return to: Bilateral Vocal Cord Paralysis or Tracheostomy and Upper Airway Management Symposium July 30 2016 IAO and SOHN Iowa City Iowa
Case Example
2001 - underwent total thyroidectomy with bilateral vocal cord paralysis
2004 - underwent left posterior cordotomy at another institution to improve airway
2010 (May) - seen at the U of Iowa for progressive shortness of breath G2R2B1A1S1:
2010 (June) - treated at UIHC with tracheotomy and left posterior laser cordotomy
2010 (July) - tracheotomy removed one month after surgery; subsequent sleep study showed no obstructive apnea
2011 (March) - followup (9 months) in clinic improved airway but worse voice G3R1B2A3S3:

2012 (March) - followup (21 months) evaluation in clinic:
"in Voice Clinic today, a severe degree of dysphonia is a G3R1B2A3S3 is identified but correlates with an excellent result from the cordotomy with a good airway, permitting the her to stride vigorously down the hallway and back with me with no shortness of breath. She relates she can navigate a flight of stairs also in a similar fashion"

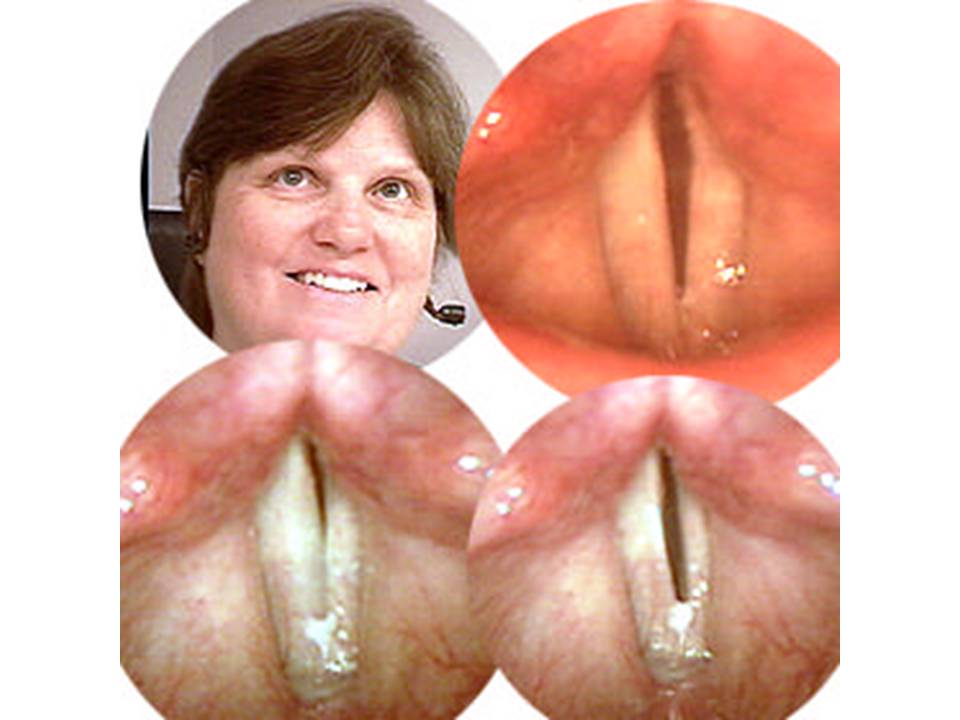
Video: preop (May 2010 evaluation followed by intraoperative process followed by 2012 March evaluation)
see video:
Modified Operative Note
Findings: Bilateral vocal cord paralysis, cords in adducted position, mobile arytenoids bilaterally, slight defect in the left vocal cord immediately anterior to vocal process
Tracheotomy performed, #4 Shiley placed Left posterior cordotomy performed with CO2 laser on 8 Watts continuous super-pulse.
Indications:... with bilateral vocal cord paralysis after TT 10 years ago. S/p left posterior cordotomy 5 years ago. Now with difficulty breathing, progressive stridor and dyspnea.
Procedure:
MicroDL with palpation of arytenoids and photography
Tracheotomy #4 Shiley
MicroDL with posterior left cordotomy
Procedure Details: Risks, benefits, indications, alternatives and procedure were explained to the patient. All questions were answered. Informed consent was reviewed and a timeout performed.
General anesthesia was induced with mask ventilation with the patient supine. A microdirect laryngoscopy was performed after dental protection placed and the larynx exposed. The cords were sprayed with 2 cc of 4% lidocaine. A 5.0 MLT tube was placed and the cuff inflated. The arytenoids were then palpated and found to be mobile bilaterally. The Lindholm scope was then placed and put into suspension, and the airway, glottis, and subglottis were visualized and photo documented. The cords were noted to be in adducted position. The patient was taken out of suspension and the Lindholm removed. Attention was directed to the neck. The neck was injected with 1% lidocaine with 1:100,000 epinephrine. At the site of planned tracheostomy, a vertical incision was planned. The patient was prepped and draped in the usual sterile fashion. A vertical incision was made with a #15 blade and carried down through the median raphe with blunt dissection and cautery. The trachea was identified. There was no thyroid, consistent with her previous total thyroidectomy. An inferior based Bjork flap was created after Anesthesia advanced the tube down to the right main stem. The tube was repositioned, as the cuff had not been damaged, and careful hemostasis was achieved. The Bjork flap was sutured to the inferior skin with three 3-0 Vicryl sutures. A 4.0 Shiley with cuff was placed and the cuff was inflated. A trach strap was placed and the trach was secured in placed. Attention was placed back to the oropharynx and glottis and the Lindholm was reinserted and the patient was placed in suspension. Moist towels were placed around the scope and careful note was made to ensure that no plastic tape was on the patient. The eyes were covered with cloth tape with saline-soaked pads. The vocal cords were identified and spreaders were used to open the adducted cords. The trach was noted to be placed just below the first tracheal ring with packing placed above the flange (moist neurosurgical cottonoids). The cords were again examined and the arytenoids palpated and found to be mobile. The left cord was examined and the area just anterior to the left vocal process was noted. A CO2 laser on 8 watts continuous super-pulse was used to perform a posterior cordotomy on the left side, just anterior to the vocal process with the lateral margin deemed the perichondrium immediately overlying the thyroid cartilage. Hemostasis was achieved with the laser and no cartilage was exposed. Photo documentation was taken throughout the case and after the cordotomy there was noted to be an improved patent airway. The patient tolerated the procedure well. Additional lidocaine was sprayed onto the cords and the char was wiped off with saline-soaked pledgets. The patient was turned back over to Anesthesia and awoke without difficulty. The patient tolerated the procedure well.