

click on image above to enlarge and advance with cursor over border
return to: Sialendoscopy; Sialogram Technique; Anatomy of submandibular gland and duct
see also: Salivary Stone Removal with Ductoplasty from Submandibular Gland
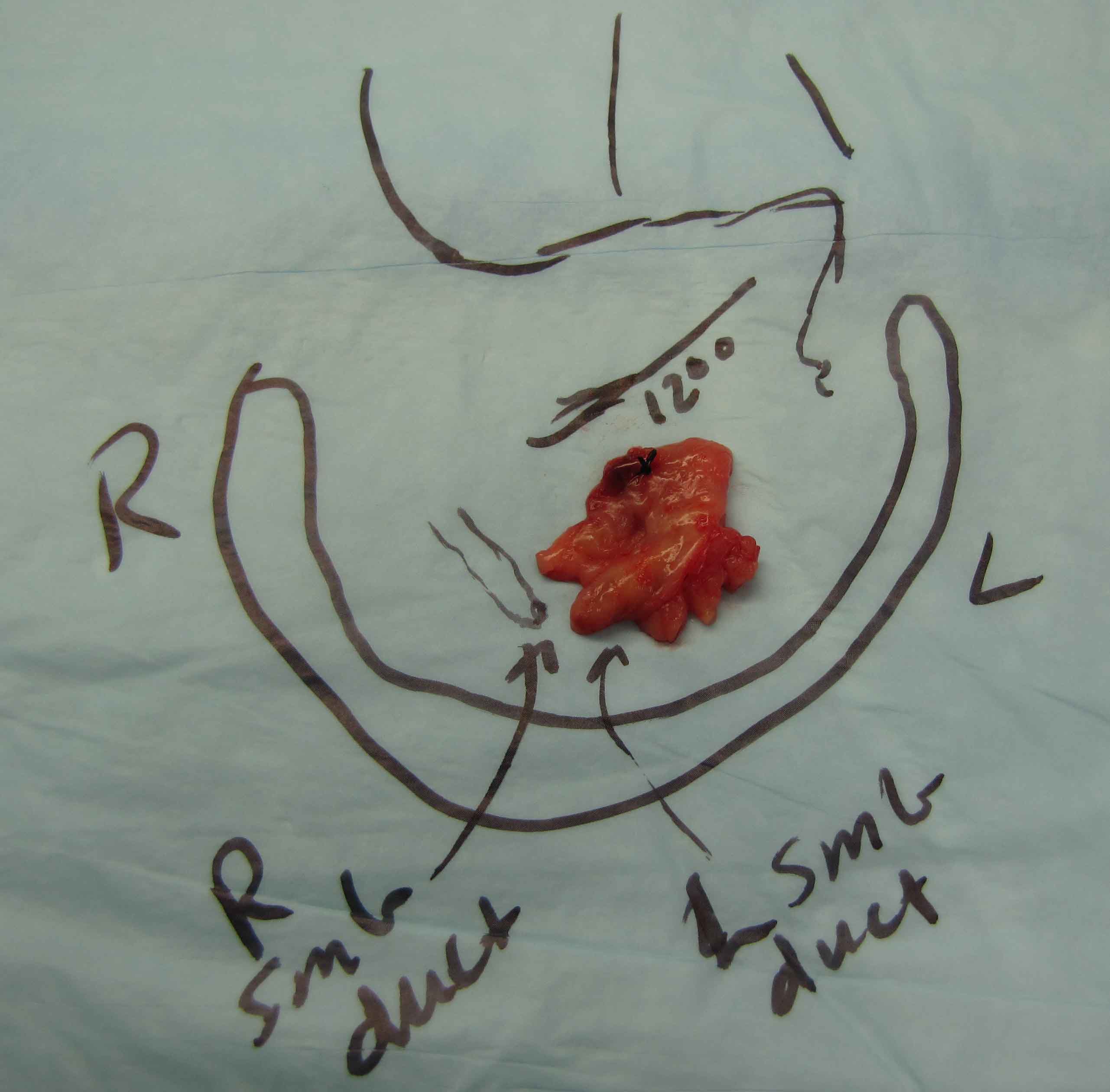
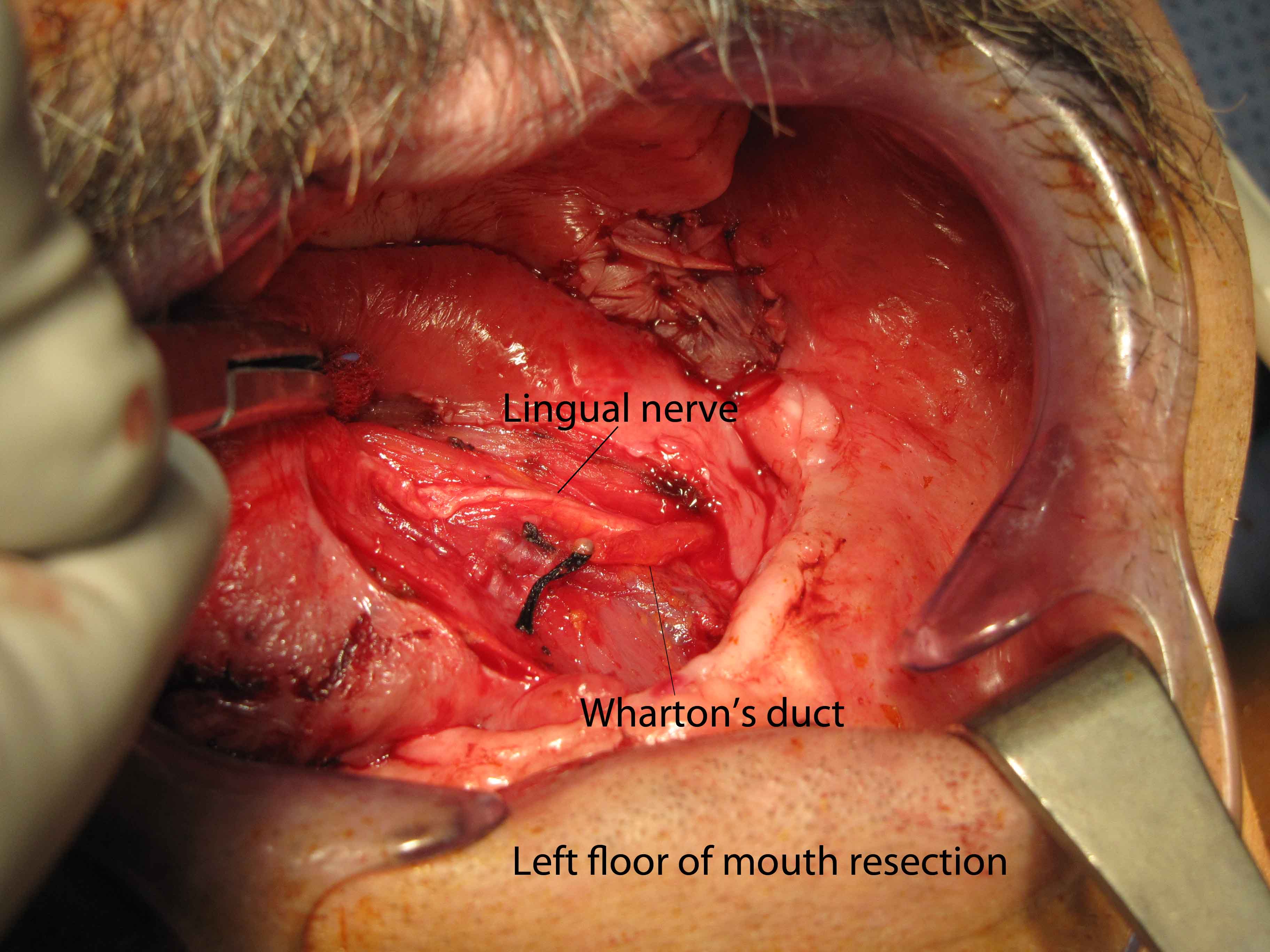
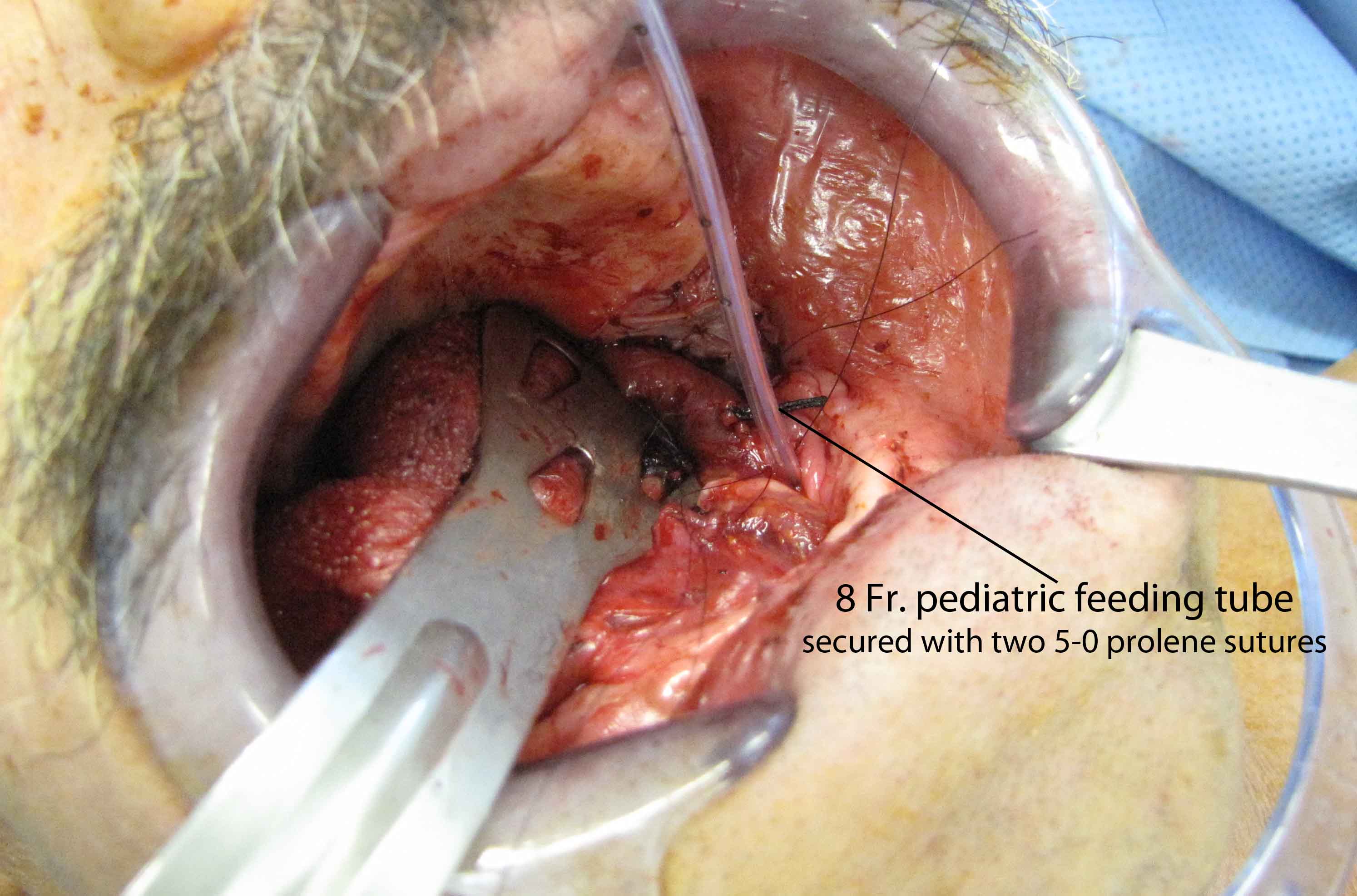
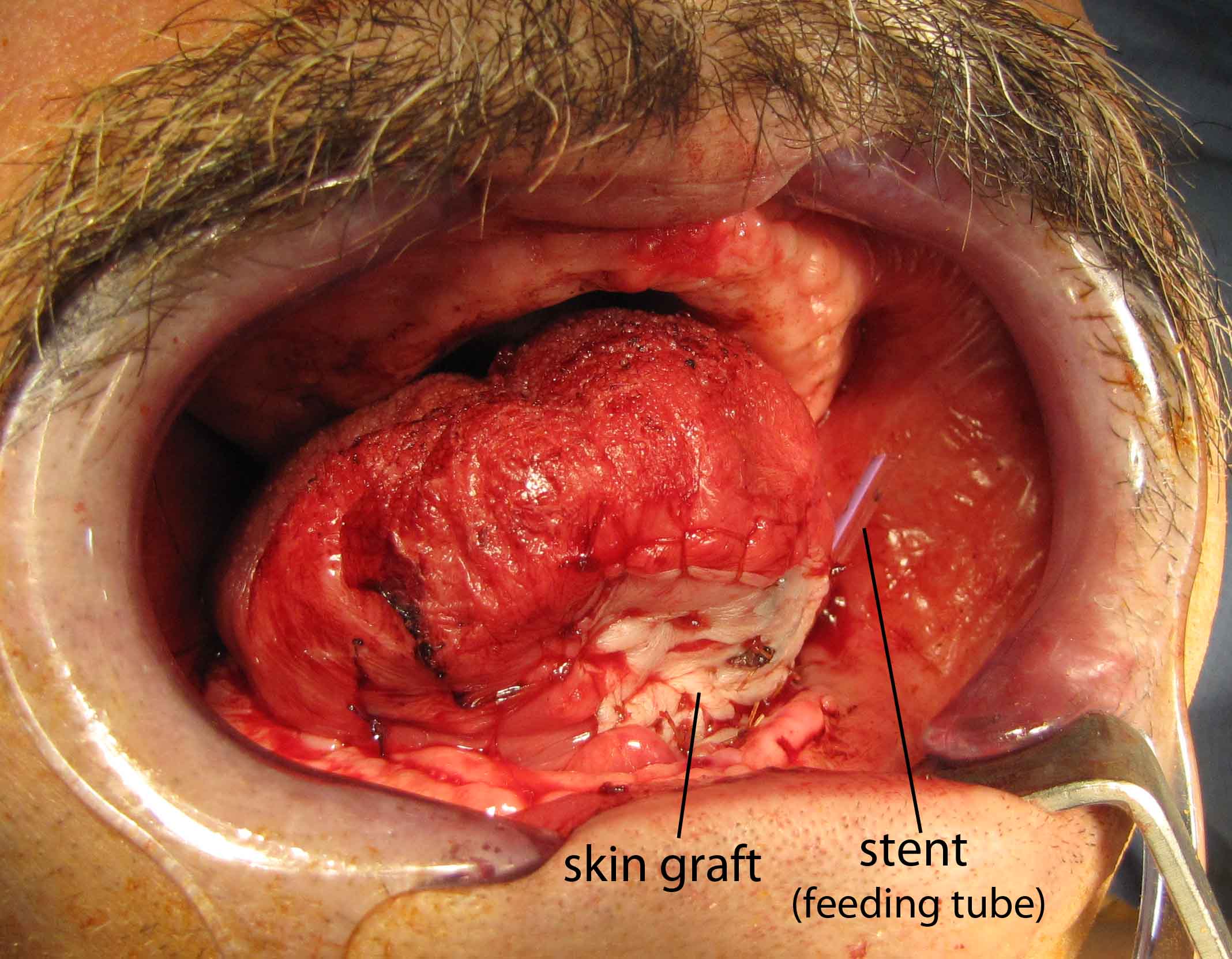
Left Wharton's ductoplasty after superficial cancer resection left floor of mouth
See video:
Salivary Stones
- Epidemiology (Bailey)
- 80% of salivary stones occur in the Submandibular Gland (SMG)
- 90% of SMG stones are radiopaque; 90% of parotid gland stones are radiolucent
- Risks (Bailey)
- Nidus of material allowing precipitation of salts coupled with salivary stasis
- SMG has more alkaline saliva and higher concentrations of calcium and phosphate
- Gout is the only systemic disease known to cause salivary gland calculi (Uric acid stones)
- Indications
- Palpable or hilar stone seen on CT or Ultrasound
- Recurrent obstructive symptoms
- Contraindications
- Poor mouth opening
- Stone removal; Efforts should be made to save glands that are obstructed by stones
- Functional recovery of glands following surgery tested by scintigraphic studies indicate return of function (Makdissi J 2004)
- Large stones (>10 mm) located proximally in the hilum have successfully been removed through transoral approach (Zhang 2010)
OPERATIVE PROCEDURE
- Two techniques for intraoral removal of stones
- Duct incision from papilla to stone with marsupialisation (Zenk 2004)
- Inject floor of mouth with Lidocaine with epinephrine
- Duct and overlying mucosa incised from papilla to stone.
- Identify lingual nerve as needed
- Creation of neo-ostium: suture duct to the oral epithelium using 4-0 vicryl
- No stents placed
- 231 patients (115 with distal stones; 102 with hilum stones; 14 with more than 1 stone)
- Neo-ostium stenosis in 5 patients (2% rate)
- Preservation of duct with ductal incision over the stone with closure of duct (McGurk 2004)
- Oblique incision from punctum of SMG along FOM towards 3rd molar tooth leaving a cuff 1.5 cm wide of normal lingual mucosa to facilitate closure
- Dissection down to duct and stone
- Identify lingual nerve
- palpate stone; incise duct over stone
- Closure of duct with 6-0 vicryl
- No stents placed
- 54 patients
- Stricture formation: 3/55 patients (5% rate)
- Duct incision from papilla to stone with marsupialisation (Zenk 2004)
- Sialodochoplasty of SMG duct (Rontal 1987)
- 27 patients treated
- Probe duct with lacrimal probe
- Sharply open the duct posteriorly
- For each 1 cm opened, suture with 5-0 chromic the duct to the oral mucosa ("suture as you go")
- This is performed back until the stone is encountered
- No stent placed
- Patient treated with 10 days of antibiotics
- Only 1 patient had restenosis b/c the posterior portion of the duct was not completely sutured
REFERENCES
McGurk M, Makdissi J, Brown JE. Intra-oral removal of stones from the hilum of the submandibular glan: report of technique and morbidity. Int J Oral Maxillofac Surg 2004; 33:683-6
Zenk J, Constantinidis J, Al-Kadah B, Iro H. Transoral removal of submandibular stone. Arch Otolaryngol Head Neck Surg 2001; 127: 432-6
Rontal, M, Rontal E, The use of Sialodochoplasty in the treatment of benign inflammatory obstructive submandibular gland disease. Laryngoscope 1987; 97: 1417-21
Zhang Lei et al. Long-term outcome after intraoral removal of large submandibular gland calculi. Laryngoscope; 120: 964-6
Makdissi J, Escudier MP, Brown JE, Osailan S, Drage N, McGurk M. Glandular function after intraoral removal of salivary calculi from teh hilum of the submandibular gland. Br J Oral Maxillofac Surg 2004: 42:538-541
Bailey, Byron & Johnson Jonas; Head and Neck Surgery--Otolaryngology 4th ed. 2006