
click on image above to enlarge; advance with cursor over border
return to: Tracheotomy - Tracheostomy
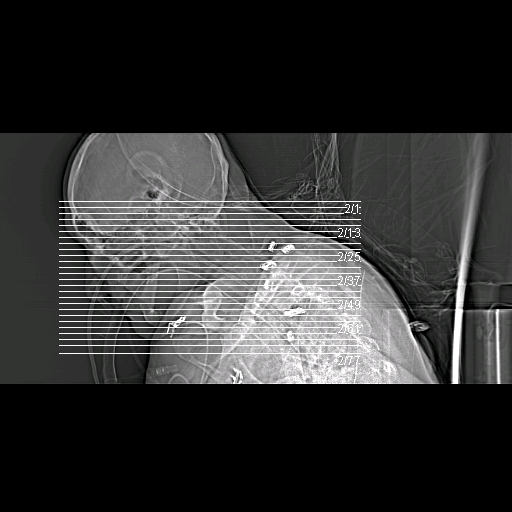
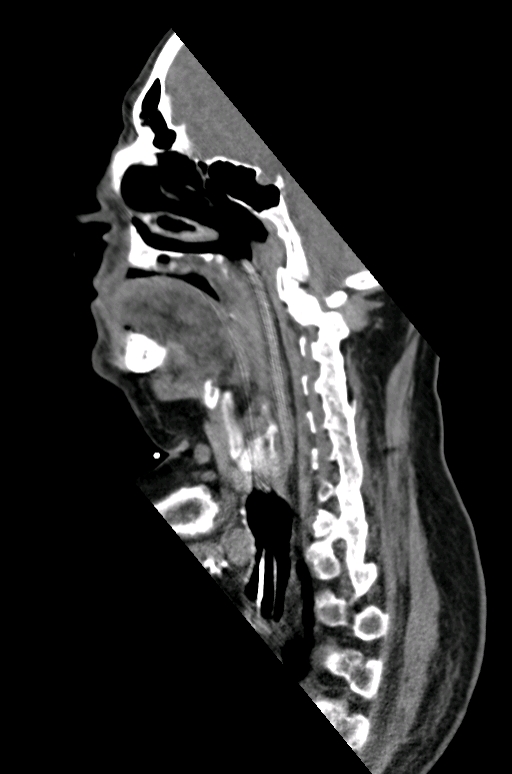
56 yo with ankylosing spondylitis with neck flexion and retrosternal larynx/cricoid. Need for prolonged intubation for complications associated with / diabetes / h/o urosepsis with stone / diabetes / s/p lower spine fixation for unstable fracture by orthopedics.









Procedure performed
Epithelial lined tracheotomy with:
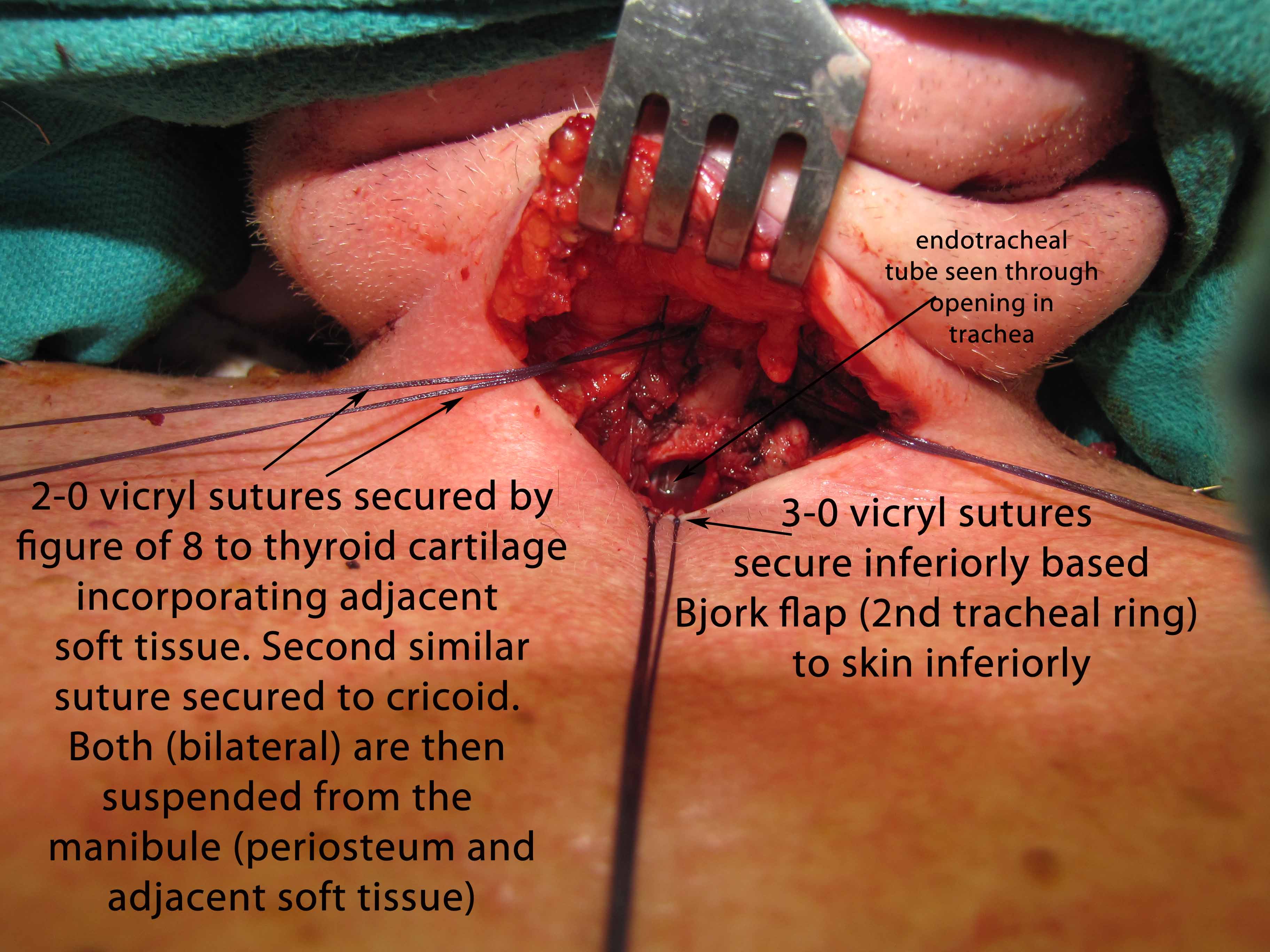
Suspension laryngoplasty - 2-0 vicryls stay sutures x 4 (two to each side) suspending the larynx to the mandible (sutures placed with figure-of-8 through lower thyroid and upper cricoid cartilages incorporating soft tissue and placed through periosteum of mandible superiorly)
Anterior cervical lipectomy with plication of skin to underlying strap musculature (providing additional pull superiorly on the larynx)
Modified and edited operative note
Patient is 56 yo male with ankylosing spondylitis, respiratory failure and urosepsis. Anatomy precludes normal tracheotomy. Requires long term ventilatory assistance.
Procedure Details:
Risks, benefits, indications, alternatives and procedure were explained to the patient's family. All questions were answered. Informed consent was obtained. The patient was brought intubated from the SICU to the main operating room. The patient was placed in a supine position using full spine precautions, with all points of back and head supported, as per orthopedic recommendations. Orthopedics verified the positioning. Time out was performed. The patient was placed into reverse Trendelenburg, and direct laryngoscopy was performed with a MAC blade. Grade IV view was obtained. The procedure was repeated with a glide scope which, with some manipulating, did permit good view of the cords. The procedure was repeated a third time with a Holinger anterior commissure scope, with a exposure of the cords. The endotracheal tube was noted to be passing through the cords. There was copious mucus in the oropharynx and subglottis. There were no lesions or irregularities of the vocal cords. Photodocumentation was obtained with a 0 degree rigid scope.
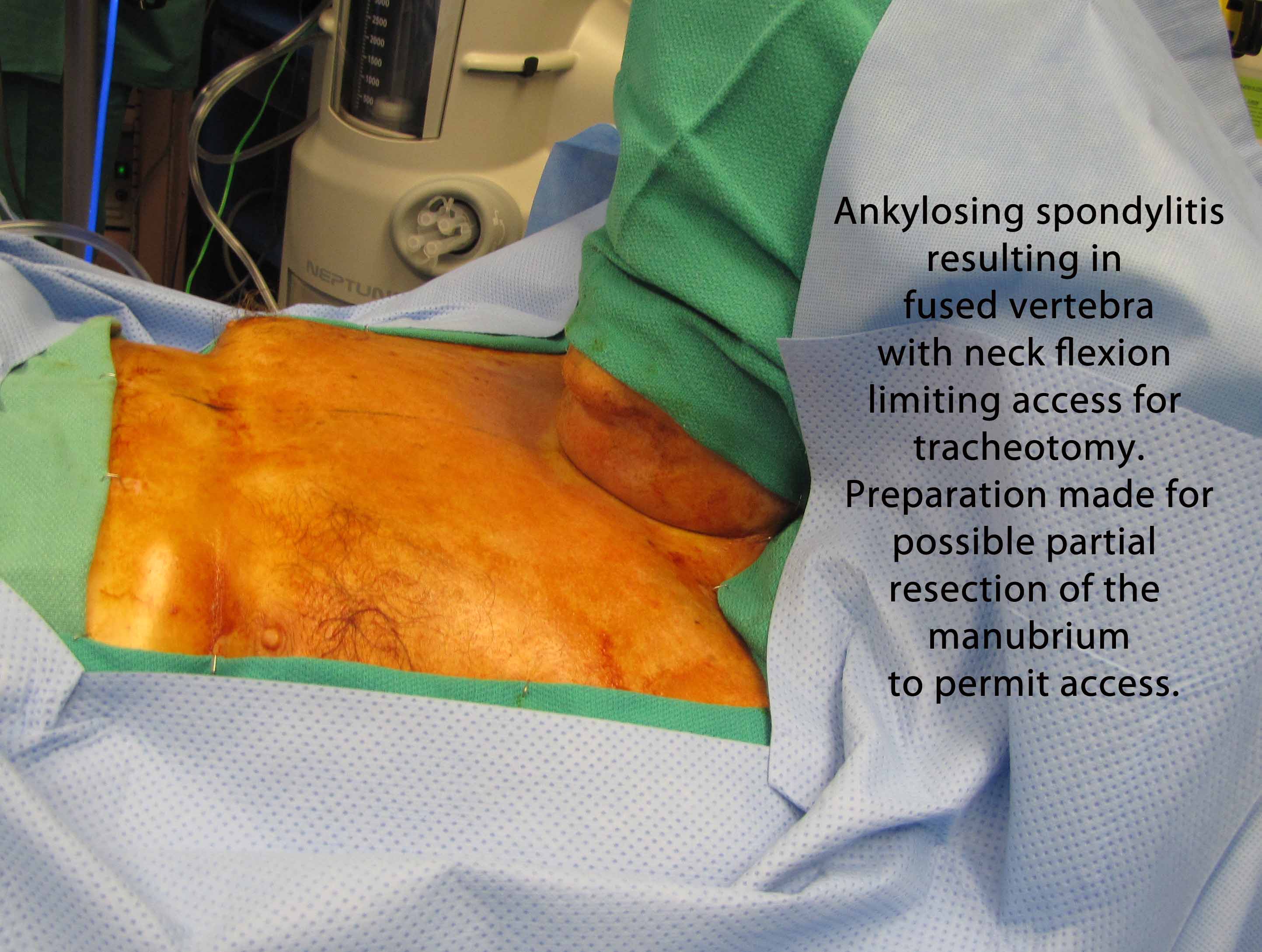
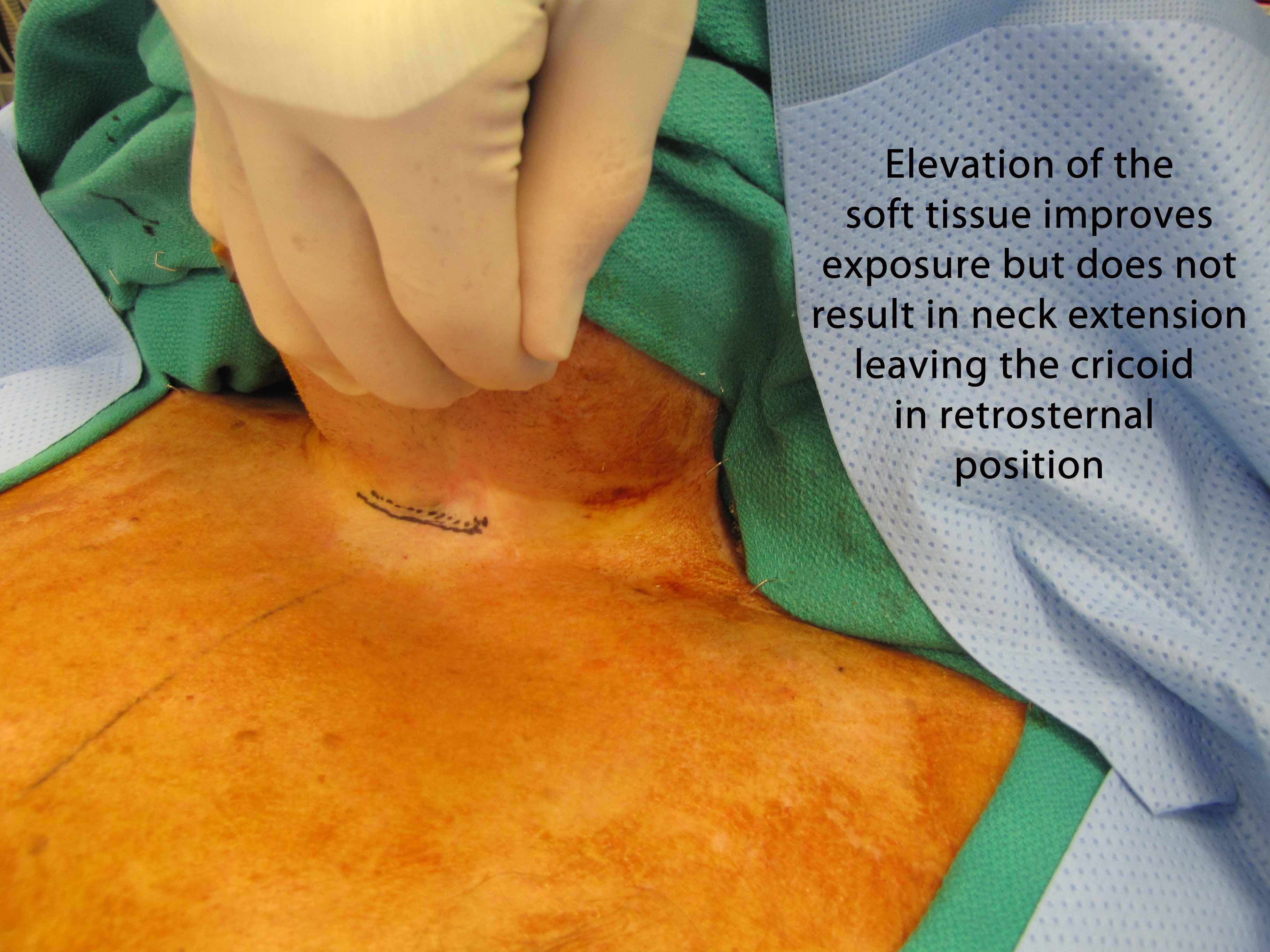
Attention was then directed to the planned tracheotomy. The hair on the chest was shaved in preparation for possible need for resection of manubrium or sternal split. The Cardiothoracic Surgery Service stopped by and was available throughout the case. The patient was prepped and draped for tracheotomy as well as sternal split. The anatomy was evaluated, and there was found to be extreme kyphosis. The neck was nonmobile, with the chin flex forward to the sternum. The upper aspect of the thyroid cartilage was palpable at sternal notch.
A horizontal incision site was planned 1 cm above the level of the sternal notch. Seven ml 1% lidocaine with 1:100,000 epinephrine were injected into the area. Incision was made with a 15 blade with Bovie and was carried down to the level of the straps. A subplatysmal flap was elevated superiorly to the level of the mandible, with care to stay just in the midline in level 1 to avoid the marge. Inferiorly, the flap was carried down above the level of the sternum. Defatting was performed from the level of the sternum up to just superior to the hyoid bone. The periosteum of the sternal notch was exposed.
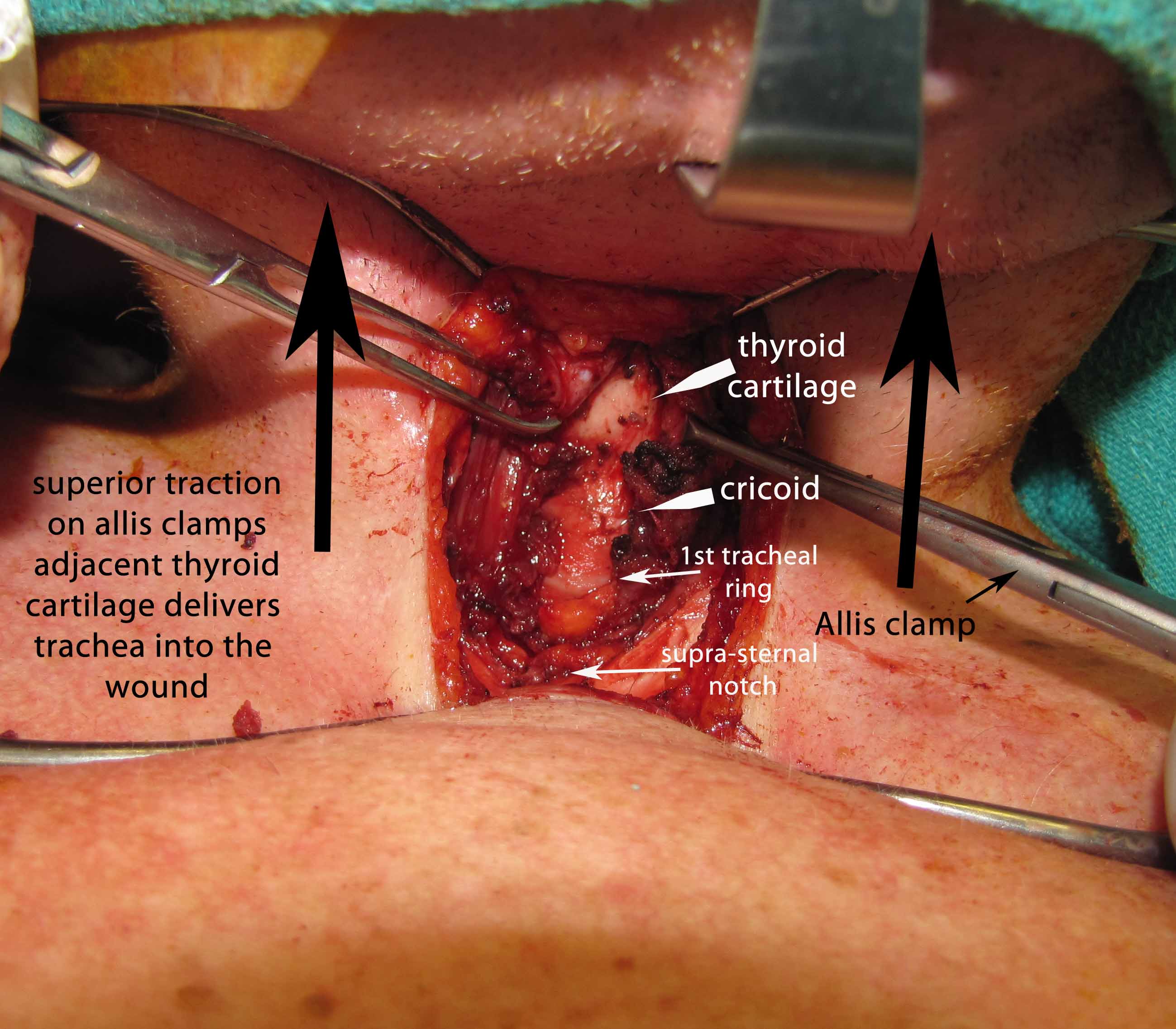
Dissection was carried down between the strap muscles onto the thyroid cartilage, which was at the level of the sternal notch. Careful dissection was carried down substernally down the anterior face of the trachea, and the tracheal rings were exposed. The larynx was noted to be extremely mobile and could be pulled superiorly into the neck employing Allis clamps placed laterally on the soft tissue adjacent the lateral borders of the thryoid cartilage.
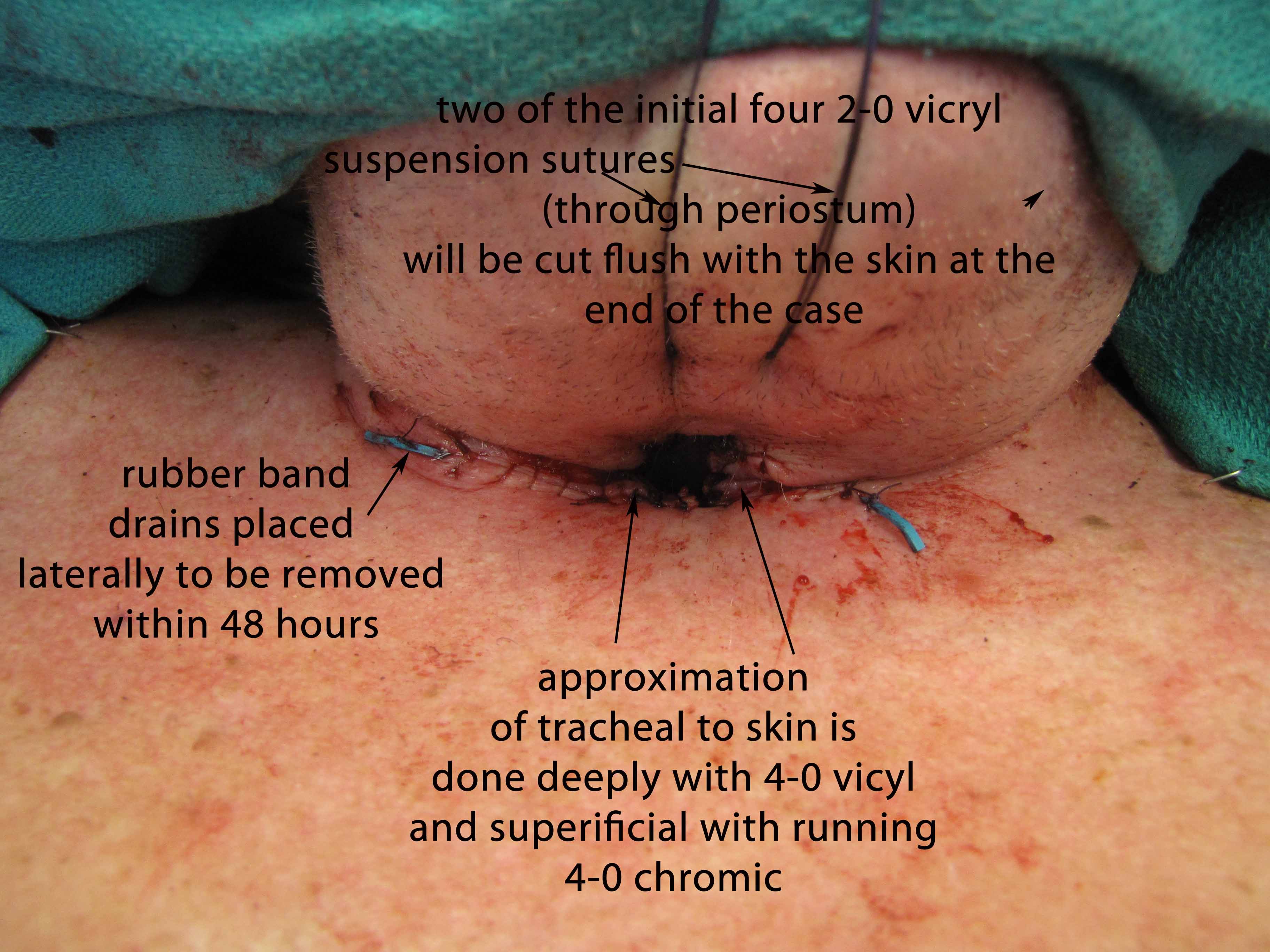
The strap muscles from the hyoid to the thyroid cartilage were partially divided. The cricoid was found to be partially fused to the thyroid cartilage itself. There was evidence of a previous tracheotomy site on the right lateral aspect of the first tracheal ring. Suspension laryngoplasty was then performed using 2-0 Vicryl stay sutures x 4 (2 on each side), suspending the larynx to the mandible. Sutures were placed with figure of eight through the lower thyroid and upper cricoid cartilage, incorporating soft tissue, and then placed through the periosteum of the mandible superiorly. This significantly elevated the level of the larynx, and the trachea was accessible, now superior to the level of the sternal notch. Plication of the superior skin flap to the underlying strap musculature was then performed using 2-0 Vicryls, providing additional pull superiorly on the larynx. This was performed after limited anterior cervical lipectomy.
With the trachea now elevated into the neck, tracheotomy was planned through the lower border of the first tracheal ring. Ventilation was stopped (brief apnea) with the endotracheal tube mobilized with cuff deflated and pushed inferiorly - "mainstemmed" - to keep the cuff from being fenestrated in the process of entering the trachea. The airway was entered with a hemostat, and an inferior based Bjork flap was created. Through the opening in the trachea, the endotracheal tube was visualized and pulled back appropriately with the cuff then reinflated (under direct vision) immediately below the tracheal opening. The Bjork flap was sutured to the skin in the manner of an epithelial lined trach inferiorly. A square of skin at the midline of the superior skin flap was resected, and the skin edges were secured to the left, right, and superior cartilage of the tracheostome.
An epithelial lined trach was performed. The skin edges were secured down to the trachea with 2-0 and 4-0 Vicryls. A rubber band drain was placed on each side of the incision.
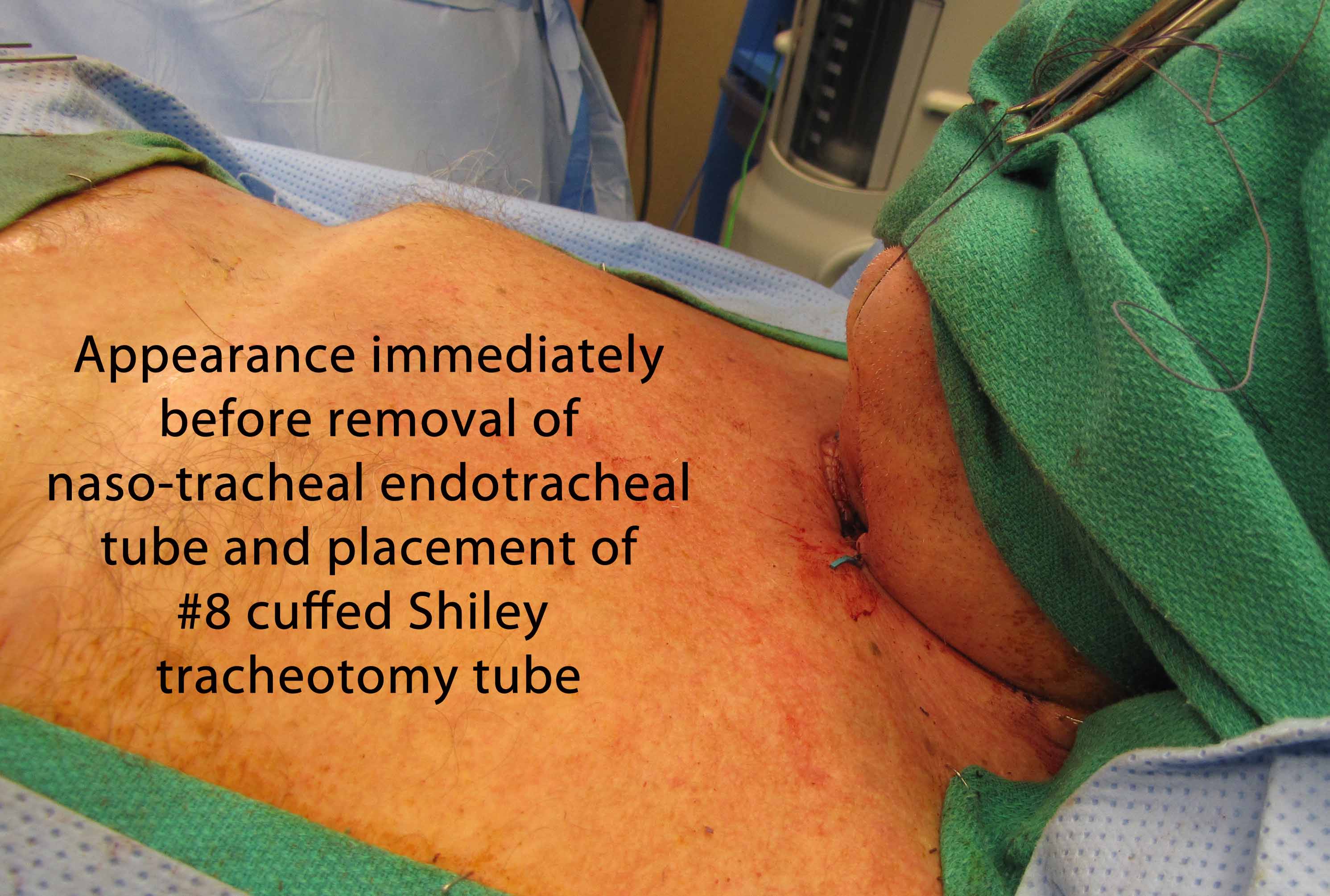
The tracheostome was matured with deep 4-0 Vicryls and superficial running 4-0 chromics. The endotracheal tube was retracted back, and an 8.0 Shiley was placed into the newly formed epithelial lined tracheotomy. The flange on the tracheotomy was noted to be pressing into the skin due to patient's severe kyphosis. The superior and inferior aspects of the flange were therefore trimmed and smoothed to allow better fit. The position of the tip of the tracheotomy tube was then verified was verified with flexible bronchoscopy through the tracheotomy tube. It was found to be sitting in good position, with good view of the carina. The trach was secured in place with a trach strap with drain sponges placed under the flanges.
Direct laryngoscopy was repeated using the Holinger anterior commissure scope. In addition to the bifid uvula identified previously, and the epiglottis was noted to be now elevated nearly to the level of the nasopharynx, confirming success of our suspension laryngoplasty, with successful elevation of the trachea into the neck. Direct laryngoscopy was performed, with good view of the cords despite the new superior position of the epiglottis.
At the request of the SICU staff, the transnasal Dobbhoff tube was resutured into place with no complications. The patient was transferred back to the SICU bed using full spine precautions, and was transported back to the SICU fully sedated and on the ventilator. The patient tolerated the procedure well, and there were no complications.
References
Patel KC and Zdanski CJ: Cricothyroidotomy vs. Sternal Tracheotomy for Challenging Airway Anatomy. Laryngoscope, 118:1827-1829, 2008
Prasai A, Jani P, and Jones G: Failed Intubation in a Patient With Long-Standing Ankylosing Spondylitis.
Deslauriers N, Jacques F, Danino A, Harris P, Martin J, Liberman M, Duranceau A and Ferraro P: Lateral mediastinal tracheostomy in benign disease: an uncommon procedure for a rare indication. Ann Thorac Surg 2010 Mar; 89)3):979-81