
return to: Salivary Gland Surgery Protocols
see also: Plunging Ranula Transoral Resection (Sublingual Gland) Aided With Sialendoscopy with Histopathology and Recurrent neck swelling after ranula resection
GENERAL CONSIDERATIONS
- Background:
- Most common intraoral salivary gland mass.
- Ranula is Latin for "little frog" as the mass was first described as looking like the underbelly of a croaking frog.
- Arises from sublingual salivary gland.
- Etiology believed to be secondary to escaped mucus entering a cavity that becomes lined with granulation tissue. This can be due to:
- Incompletely encapsulated sublingual gland
- Extravasation after disruption
- Obstruction of the sublingual duct
- Ruptured acini
- Classification
- Oral ranula: only intraoral swelling
- Plunging ranula: submandibular or submental swelling without intraoral swelling.
- Mixed ranula: intra- and extra-oral swelling
- Indications:
- Ranulas compromising the airway require immediate management through either excision or incision & drainage.
- There are case reports of congenital ranula noted on prenatal ultrasound. Peripartum surgery may be necessary to establish the airway in a neonate.
- Ranulas that interfere with speech causing dysarthria.
- Ranulas that interfere with submandibular gland function and drainage.
- Ranulas that become infected recurrently
- Asymptomatic lesions maybe resected to avoid any of the above.
- Ranulas compromising the airway require immediate management through either excision or incision & drainage.
- Contraindications:
- Comorbid conditions that prevent safe administration of general anesthesia.
- Active infection is a relative contraindication as it would make dissection and complete excision more difficult.
PREOPERATIVE PREPARATIONS
- Evaluation:
- Clinical examination is the most common diagnostic tool. It is usually discovered as a submucosal blue mass in the floor of mouth.
- Plunging ranulas (without significant intraoral swelling) will present has a cervical mass and will hence have a wider differential:
- Branchial cleft cyst
- Lymphatic malformation
- Thyroglossal duct cyst
- Thymic cyst
- Dermoid cyst
- Teratoma
- CT scan or MRI can be useful in imaging the full extent of the lesion and to confirm clinical findings.
- See Ranula Rads
- Consent for Surgery:
- Explain that the surgery could potentially include both intraoral and extraoral approaches to allow for complete excision.
- May identify that an open approach (with neck incision) has been considered standard and often included removal not only of the pseudocyst, but also the submandibular gland and sublingual gland (see Case Example of Plunging Ranula (Transoral Resection))
-
Contemporary thought is that transoral resection of the sublingual gland without a neck incision (potentially still with placement of a neck drain in selected cases) is adequate treatment (ref Lesperance 2013) - examples with sample operative note of:
- Transoral resection of ranula with ductoplasty use of sialendoscopy
- Transoral resection of ranula with use of sialendoscopy
- The surgery may be described as follows, "An incision will be made in the upper neck and the lesion will be dissected out along its capsule toward the floor of mouth. An incision will then be made in the floor of the mouth to remove the remainder of the lesion and its source: the sublingual salivary gland."
- A discussion should be had with the patient regarding the benefits, alternatives, and risks of the procedure. The discussion of risks should include the following:
- Risks of general anesthesia.
- Pain
- Bleeding
- Infection
- Scar
- Facial nerve injury: marginal mandibular branch (weakness at the corner of the mouth)
- Lingual nerve injury: tongue parethesias or pain.
- Hypoglossal nerve injury: impaired tongue movement, speech disturbance.
- Submandibular duct disruption.
- Recurrence of the lesion
- Need for further surgery
- For simple (non-plunging, non-recurrent) ranula an alternative to resection of the sublingual gland (usually requiring a general anesthetic) is an effort at marsupialization with recognition of the high recurrence rate that may lead to more definitive treatment (Schwanke et al 2013). If this approach is taken, the procedure can be done under local anesthesia and patient is pre-medicated with Augmentin PO beginning the day of surgery and continuing for 1 week and Peridex rinse is continued for several weeks post-op.
- Explain that the surgery could potentially include both intraoral and extraoral approaches to allow for complete excision.
NURSING CONSIDERATIONS
- Room Setup
- Microscope if indicated for submandibular duct cannulation
- Instrumentation and Equipment
- Parsons McCabe nerve stimulator
- Medications (specific to nursing)
- 1% Lidocaine with 1:100,000 epinephrine on the field
- Prep and Drape
- Both intraoral (dilute betadine) and extraoral betadine prep.
- Head drape
- Towels to allow visualization past facial midline to allow for nerve monitoring.
- Drains and Dressings
- Penrose vs #10 soft flat Jackson Pratt drain
ANESTHESIA CONSIDERATIONS
- Relaxation:
- Cervical portion: no neuromuscular blockade to allow for facial nerve stimulation and monitoring.
- Intraoral portion: neuromuscular blockade permissible to allow for improved intraoral access.
OPERATIVE PROCEDURE
IMAGES ABOVE SHOW CASE EXAMPLE OF AN APPROACH USED PREVIOUSLY - FOR MORE CONTEMPORARY TX WITHOUT NECK INCISION, SEE:
Case Example of Plunging Ranula (Transoral Resection)
Case Example: Patient referred after transoral appoach followed by submandibular gland resection now with plunging ranula.
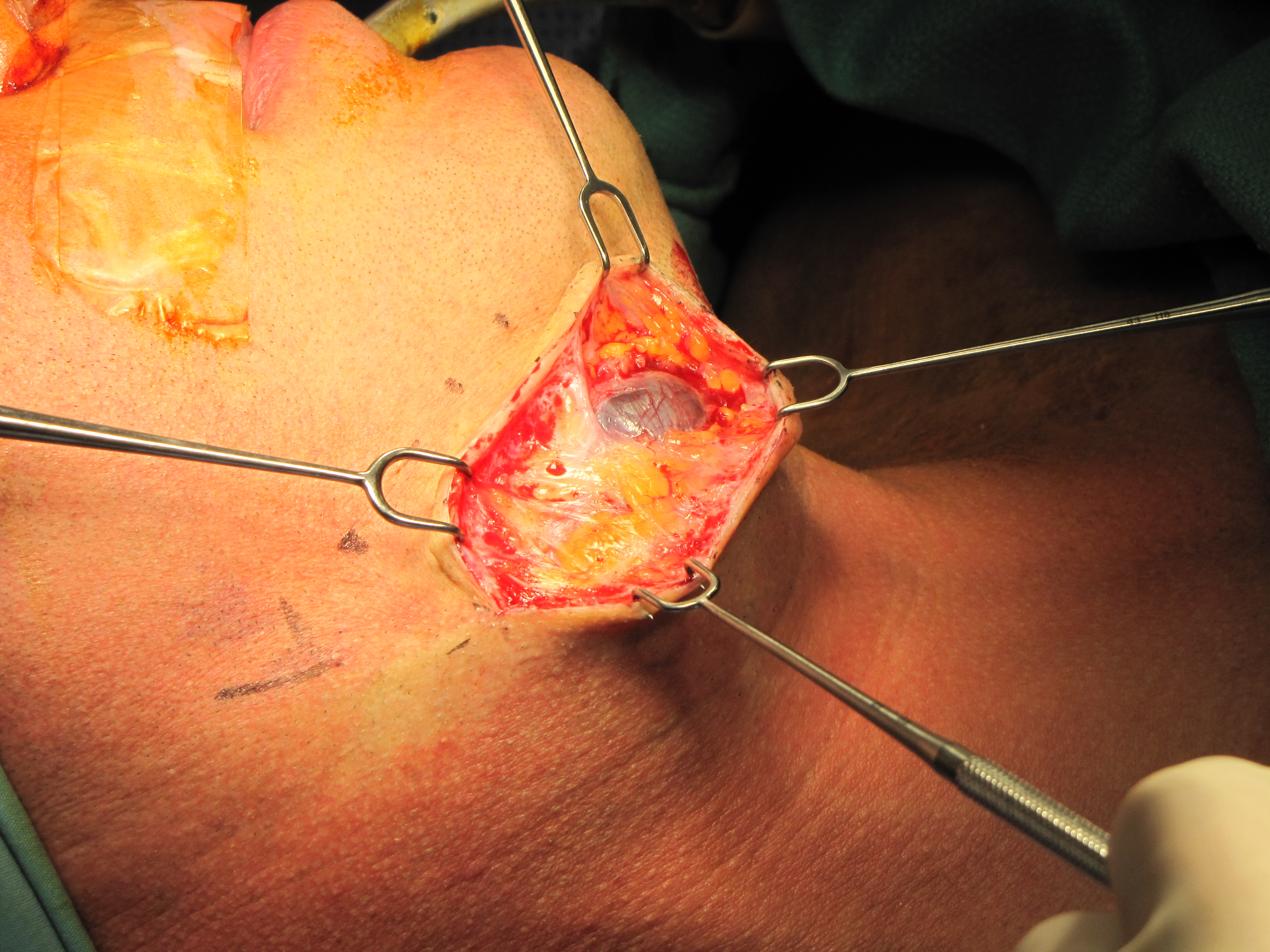
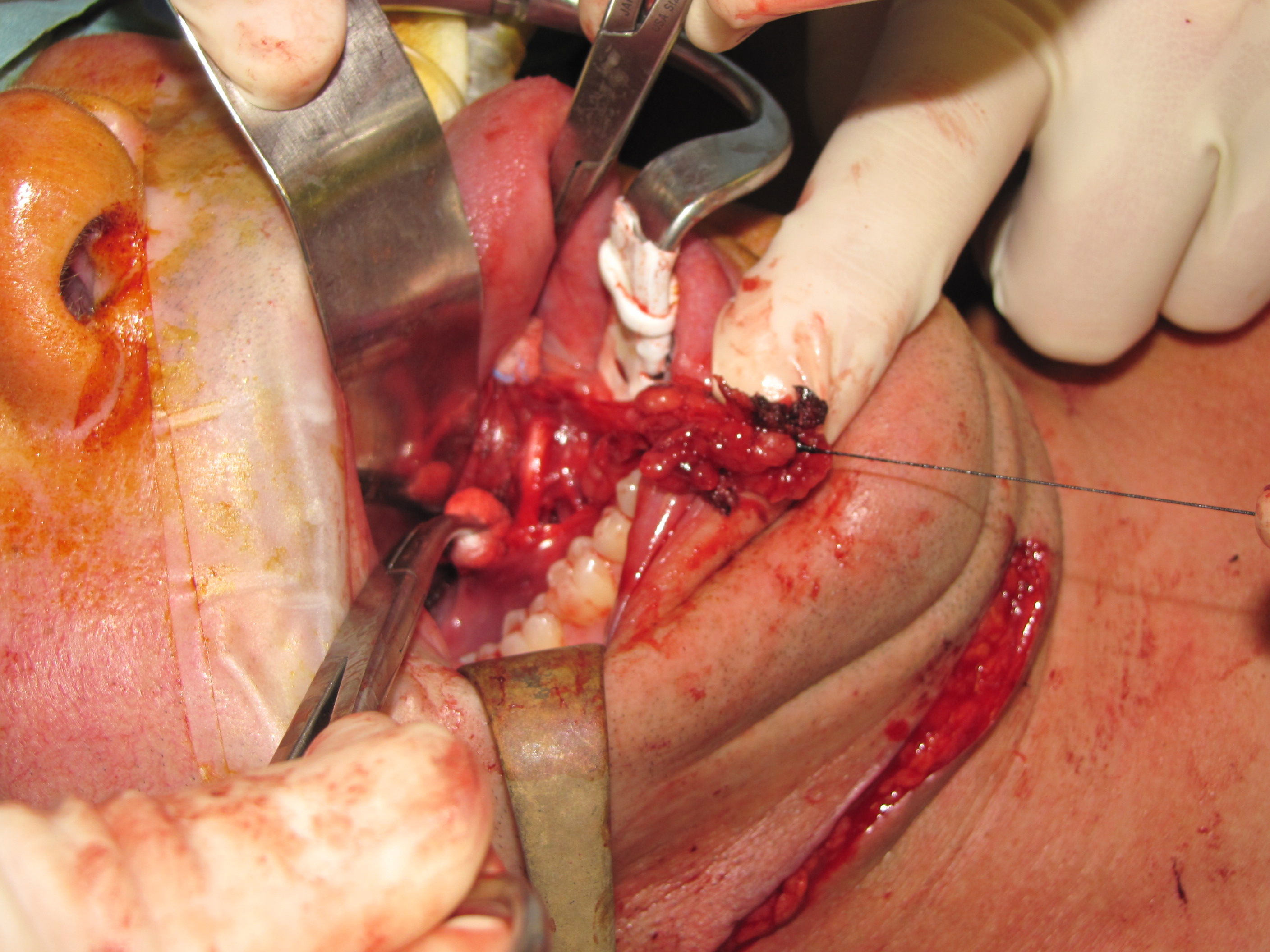
Preparation and incision:
- Neck incision through platysma, use of nerve stimulator to prevent injury to ramus mandibularis.
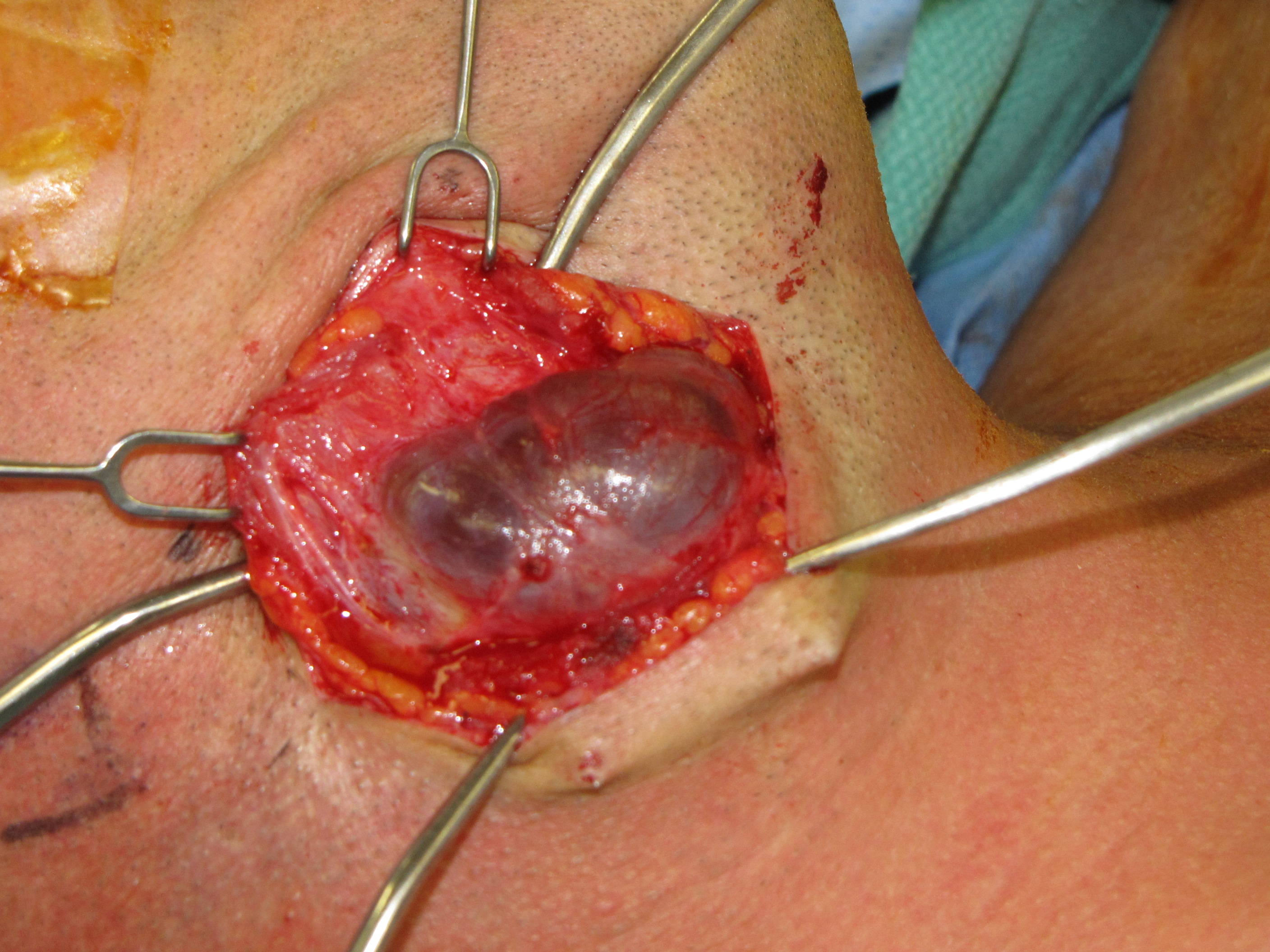
- ## Resection of the pseudocapsule of the plunging ranula (extravasation pseudocyst) is performed - but of questionable value (see Patel et al 2009) in that the key is to remove the sublingual gland(s) responsible for the salivary production
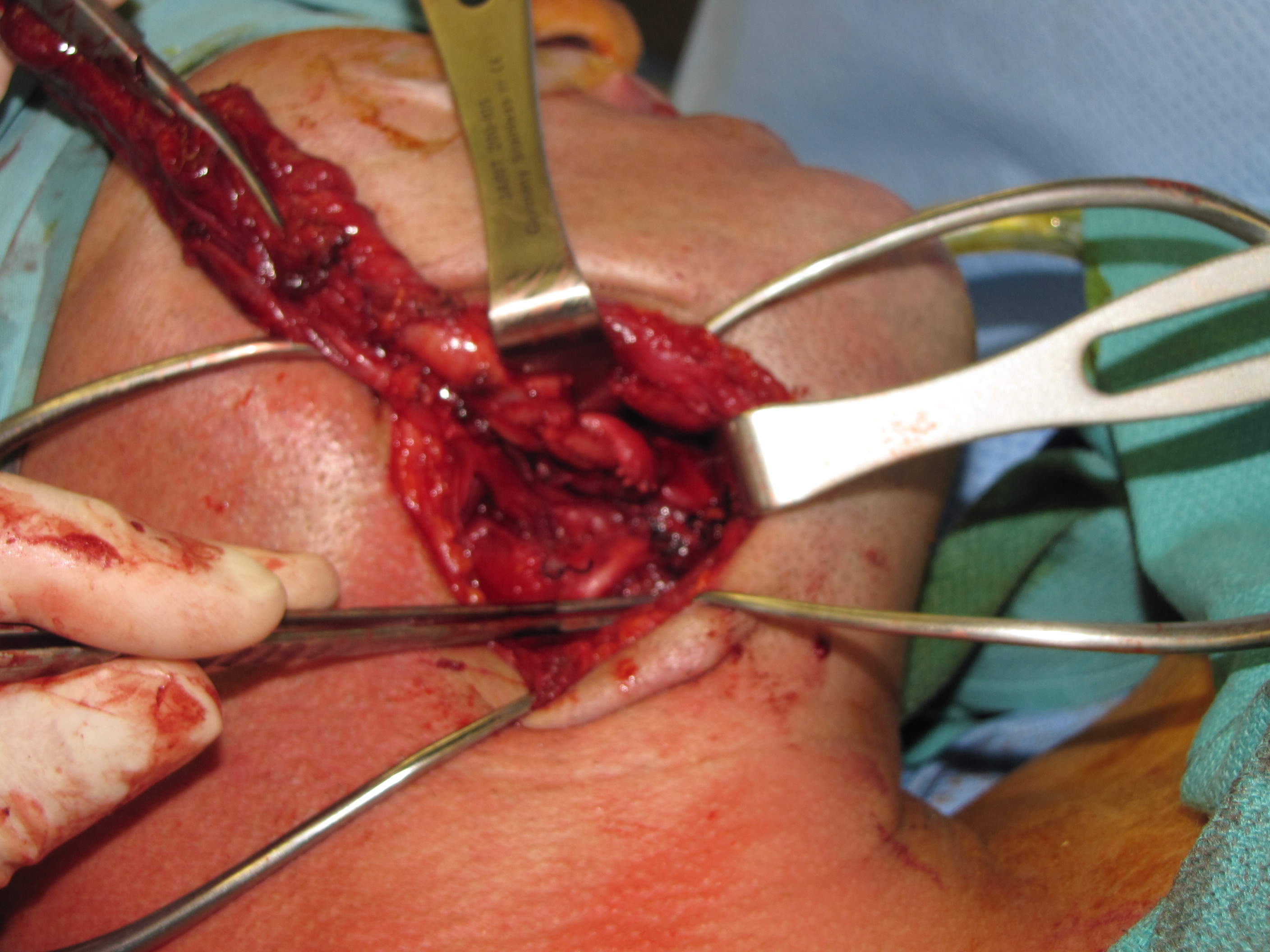
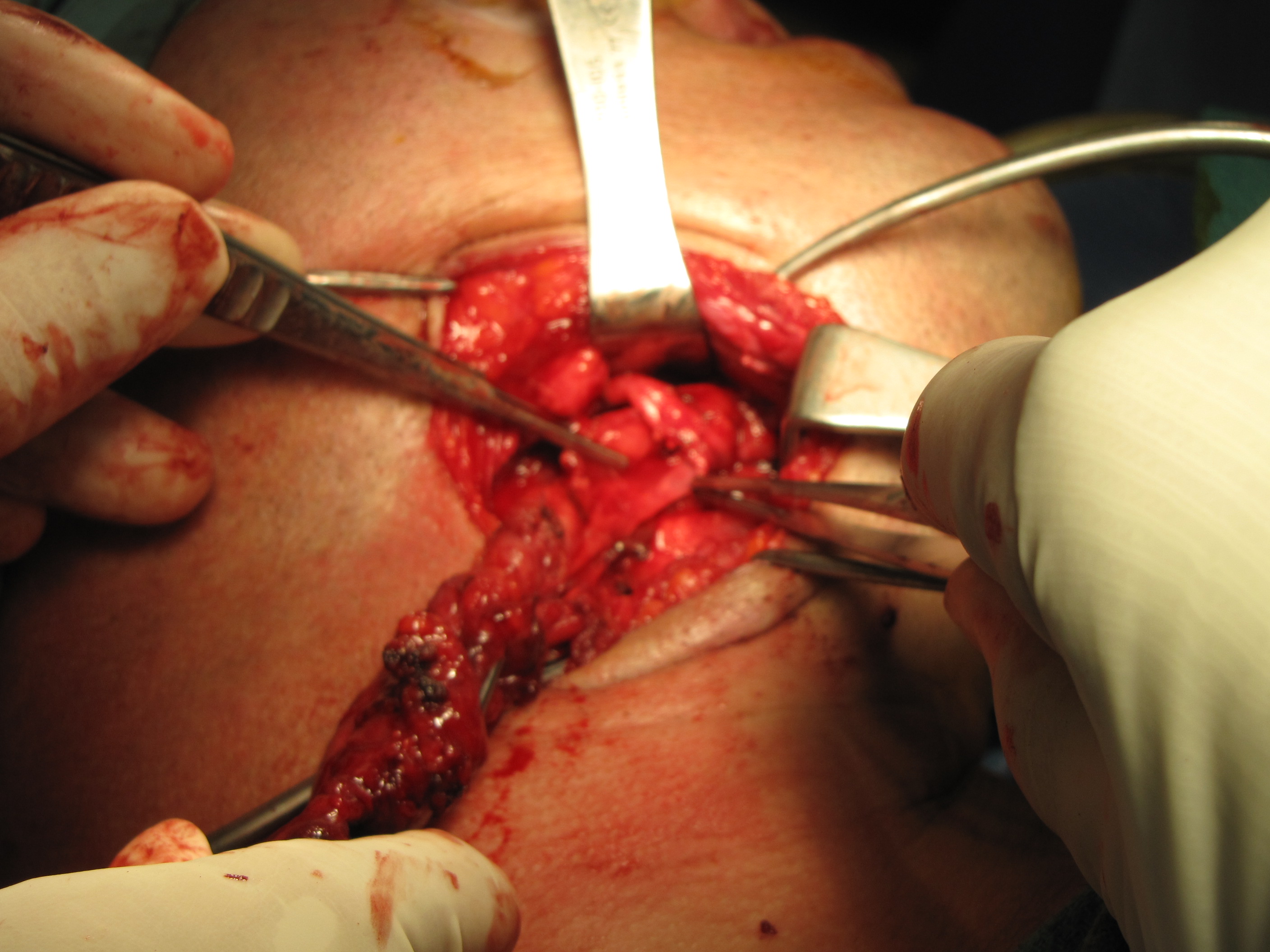
- Dissection permits preservation and exposure of the lingual nerve (and hypoglossal nerve)
- The end of the plunging ranula as it extends under the lingual nerve is ligated with 2-0 silk. After transection below the ligature, the silk suture with attached sublingual gland will be manipulated intra-orally in the process of the transoral floor of mouth resection to ensure complete removal of the sublingual gland.
- Incision sparing mucosa for later water-tight closure exposes the sublingual gland and lingual nerve.
- The sublingual gland is dissected free of the lingual nerve and removed.
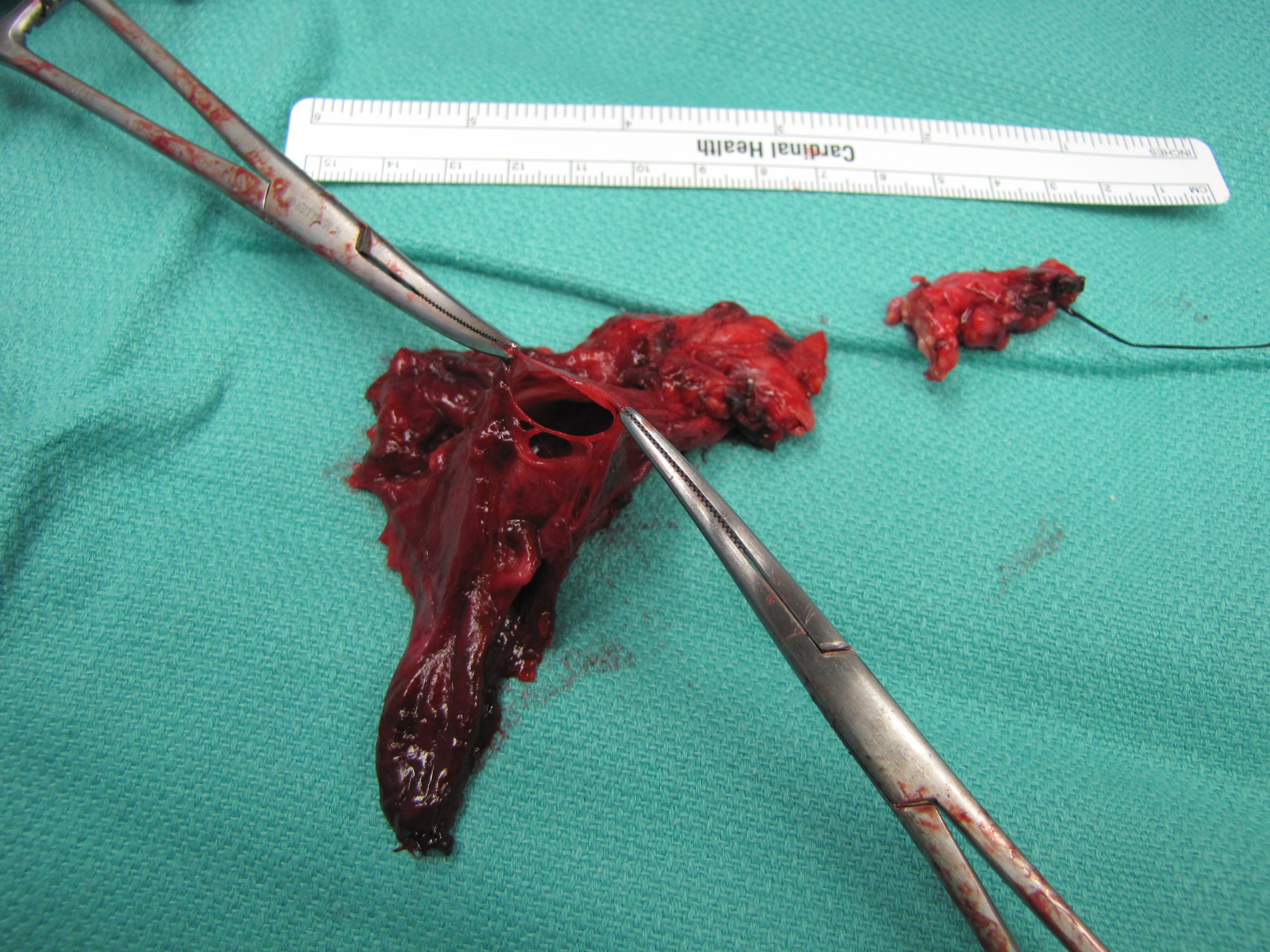
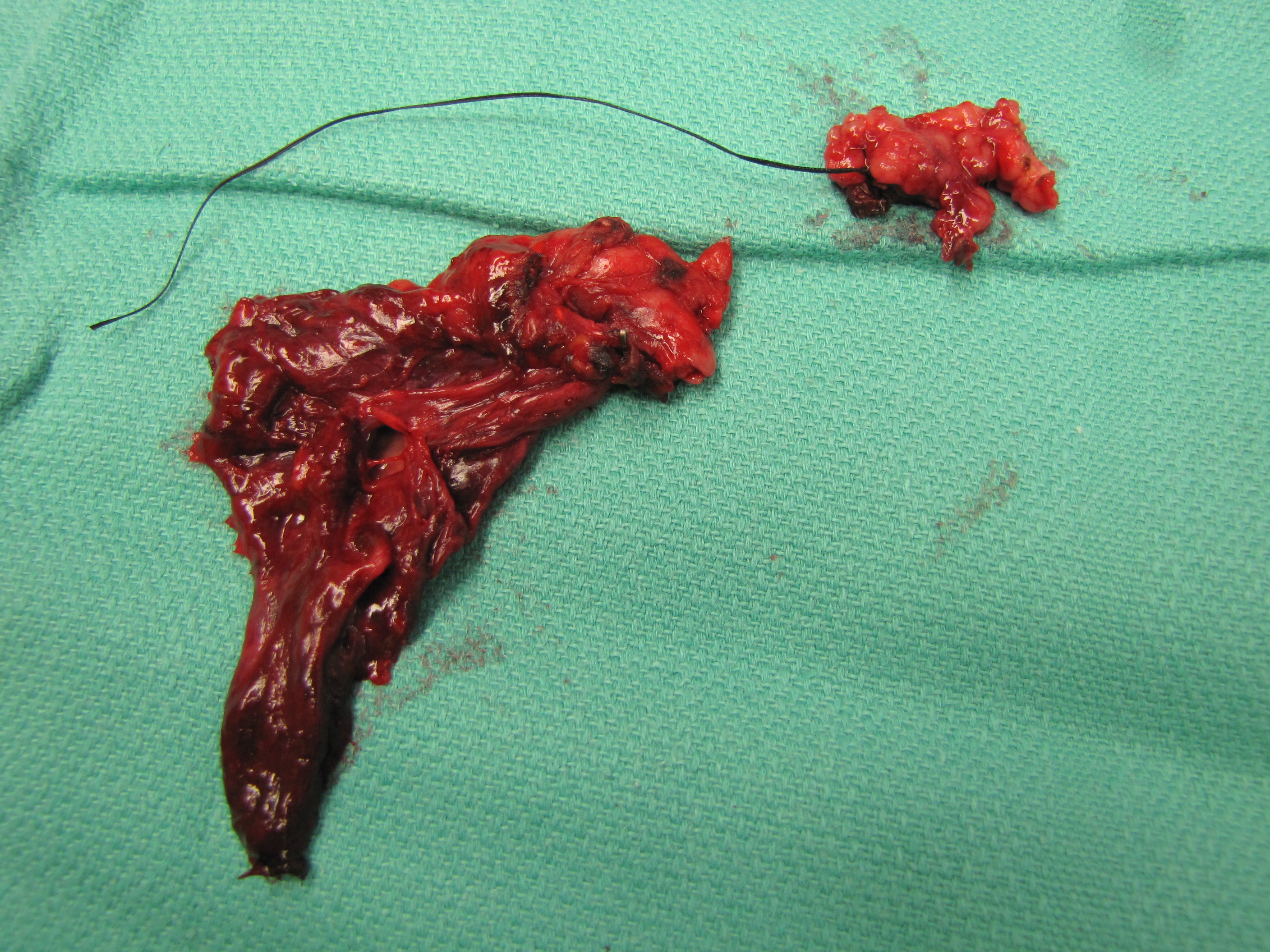
- The sublingual glands and plunging ranula after removal. Note suture on sublingual gland (had been placed through the neck under the lingual nerve).
- Specimen opened.
POSTOPERATIVE CARE
- Inpatient admission for acute post-operative care
- Strict intake and output to determine when drains can be safely removed.
- Iowa criteria is less than 30cc total over three 8 hour shifts in closed suction drains.
- Chlorhexadine rinse 15cc TID to keep floor of mouth incision clean.
- 48 hours of post-operative broad spectrum antibiotic coverage.
- Strict intake and output to determine when drains can be safely removed.
- Discharge Instructions:
- No heavy lifting (over 15lbs) for two weeks
- Antibacterial ointment to incision BID
- No soaking wound
REFERENCES
Patel MR, Deal AM, Shockley WW: Oral and plunging ranulas: What is the most effective treatment? Laryngoscope. 2009 Aug;119(8):1501-9.
Lesperance MM: When Do Ranulas Rquire a Cervical Approach? Laryngoscope 2013 Aug; 123 pp 1826-1827
Schwanke TW, Oomen KP, April MM, Ward RF, and Modi VK: Floor of mouth masses in children: proposal of a new algorithm. int J Pediatr. Otorhinolaryngol 2013 Sep;77(9):1489094
Bowers EMR, Schaitkin B. Management of Mucoceles, Sialoceles, and Ranulas. Otolaryngol Clin North Am. 2021 Jun;54(3):543-551. doi: 10.1016/j.otc.2021.03.002. PMID: 34024482.
Ogle OE. Excision of Sublingual Gland. Oral Maxillofac Surg Clin North Am. 2021 May;33(2):161-168. doi: 10.1016/j.coms.2020.12.001. Epub 2021 Jan 29. PMID: 33526317.