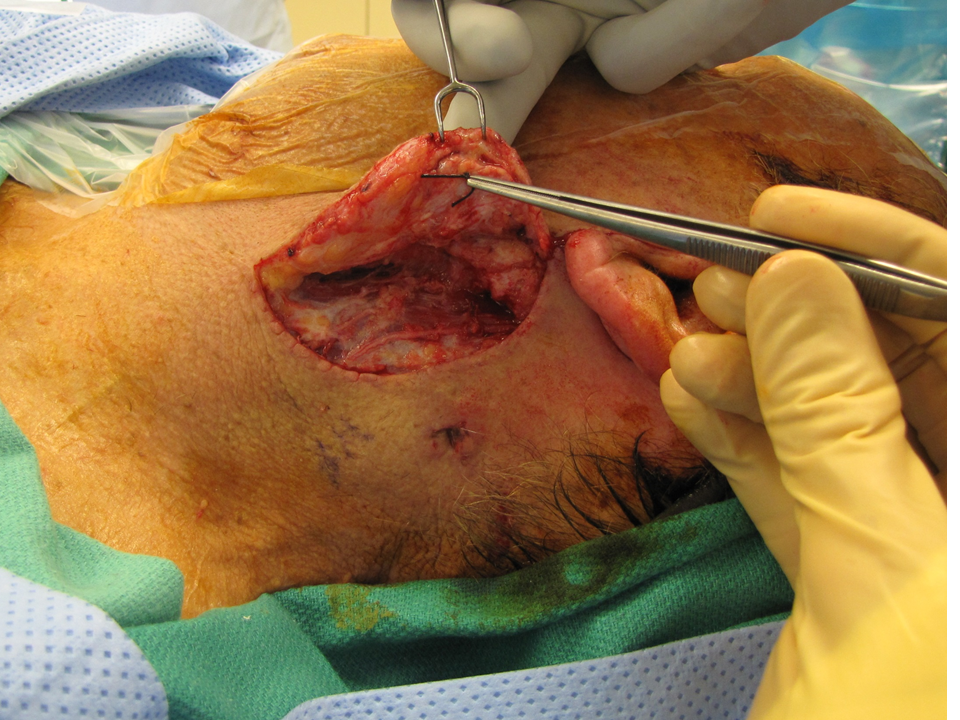
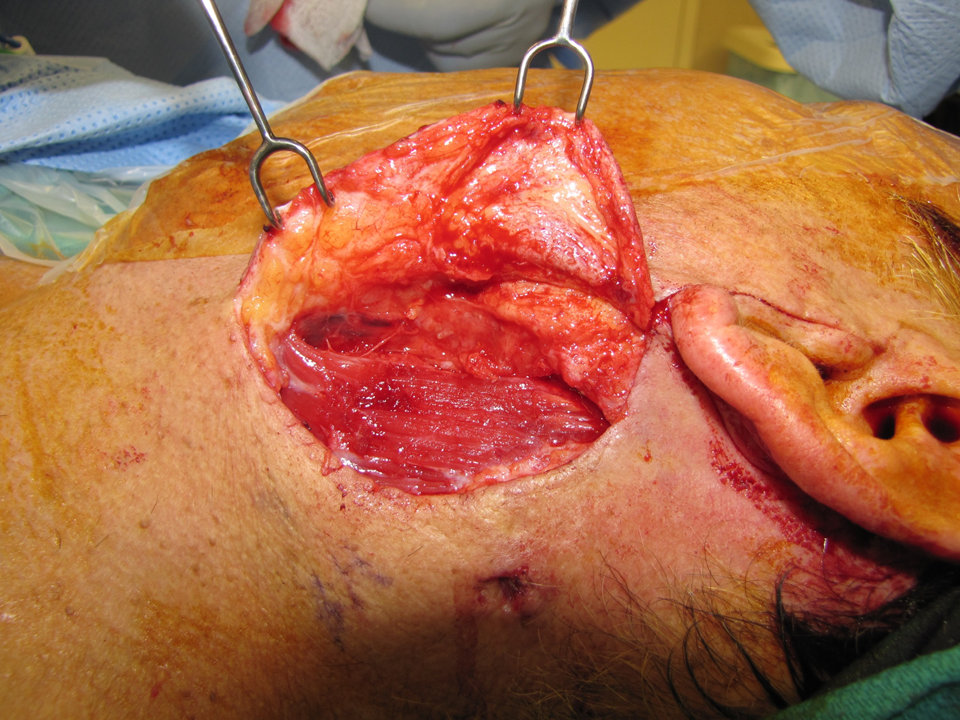
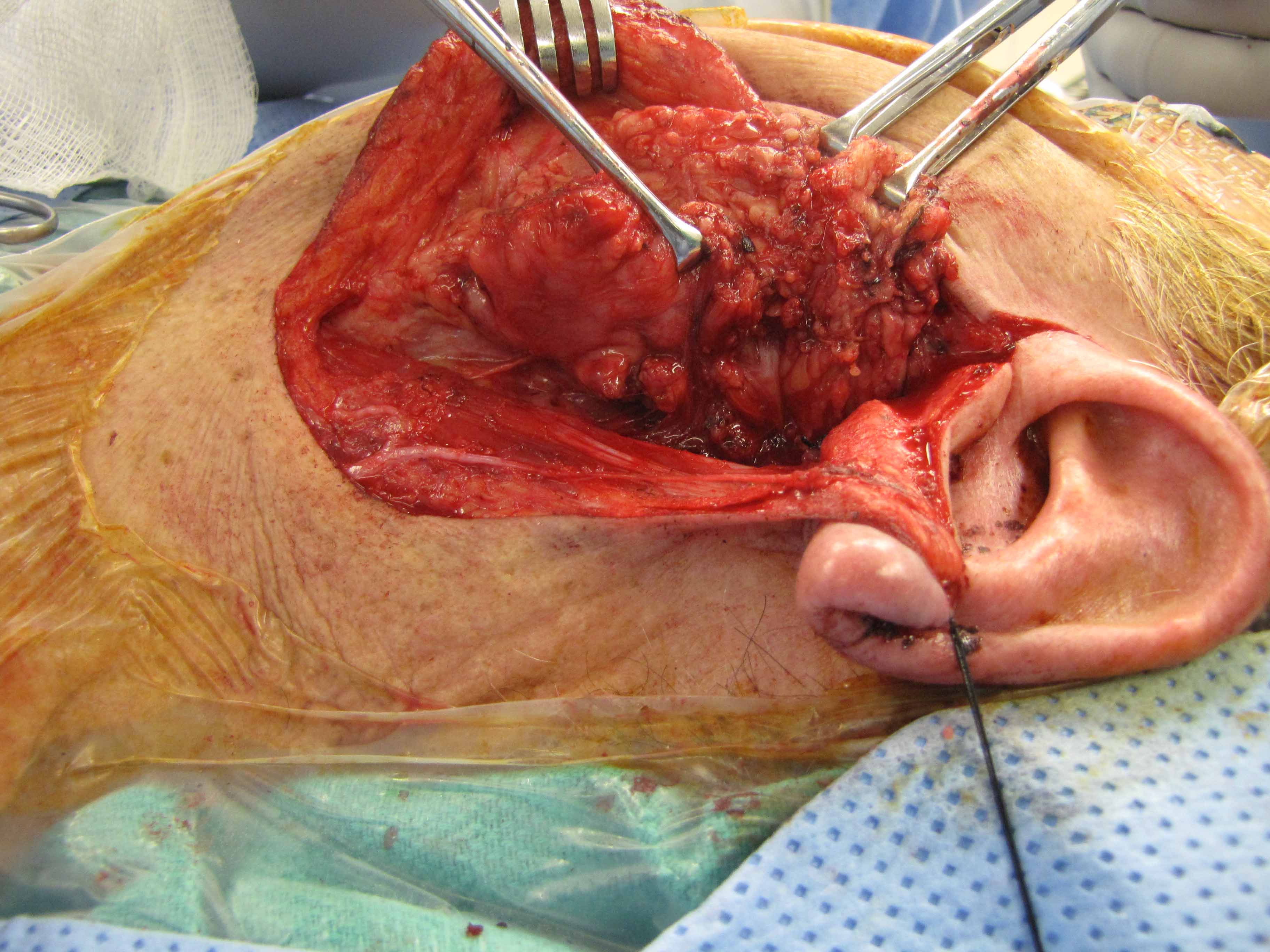
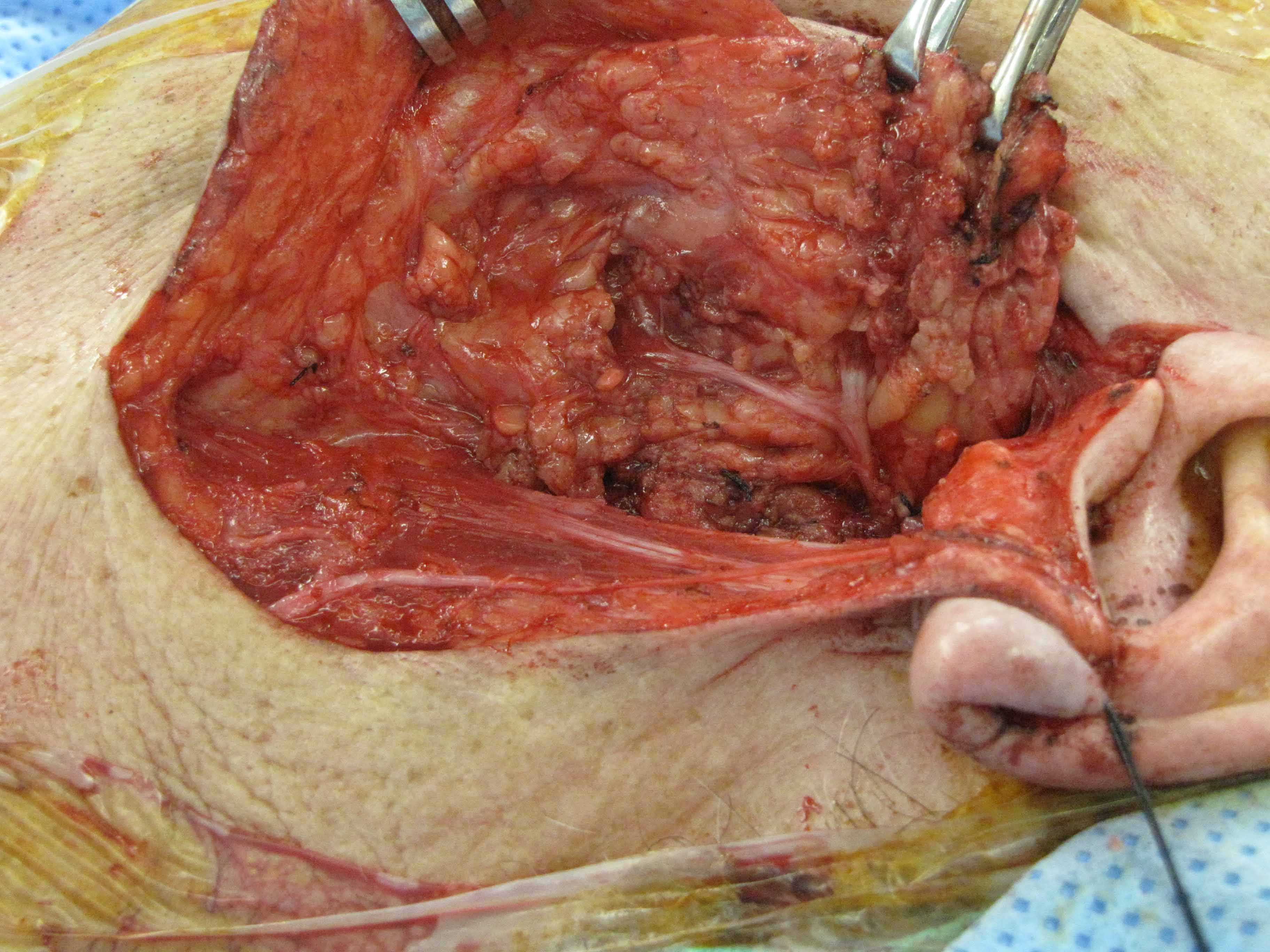
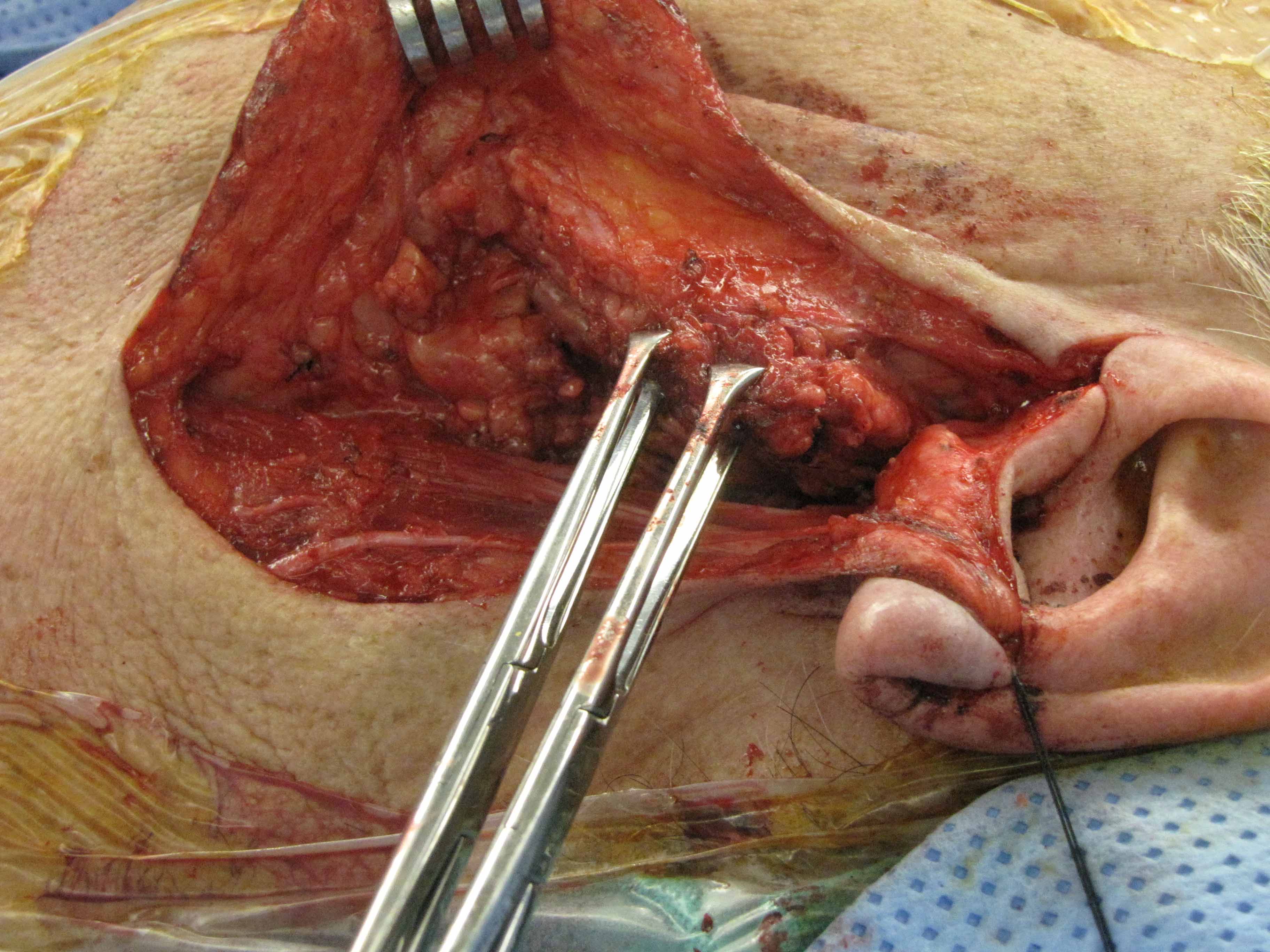
Second resection 7 days later to clear positive margins
(sacrifice of great auricular nerve):