
Pediatric Vital Signs Normal Ranges Summary Table:
-
Values were derived from numerous sources (listed below) and reflect the guidelines determined to be up-to-date as of May 20, 2020. Normal ranges may include measurements that deviate from these values. Note that the patient's normal range and clinical condition should always be considered.
(Flynn, Kaelber et al. 2017, National High Blood Pressure Education Program Working Group on High Blood Pressure in and Adolescents 2004, Xi, Zong et al. 2016, Morgan & Mikhail's Clinical Anesthesiology, Chapter 42. Pediatric Anesthesia)
|
*Age Group (weight in kg) |
Age (years) |
Height (cm) |
Blood pressure (mmHg) (50th-90th percentile) |
Respiratory Rate |
Heart Rate |
||||
|
Boys |
Girls |
Awake |
Sleeping |
||||||
|
Systolic |
Diastolic |
Systolic |
Diastolic |
||||||
|
Infant |
1-12 months |
|
72 -104 |
37-56 |
72-104 |
37-56 |
30-60 |
100-170 |
75-160 |
|
Toddler (10-14 Kg) |
1 |
77-87 |
86-101 |
41-54 |
85-102 |
42-58 |
24-40 |
80-150 |
60-90 |
|
2 |
86-98 |
89-104 |
44-58 |
89-106 |
48-62 |
||||
|
Preschooler (14-18Kg) |
3 |
92-105 |
90-105 |
47-61 |
90-107 |
50-65 |
20-34 |
70-130 |
|
|
4 |
98-113 |
92-107 |
50-64 |
92-108 |
53-67 |
||||
|
5 |
104-120 |
94-110 |
53-67 |
93-110 |
55-70 |
||||
|
School-age (20-42 Kg) |
6 |
111-127 |
90-109 |
59-73 |
91-108 |
59-73 |
15-30 |
65-120 |
|
|
7 |
116-134 |
91-111 |
60-74 |
92-110 |
60-74 |
||||
|
8 |
120-140 |
93-113 |
60-75 |
94-112 |
60-75 |
||||
|
9 |
125-145 |
94-115 |
61-75 |
95-114 |
61-76 |
||||
|
10 |
130-151 |
96-117 |
62-76 |
97-116 |
62-77 |
||||
|
11 |
135-157 |
98-119 |
62-77 |
99-118 |
63-78 |
||||
|
12 |
141-164 |
100-121 |
63-78 |
100-120 |
64-78 |
||||
|
Adolescent (50 Kg) |
>13 |
147-172 |
102-124 |
64-80 |
102-121 |
64-79 |
12-20 |
55-90 |
50-90 |
* For Newborn infants, BP values vary considerably during the first few weeks of life and the definition of HTN in preterm and term neonates also varies. Data have been compiled on neonatal BP values and the summary table is available. Please note that no alternative data have been developed recently. For further information, please see the following articles:
Dionne, J. M., et al. (2012). "Hypertension in infancy: diagnosis, management, and outcome." Pediatr Nephrol 27(1): 17-32.
Dionne, J. M., et al. (2017). "Hypertension Canada's 2017 Guidelines for the Diagnosis, Assessment, Prevention, and Treatment of Pediatric Hypertension." Can J Cardiol 33(5): 577-585.
"Report of the Second Task Force on Blood Pressure Control in Children--1987. Task Force on Blood Pressure Control in Children. National Heart, Lung, and Blood Institute, Bethesda, Maryland." Pediatrics 79(1): 1-25.
When to start screening for high BP and how often?
(National High Blood Pressure Education Program Working Group on High Blood Pressure in and Adolescents 2004)
- Guidelines suggest that the blood pressure of children should be assessed starting at 3 years of age. (Grade C, moderate recommendation)
- Children less than 3 years of age should have their BP checked under special conditions including a history of prematurity, congenital heart disease malignancy and other systemic illnesses (Grade C, moderate recommendation)
Hypertension (HTN) or High Blood Pressure
(Chen and Wang 2008, Chiolero, Cachat et al. 2007, McNiece, Poffenbarger et al. 2007, National High Blood Pressure Education Program Working Group on High Blood Pressure in and Adolescents 2004, Weaver 2019)
- What is the definition of HTN?
- High blood pressure is defined as average systolic BP and/or diastolic BP >/= 95th percentile for age, gender and height on more than 3 occasions.
- Pre-hypertension is defined as SBP and/or DBP between 90th and 95th percentile.
- For adolescents, BP readings >/= 120/80 are considered to be pre-hypertensive.
- How prevalent is HTN in Children?
- The prevalence of clinical HTN in children and adolescent is ~3.5%
- The prevalence of persistent HTN is ~2.2% to 3.5%
- Higher rates are present among overweight and obese children and adolescents.
- Does HTN in children track into HTN in adulthood?
- Data on BP tracking suggest that higher BP in childhood correlates with higher BP in adulthood
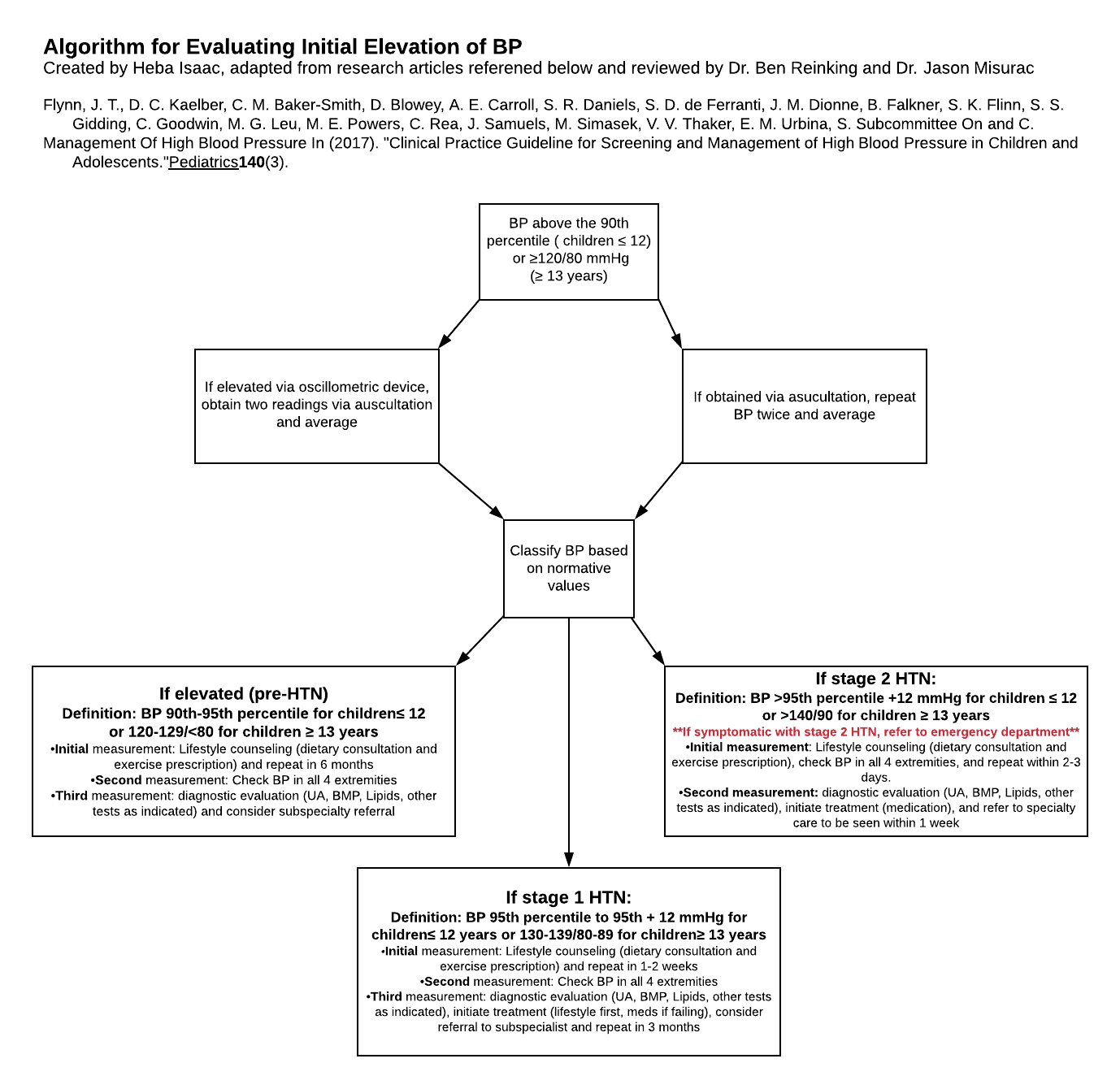
A Summary of Pediatric BP Categories, Stages and Follow-Up
- The table was recreated from the articles listed below. Given that there were slight variations in BP values, we elected to include both percentiles and BP ranges.
(National High Blood Pressure Education Program Working Group on High Blood Pressure in and Adolescents 2004, Chen and Wang 2008, Banker, Bell et al. 2016, Flynn, Kaelber et al. 2017, Weaver 2017, Weaver 2019)
|
|
Age <13 years |
Age>13 years |
Follow-up |
|---|---|---|---|
|
Elevated or persistent or pre-HTN |
90th to 95th percentile or 120/80 mm Hg to <95th percentile (whichever is lower) |
120-129/<80 mm Hg |
Recheck in 6 months Consider school or home BP monitoring |
|
Stage 1 HTN |
>95th to 99th percentile + 5 mmHg or 130-139/89 mm Hg (whichever is lower) |
130-139/89 mm Hg |
Evaluate in 1 week to 1 month |
|
Stage 2 HTN |
> 99th percentile + 5 mm Hg or >/=140/90 mm Hg (whichever is lower) |
>/=140/90 mm Hg |
Evaluate in 1 week or sooner if symptomatic |
|
White-coat HTN |
> 95th percentile in a medical setting. Normal outside the medical setting |
Consider ABPM as well as home or school BP monitoring |
|
|
Masked HTN |
< 95th percentile in a medical setting. > 95th percentile outside a medical setting |
Consider ABPM in high-risk patients. |
|
Obtaining Accurate Blood Pressure Measurements:
(Scott, Rocchini et al. 1988, Pickering, Hall, et al. 2005)
- Different methods to measure Blood pressure: The mercury sphygmomanometer is the gold standard device for in-office blood pressure measurement
- The Auscultatory method
- The most widely used noninvasive method for measuring blood pressure.
- The preferred method for BP measurement in children
- Korotkoff technique
- Discovered by Dr. Nikolai Korotkov over 100 years ago.
- It involves blocking the brachial artery by inflating a cuff to above systolic blood pressure and gradually deflate to re-establish blood flow.
- The sounds detected by the stethoscope are known as Korotkoff sounds and are generally classified as phases I -V.
- Phase I appears as a tapping sound and corresponds to systolic blood pressure
- Phase V (disappearance of sound) corresponds to diastolic blood pressure (Pickering, Hall et al. 2005).
- The oscillometric method:
- The SBP and DBP are estimated indirectly by measuring the mean arterial pressure.
- Not commonly used as ambulatory blood pressure monitors.
- Advantages:
- No transducer is needed and therefore, the placement of the cuff is not critical
- Convenient and minimize observer error
- Current guidelines suggest that if blood pressure reading exceeds the 90th percentile, it should be confirmed by the auscultatory method.
- The Auscultatory method
- Location of measurement:
- The upper arm is the standard location for blood pressure measurement. Wrist monitors can be used in obese patients because wrist diameter is not significantly affected by obesity
- Subject preparation: For most accurate blood pressure measurements, the American Heart Association recommends the following:
- Sitting quietly for at least 5 minutes.
- The child should be seated comfortably in a chair with back supported and legs uncrossed.
- An unsupported back may result in an increase in diastolic blood pressure
- Crossing the legs may increase systolic blood pressure.
- Remove all clothing that covers the location of cuff placement
- child’s arm should be supported at heart level
- the right arm is preferred due to the possibility of coarctation of the aorta, which may result in a falsely low reading (Scott, Rocchini et al. 1988)
- Cuff size:
- The ideal cuff size is one with a bladder length of 80% and a width that is at least 40% of arm circumference
- Using a cuff that is too narrow will result in inappropriately high blood pressure. whereas a cuff that is too wide will result in an inappropriately low blood pressure reading.
- Below are recommended BP cuff sizes for children and adolescents for a range of arm circumference.
- The table recreated from numerous sources listed below. Slight variations were noted.
- (Mattoo 2002, National High Blood Pressure Education Program Working Group on High Blood Pressure in and Adolescents 2004, Pickering, Hall et al. 2005, Prineas, Ostchega et al. 2007, Palatini and Frick 2012, Ostchega, Hughes, et al. 2014, Weaver 2017, Ostchega, Hughes, et al. 2018)
|
BP Cuff |
Arm Circumference (cm) |
|---|---|
|
Newborn |
10 |
|
Infant |
11 – 15 |
|
Child |
16 – 22 |
|
Small Adult |
23 – 26 |
|
Adult |
27 – 34 |
|
Large Adult |
35 – 44 |
|
Thigh |
45 – 52 |
Childhood Obesity and its Effects on Blood Pressure
- It is noteworthy that the increasing prevalence of obesity in the United States has not only affected adults but also children. As a result, population-based studies of pediatric weight will vary according to the period to time sampled - and will also affect (as per Keefe 2019) - the prevalence of sleep apnea with its related impact on hypertension.
- The prevalence of childhood obesity has significantly increased since 1980 with approximately 30% of children who are overweight/obese (Ogden, Carroll et al. 2015).
- Children with high BMI are more likely to develop hypertension later in life compared to children with lower BMI (Parker, Sinaiko et al. 2016)
- With the unfortunate rising rates of childhood obesity, obtaining an accurate measurement has proven to be challenging due to an abnormally large arm circumference:
- Arm circumference can be large enough which requires the use of adult size BP cuff
- NHANES data from 2007-2010 showed that boys and girls as young as 9 years of age required a standard adult-sized cuff. Additionally, of obese participants, one third required a large adult BP cuff (Palatini and Frick 2012)
- Disproportionately short arm compared to the cuff required for a given arm circumference
- Conically shaped arms resulting in an average difference of 8.7 cm between the proximal and distal upper arm circumference (Palatini and Frick 2012)
- Pathophysiology: (Stefan, Vozarova et al. 2002, Rasouli and Kern 2008, do Carmo, da Silva et al. 2011, Kalil and Haynes 2012, Brambilla, Antolini et al. 2013, Vecchiola, Lagos et al. 2016, Brady 2017)
- Increased adiposity leads to dysfunctional activation of the sympathetic nervous system:
- Increased adipose tissue results in an increased production of adipokines (pro- and anti-inflammatory hormones and cytokines) to maintain homeostasis
- Recent research has been focused on the role of adiponectin (AD) due to its anti-inflammatory and anti-atherogenic effects as well as its role in increasing insulin sensitivity
- Over time, the disproportionate increase in pro-inflammatory adipokines (IL-6, leptin, etc.) leads to a chronic inflammatory state
- For example, Leptin’s activation of SNS is mediated via leptin receptors present on POMC neurons in the brain
- Increased adipose tissue results in an increased production of adipokines (pro- and anti-inflammatory hormones and cytokines) to maintain homeostasis
- The activation of SNS leads to increased norepinephrine production resulting in elevated BP via the following mechanisms
- Increased activity of RAAS and release of renin.
- Direct vasoconstricting effects
- Chronic inflammation and increased oxidative stress lead to endothelial damage and vascular dysfunction which manifests clinically as hypertension.
- Increased adiposity leads to dysfunctional activation of the sympathetic nervous system:
References:
Banker, A., C. Bell, M. Gupta-Malhotra and J. Samuels (2016). "Blood pressure percentile charts to identify high or low blood pressure in children." BMC Pediatr 16: 98.
Brady, T. M. (2017). "Obesity-Related Hypertension in Children." Front Pediatr 5: 197.
Brambilla, P., L. Antolini, M. E. Street, M. Giussani, S. Galbiati, M. G. Valsecchi, A. Stella, G. V. Zuccotti, S. Bernasconi and S. Genovesi (2013). "Adiponectin and hypertension in normal-weight and obese children." Am J Hypertens 26(2): 257-264.
Chen, X. and Y. Wang (2008). "Tracking of blood pressure from childhood to adulthood: a systematic review and meta-regression analysis." Circulation 117(25): 3171-3180.
Chiolero, A., F. Cachat, M. Burnier, F. Paccaud and P. Bovet (2007). "Prevalence of hypertension in schoolchildren based on repeated measurements and association with overweight." Journal of hypertension 25(11): 2209-2217.
Coulthard, M. G. (2020). "Single blood pressure chart for children up to 13 years to improve the recognition of hypertension based on existing normative data." Arch Dis Child.
do Carmo, J. M., A. A. da Silva, Z. Cai, S. Lin, J. H. Dubinion and J. E. Hall (2011). "Control of blood pressure, appetite, and glucose by leptin in mice lacking leptin receptors in proopiomelanocortin neurons." Hypertension 57(5): 918-926.
Flynn, J. T., D. C. Kaelber, C. M. Baker-Smith, D. Blowey, A. E. Carroll, S. R. Daniels, S. D. de Ferranti, J. M. Dionne, B. Falkner, S. K. Flinn, S. S. Gidding, C. Goodwin, M. G. Leu, M. E. Powers, C. Rea, J. Samuels, M. Simasek, V. V. Thaker, E. M. Urbina, S. Subcommittee On and C. Management Of High Blood Pressure In (2017). "Clinical Practice Guideline for Screening and Management of High Blood Pressure in Children and Adolescents." Pediatrics 140(3).
Kalil, G. Z. and W. G. Haynes (2012). "Sympathetic nervous system in obesity-related hypertension: mechanisms and clinical implications." Hypertens Res 35(1): 4-16.
Mattoo, T. K. (2002). "Arm cuff in the measurement of blood pressure." Am J Hypertens 15(2 Pt 2): 67S-68S.
McNiece, K. L., T. S. Poffenbarger, J. L. Turner, K. D. Franco, J. M. Sorof and R. J. Portman (2007). "Prevalence of hypertension and pre-hypertension among adolescents." The Journal of pediatrics 150(6): 640-644. e641.
National High Blood Pressure Education Program Working Group on High Blood Pressure in, C. and Adolescents (2004). "The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents." Pediatrics 114(2 Suppl 4th Report): 555-576.
Ogden, C. L., M. D. Carroll, C. D. Fryar and K. M. Flegal (2015). "Prevalence of Obesity Among Adults and Youth: United States, 2011-2014." NCHS Data Brief(219): 1-8.
Ostchega, Y., J. P. Hughes, T. Nwankwo and G. Zhang (2018). "Mean mid-arm circumference and blood pressure cuff sizes for US children, adolescents and adults: National Health and Nutrition Examination Survey, 2011-2016." Blood Press Monit 23(6): 305-311.
Ostchega, Y., J. P. Hughes, R. J. Prineas, G. Zhang, T. Nwankwo and M. M. Chiappa (2014). "Mid-arm circumference and recommended blood pressure cuffs for children and adolescents aged between 3 and 19 years: data from the National Health and Nutrition Examination Survey, 1999-2010." Blood Press Monit 19(1): 26-31.
Palatini, P. and G. N. Frick (2012). "Cuff and bladder: overlooked components of BP measurement devices in the modern era?" Am J Hypertens 25(2): 136-138.
Parker, E. D., A. R. Sinaiko, E. O. Kharbanda, K. L. Margolis, M. F. Daley, N. K. Trower, N. E. Sherwood, L. C. Greenspan, J. C. Lo, D. J. Magid and P. J. O'Connor (2016). "Change in Weight Status and Development of Hypertension." Pediatrics 137(3): e20151662.
Pickering, T. G., J. E. Hall, L. J. Appel, B. E. Falkner, J. Graves, M. N. Hill, D. W. Jones, T. Kurtz, S. G. Sheps and E. J. Roccella (2005). "Recommendations for blood pressure measurement in humans and experimental animals: part 1: blood pressure measurement in humans: a statement for professionals from the Subcommittee of Professional and Public Education of the American Heart Association Council on High Blood Pressure Research." Circulation 111(5): 697-716.
Pickering, T. G., J. E. Hall, L. J. Appel, B. E. Falkner, J. W. Graves, M. N. Hill, D. H. Jones, T. Kurtz, S. G. Sheps, E. J. Roccella, P. Council on High Blood Pressure Research and A. H. A. Public Education Subcommittee (2005). "Recommendations for blood pressure measurement in humans: an AHA scientific statement from the Council on High Blood Pressure Research Professional and Public Education Subcommittee." J Clin Hypertens (Greenwich) 7(2): 102-109.
Prineas, R. J., Y. Ostchega, M. Carroll, C. Dillon and M. McDowell (2007). "US demographic trends in mid-arm circumference and recommended blood pressure cuffs for children and adolescents: data from the National Health and Nutrition Examination Survey 1988-2004." Blood Press Monit 12(2): 75-80.
Rasouli, N. and P. A. Kern (2008). "Adipocytokines and the metabolic complications of obesity." J Clin Endocrinol Metab 93(11 Suppl 1): S64-73.
Scott, W. A., A. P. Rocchini, E. L. Bove, D. M. Behrendt, R. H. Beekman, M. Dick, 2nd, G. Serwer, R. Snider and A. Rosenthal (1988). "Repair of interrupted aortic arch in infancy." J Thorac Cardiovasc Surg 96(4): 564-568.
Stefan, N., B. Vozarova, T. Funahashi, Y. Matsuzawa, C. Weyer, R. S. Lindsay, J. F. Youngren, P. J. Havel, R. E. Pratley, C. Bogardus and P. A. Tataranni (2002). "Plasma adiponectin concentration is associated with skeletal muscle insulin receptor tyrosine phosphorylation, and low plasma concentration precedes a decrease in whole-body insulin sensitivity in humans." Diabetes 51(6): 1884-1888.
Vecchiola, A., C. F. Lagos, C. A. Carvajal, R. Baudrand and C. E. Fardella (2016). "Aldosterone Production and Signaling Dysregulation in Obesity." Curr Hypertens Rep 18(3): 20.
Weaver, D. J., Jr. (2017). "Hypertension in Children and Adolescents." Pediatr Rev 38(8): 369-382.
Weaver, D. J., Jr. (2019). "Pediatric Hypertension: Review of Updated Guidelines." Pediatr Rev 40(7): 354-358.
Xi, B., X. Zong, R. Kelishadi, Y. M. Hong, A. Khadilkar, L. M. Steffen, T. Nawarycz, M. Krzywinska-Wiewiorowska, H. Aounallah-Skhiri, P. Bovet, A. Chiolero, H. Pan, M. Litwin, B. K. Poh, R. Y. Sung, H. K. So, P. Schwandt, G. M. Haas, H. K. Neuhauser, L. Marinov, S. V. Galcheva, M. E. Motlagh, H. S. Kim, V. Khadilkar, A. Krzyzaniak, H. B. Romdhane, R. Heshmat, S. Chiplonkar, B. Stawinska-Witoszynska, J. El Ati, M. Qorbani, N. Kajale, P. Traissac, L. Ostrowska-Nawarycz, G. Ardalan, L. Parthasarathy, M. Zhao, T. Zhang and C. International Child Blood Pressure References Establishment (2016). "Establishing International Blood Pressure References Among Nonoverweight Children and Adolescents Aged 6 to 17 Years." Circulation 133(4): 398-408.