See also: Laryngotracheal Reconstruction with Costal Cartilage Grafting; The Evaluation of Stridor in Pediatric Patients
See video:
Indications
- For symptomatic grade 1, 2 and some grade 3 sublgottic stenosis
- Two or fewer laryngotracheal units involved
- Good pulse oximetry
- No recent oxygen or ventilator requirement
Contraindications
- Ventilator-dependence
- Poor pulmonary status
- Poor overall condition
- Anesthesia related contraindications
- Severe reflux (relative contraindication)
**No minimum age or weight requirements for laryngotracheal reconstruction
Preoperative Preparation
Evaluation
- Complete history and physical examination
- Flexible fiberoptic laryngoscopy
- Diagnostic laryngoscopy, bronchoscopy
Consent
- Description of procedure
- Explain possible complications
- Bleeding
- Complications related to general anesthesia
- Graft dislodgment
- Need for tracheotomy
- Hypoxic injury
- Pneumothorax/pneumomediastinum from graft harvest
- Loss of airway / ventilation issues
- Inadvertent separation of trachea with retraction of distal trachea into chest
- ETT obstruction
- Accidental extubation
- Glottic edema
- Wound dehiscence / infection
- Airway obstruction post-extubation
- Death
Medications
- 0.5% Lidocaine with 1:100,000 Epinephrine
Positioning
- Supine position with shoulder roll, donut jelly, and eye protection
- Turn table 90° for DL and B
- Turn bed back towards anesthesia side for ssLTR with anterior costal cartilage graft
Prep and Drape
- Insert foley catheter
- Prep from the lip to the naval
- Drape to separate the chest and neck incisions
- Please see video for details
Drains and Dressings
- Quarter inch Penrose drains x 2
- 4x4 gauze pack
- Medium size Tegaderm transparent dressing x 2
- Dermabond skin glue
Anesthesia Considerations
- Well communication and coordination with the anesthesia team
- General anesthesia for induction and bag mask ventilation to maintain spontaneous respiration
- Direct laryngoscopy and bronchoscopy to reassess the grade, location, and length of airway stenosis
- Size the airway using cuffless pediatric ETT to age appropriate expected ETT. Assess air leak. If leak present with <10cm H20, upsize tube. If between 10-25 cmH20, compare to expected ETT. If >25 cmH20, downsize tube.
- Balloon dilation according to grade of stenosis (e.g. 5, 7 dilators)
- Nasal endotracheal intubation
Procedure
Costal cartilage graft harvest
- A skin marker to plan a 4.5cm incision 1.5cm below the right nipple
- 0.5% Lidocaine mixed with 1:100,000 Epinephrine is injected to the incision site
- Aim to harvest the right 5th costal cartilage
- A 15 blade to make a 4.5 cm right chest incision through subcutaneous tissue
- Monopolar cautery to dissect through pectoralis major and serratus anterior and reveal the cartilaginous portion of the right rib
- Bipolar cautery to remove the attachments of the external intercostals inferior and superior to the cartilaginous portion of the rib
- A 15 blade to sharply dissect pericondrium superiorly and inferiorly
- A cottlle's elevator and freer elevator to dissect the plane between perichondrium and rib to connect the inferior and superior incisions, leaving the deep layer of pericondrium down
- Laterally, the blue line, separating cartilage from bone, is identified. A 22-gauge needle is used to identify the bony cartilaginous junction
- The flat portion of a Senn retractor is placed in the pocket beneath the rib to protect the pleura and a 15 blade is used to cut down through cartilage completely
- The rib is dissected free from the perichondrium underneath under direct visualization
- The flat portion of a Senn retractor is then placed deep to the rib medially and a 15 blade is used to complete the removal of the rib cartilage
- The rib cartilage is placed in saline
- Irrigation of the surgical bed to check for leak at 35 mmHg
- Deep muscle and fascia are approximated with running and interrupted 3-0 vicryl sutures
- A quarter inch penrose drain is placed deep to this and secured to skin using 2-0 Proline
- Skin closure using 4-0 monocryl is running subcuticular fashion
- The skin is sealed with dermabond
- Gauze covered in tegaderm is used to dress the wound
Single Stage Laryngotracheal Reconstruction
- A skin marker to plan a 5.5cm incision in the neck midway between the thyroid cartilage and suprasternal notch at midline
- 0.5% Lidocaine mixed with 1:100,000 Epinephrine is injected to the incision site
- A 15 blade to make the incision through skin and platysma
- Monopolar cautery to raise upper and lower subplatysmal flaps
- The midline raphe of the strap muscles is divided and retracted laterally
- Hyoid, thyroid and cricoid cartilage landmarks are palpated
- The thyroid gland is divided with bipolar cautery
- Kittners to remove fascia and soft tissue from the larynx
- 3-0 Proline sutures to be placed through the cricoid and trachea bilaterally as retraction suture. Care taken not to puncture the ETT cuff
- A straight beaver blade to make a ~1.5cm incision through the very caudal portion of thyroid cartilage down through the cricoid, down to the first and second tracheal rings
- A caliber to measure the dimensions required to expand the airway with the anterior right rib graft (length, distraction and thickness)
- The rib cartilage graft is crafted in a boat shape in a sterile setup
- The required dimension are crafted with flanges to fit easily and to prevent dislodgement
- Perichondrium is preserved to line the airway
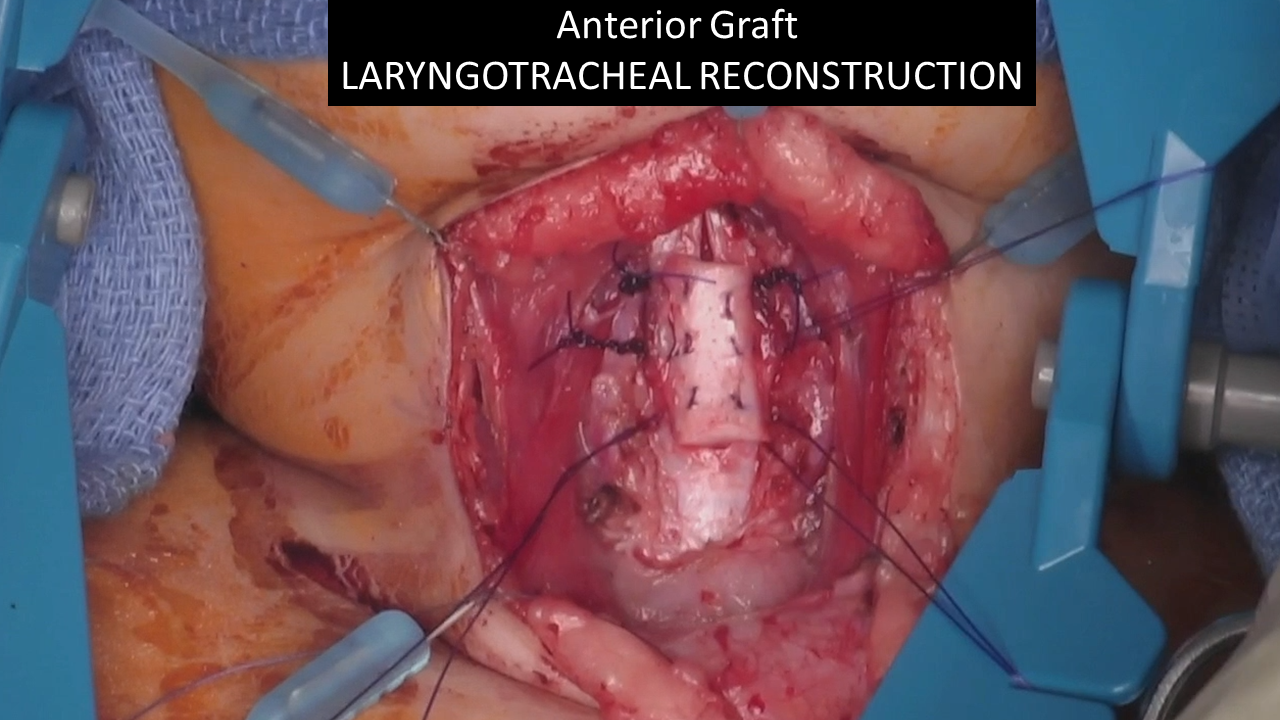
- The anterior graft is then positioned to the anterior open defect such that perichondrium lines the expanded airway
- 3-0 PDS mattress sutures are placed in a stepwise fashion through the graft at a 90 degree angle of the graft and through the intercartilaginous trachea. 3 of these are placed on either side and the graft is parachuted in place
- An interrupted PDS suture is placed superior to the graft
- Tiseel is used to cover the graft
- Air leak is checked with valsalva
- The thyroid lobes are approximated using interrupted 3-0 Vicryl
- Strap musculature are re-approximated in a similar fashion and deep dermal Vicryl sutures are placed
- A quarter inch penrose is placed for drainage
- 4-0 Monocryl is used for running subcuticular closure
- This skin closure is coated with dermabond
- Gauze covered in tegaderm is used to dress the wound
- The ETT cuff is deflated and should remain deflated till extubation
- ETT is taped securely in place while taking care to avoid alar pressure that may cause necrosis. It is confirmed in position by flexible bronchoscopy and intraoperative CXR
- A size appropriate nasogastric tube is placed and secured. This is confirmed in place by direct visualization and CXR
Postoperative Care and Instructions
- Transfer to neonatal/pediatric intensive care unit
- Airway cart, bronchoscopy tower, flexible fiberoptic bronchoscope, similar and smaller size ETT at bedside in case of accidental extubation requiring emergent reintubation
- Prominent sign to call pediatric otolaryngology for any airway concerns
- Keep nasally intubated and sedated and provide NICU/PICU with sedation protocol
- Watch for nasal alar redness/necrosis
- Keep ETT cuff deflated till time of extubation
- Paralysis for 2 days then wean per protocol
- Nutrition consults and NG feeds
- Intravenous broad-spectrum antibiotic: Zosyn for 10 days
- Omeprazole for 3 months
- Avoid steroids until planned extubation
- Neck and chest Penrose drains to be removed on POD1
- Repeat DL and B in 4-5 days to examine the airway, downsize to an uncuffed ETT with planned extubation the following day
LTR sedation protocol
- All patients managed in the neonatal or pediatric ICU postoperatively
- State behavioral scale to monitor depth of sedation
- Morphine and Dexmedetomidine infusions through central venous lines to maintain SBS goal -2 (responsive to noxious stimuli) to -3 (unresponsive) as prescribed by the ICU team
- If needed, opioid boluses given q 2 to 4 hours as prescribed by the ICU team
- NM blockade initiated with vecuronium and titrated to maintain a train-of-four of one
- Train-of-four monitoring by trained nursing staff as per PICU standard of practice
- Daily NM blockade “holidays” as decided by PICU and ENT teams
- Avoid Corticosteroids due to association with myopathy when used in conjunction with Aminosteroid paralytic agents and delays in healing
- Enteric nutrition (TP) initiated on postoperative day 1 to optimize nutrition
- Prior to extubation, Dexamethasone (0.25–0.5 mg/kg IV q6h 2–4 doses) empirically for all patients starting 8 hours prior to planned extubation. Patients should not otherwise receive steroids during their hospitalization
- Neuromuscular blockade discontinued 4 to 6 hours prior to extubation
- Propofol initiated and titrated to goal SBS -2 as paralysis is lifted
- Dexmedetomidine continued at its prior rate, unless bradycardia limited coadministration with Propofol
- Propofol is discontinued in all patients and washout is ensured prior to extubation. Patients frequently remain on Dexmedetomidine through extubation
- Opioid infusions discontinued entirely for the 1 to 2 hours immediately surrounding extubation and restarted at 25% to 50% of prior dose only if needed for withdrawal symptoms
Extubation criteria
- Awake
- Breathing tidal volumes >5 to 7 ml/kg on pressure support of 6-10 cm H2O
- Positive end-expiratory pressure of 5 cm H2O with FiO2 of 40% or lower, without tachypnea or respiratory distress
Post extubation
- Dexmedetomidine infusion maintained as Morphine stopped or tapered
- Opioid and Dexmedetomidine taper as per PICU pharmacy protocol
- Nebulized Ciprodex should be started
- PO diet initiated and advanced as tolerated
References
Cable BB, Manaligod JM, Bauman NM, Smith RJ. Pediatric airway reconstruction: principles, decision-making, and outcomes at the University of Iowa hospitals and clinics. Ann Otol Rhinol Laryngol. 2004 Apr;113(4):289-93. doi: 10.1177/000348940411300406. PMID: 15112971.
Fauman KR, Durgham R, Duran CI, Vecchiotti MA, Scott AR. Sedation after airway reconstruction in children: A protocol to reduce withdrawal and length of stay. Laryngoscope. 2015 Sep;125(9):2216-9. doi: 10.1002/lary.25176. Epub 2015 Jul 7. PMID: 26152806.