see also: Esophageal Reflux Precautions; Singers Packet (Voice Clinic Handouts); Nasal Irrigation
Background
Thought to be retained or excessive secretions in the upper aerodigestive tract, phlegm presents a unique challenge to both patients and providers. Though its presentation may appear benign, it can become very frustrating for patients when therapy fails. It proves equally challenging for providers who seek to identify the source of these secretions, when their origins may be multifactorial with little evidence of a treatable cause.

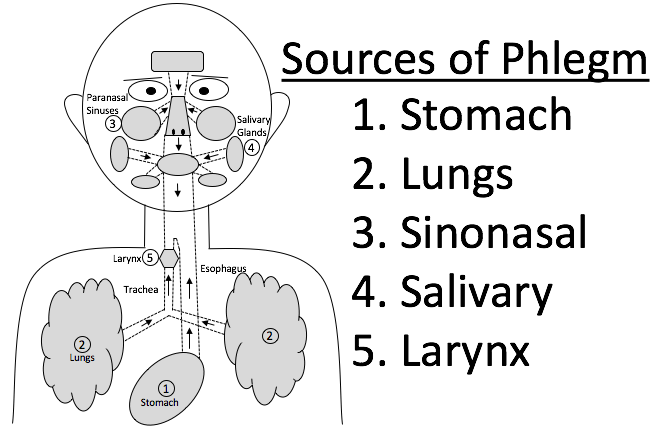
Sources of Phlegm
- Reflux of Gastric Contents
- Laryngopharyngeal Reflux (LPR) or Atypical Gastroesophageal Reflux Disease (GERD)
- Bronchial Glands
- Composed of mucus cells (secreting mucins), serous cells (secreting antibacterials), and water secretions
- Normally <10 mL/d of mucus produced to protect the lower respiratory tract (Hess 2007)
- Pathologic Influences: Asthma, Chronic Bronchitis, Autonomic Nervous System Abnormalities
- Sinonasal Drainage
- Sources of Sinonasal Fluid
- Vascular permeability via postcapillary venules & fenestrated capillaries
- Exocytosis from submucosal gland seromucous cells
- Exocytosis from epithelial goblet & submucocal gland mucous cells
- Infiltrating leukocytes
- Pathologic Influences: Allergic Rhinitis, Chronic Rhinosinusitis (CRS)
- Sources of Sinonasal Fluid
- Salivary Glands
- Major (Parotid, Submandibular, Sublingual) and minor salivary glands (throughout upper aerodigestive tract)
- Average human swallows 1.5 liters of saliva per day.
- Sialorrhea
- Laryngeal Secretions
- Saccule Glands
- Cough Reflex
Etiologic Factors
- Age
- Changes in Fluid Character
- Changes in Swallowing
- As we age, there are some small systematic changes in the oropharyngeal swallow largely related to a slight slowing in the movement of the bolus and triggering of the pharyngeal stage of swallow (Tracy et al 1989)
- There is a small but significant increase in oral transit time and in the delay time between the oral and the pharyngeal stage (Logemann & Larsen 2012)
- Flexibility and reserve in swallow have also been seen as reduced in elderly normal individuals (Logemann et al 2000)
- The frequency of penetration of liquids and pudding into the airway also increases significantly with age over 50 years (Daggett et al 2006)
- Reduced muscle strength, particularly in the tongue, has been found in individuals over age 60 (Nicosia et al 2000)
- Inhaled Irritants
- Cigarette Smoke
- Marijuana Smoke
- Humidity of Inhaled Air
- Medications
- Autoimmune Disease
- Sjogren's Syndrome
- Radiation Exposure
- Infections
- Viral
- Chronic Airway Disease
- Bronchitis, Cystic Fibrosis, Bronchiectasis, Asthma, Emphysema
Management of Phlegm
- Behavioral Techniques for Oropharyngeal Dysphagia (Logemann 1994, McCabe et al 2009)
- Postural changes
- Affect the way in which gravity moves food through the mouth and pharynx or changes the relationship of oropharyngeal structures before, during, and after the swallow (Welch et al 1993)
- 5 Postural Changes (Logemann et al 1994)
- Chin down to the chest
- Head lifted
- Head rotated to the dynamic side of the pharynx
- Head tilted to the better side of the pharynx or oral cavity
- Lying down, either on the side or on the back
- Sensory enhancements
- Swallow maneuvers
- Diet modification
- Postural changes
Globus Pharyngeus Defined (Eckner 2014)
- Definition: persistent sensation of having a lump, obstruction, or too much mucus in the throat without clinical evidence of such
- Location: most commonly felt in front of neck but sensation can move
- Esophageal Motility: does not interfere with eating and drinking
- Pain: patients commonly feel no pain
Etiologies of Globus Pharyngeus (Järvenpää 2018)
- Inflammation
- LPR
- Rhinitis
- Allergies
- Neuralgia
- Esophageal problems
- Thyroid Disease
- Thyroiditis
- Goiter
- Muscle Strain
- Muscle tension dysphonia
- Overuse of voice
- Tightness of muscles from speaking
- Cervical spine osteophytes
- Lingual tonsil hypertrophy
- Medications
- Sprays that relax the throat
- Anticholinergics
- Isolated cases in which tumors or malignancy cause a globus sensation
- Anxiety
Goals in Management of Globus Pharyngeus
- Rule out significant pathology
- Identify etiology of symptoms
- Decide if treatment is necessary
Diagnostic Testing
- Transnasal Esophagoscopy
- Esophageal Disorder
- Mass effect
- Inflammation
- Barium Swallow & High-Resolution Manometry
- Esophageal Sphincter Spasm
- Esophageal Dysmotility
- pH Probe & Impedance Testing
- LPR
- Radiologic Imaging
- Patients at high risk for malignancy
- Feeling of lump vs excess mucus
Treatment of Globus Pharyngeus
- LPR
- Proton Pump Inhibitors
- H2 Receptor Blockers
- Antacids
- Diet
- Rhinitis
- Allergies
- Neuralgia
- Gabapentin
- Proton Pump Inhibitors
- Myogenic
- Voice Therapy
- Psychogenic
- Antidepressants
- Cognitive Behavioral Therapy (CBT)
Management of Idiopathic Globus Pharyngeus
- Reassurance
References
Eckner A., "Globus Presents Diagnostic Challenge for Otolaryngologists", ENT Today, Feb 2014.
Hess DR. Airway clearance: physiology, pharmacology, techniques, and practice. Respir Care. 2007 Oct;52(10):1392-6. PMID: 17894906.
Tracy JF, Logemann JA, Kahrilas PJ, Jacob P, Kobara M, Krugler C. Preliminary observations on the effects of age on oropharyngeal deglutition. Dysphagia. 1989;4(2):90-4. doi: 10.1007/BF02407151. PMID: 2640185.
Logemann JA, Larsen K. Oropharyngeal dysphagia: pathophysiology and diagnosis for the anniversary issue of Diseases of the Esophagus. Dis Esophagus. 2012 May;25(4):299-304. doi: 10.1111/j.1442-2050.2011.01210.x. Epub 2011 May 19. PMID: 21595782.
Logemann JA, Pauloski BR, Rademaker AW, Colangelo LA, Kahrilas PJ, Smith CH. Temporal and biomechanical characteristics of oropharyngeal swallow in younger and older men. J Speech Lang Hear Res. 2000 Oct;43(5):1264-74. doi: 10.1044/jslhr.4305.1264. PMID: 11063246.
Daggett A, Logemann J, Rademaker A, Pauloski B. Laryngeal penetration during deglutition in normal subjects of various ages. Dysphagia. 2006 Oct;21(4):270-4. doi: 10.1007/s00455-006-9051-6. PMID: 17216388.
Nicosia MA, Hind JA, Roecker EB, Carnes M, Doyle J, Dengel GA, Robbins J. Age effects on the temporal evolution of isometric and swallowing pressure. J Gerontol A Biol Sci Med Sci. 2000 Nov;55(11):M634-40. doi: 10.1093/gerona/55.11.m634. PMID: 11078092.
Logemann JA. Rehabilitation of oropharyngeal swallowing disorders. Acta Otorhinolaryngol Belg. 1994;48(2):207-15. PMID: 8209683.
McCabe D, Ashford J, Wheeler-Hegland K, Frymark T, Mullen R, Musson N, Hammond CS, Schooling T. Evidence-based systematic review: Oropharyngeal dysphagia behavioral treatments. Part IV--impact of dysphagia treatment on individuals' postcancer treatments. J Rehabil Res Dev. 2009;46(2):205-14. PMID: 19533534.
Welch MV, Logemann JA, Rademaker AW, Kahrilas PJ. Changes in pharyngeal dimensions effected by chin tuck. Arch Phys Med Rehabil. 1993 Feb;74(2):178-81. PMID: 8431103.
Järvenpää P, Arkkila P, Aaltonen LM. Globus pharyngeus: a review of etiology, diagnostics, and treatment. Eur Arch Otorhinolaryngol. 2018 Aug;275(8):1945-1953. doi: 10.1007/s00405-018-5041-1. Epub 2018 Jun 25. PMID: 29943257.