

















F/u treatment in clinic to ensure ductal patency:
Ultrasound Sialography (Ultrasound With Salivary Duct Infusion)
return to: Instructions to patients - parotid salivary stones
Modified Operative Note
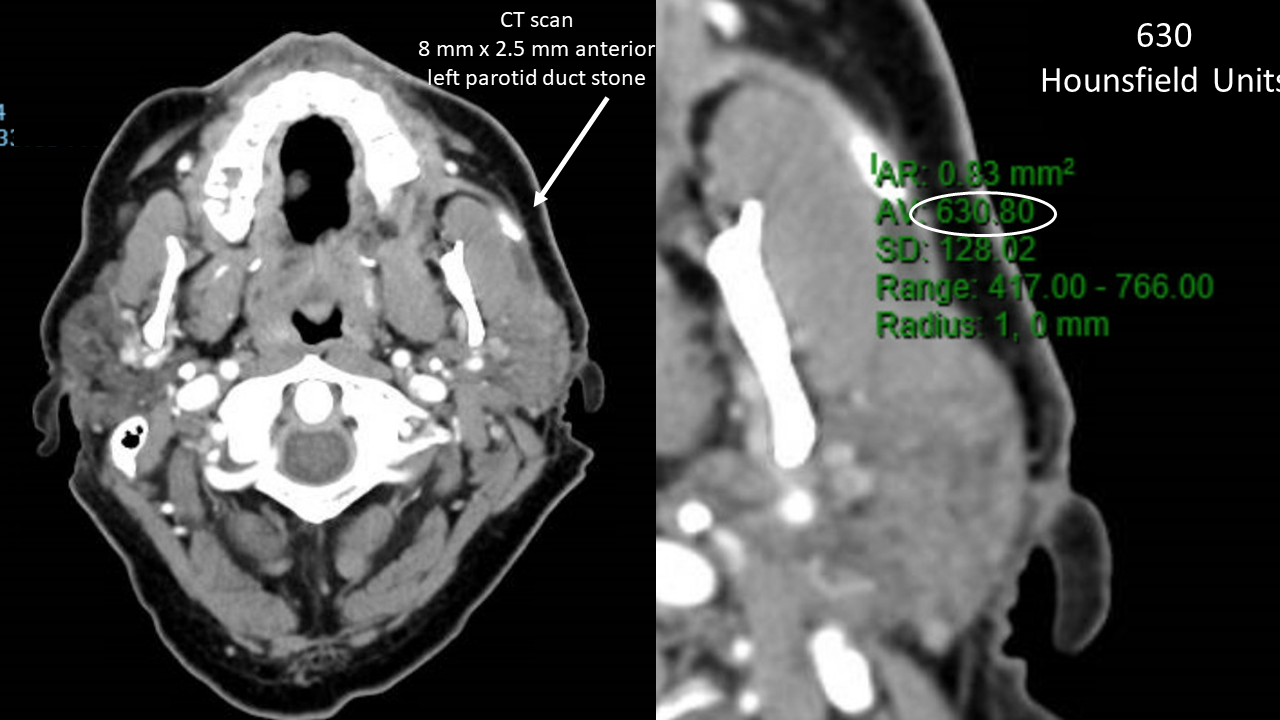
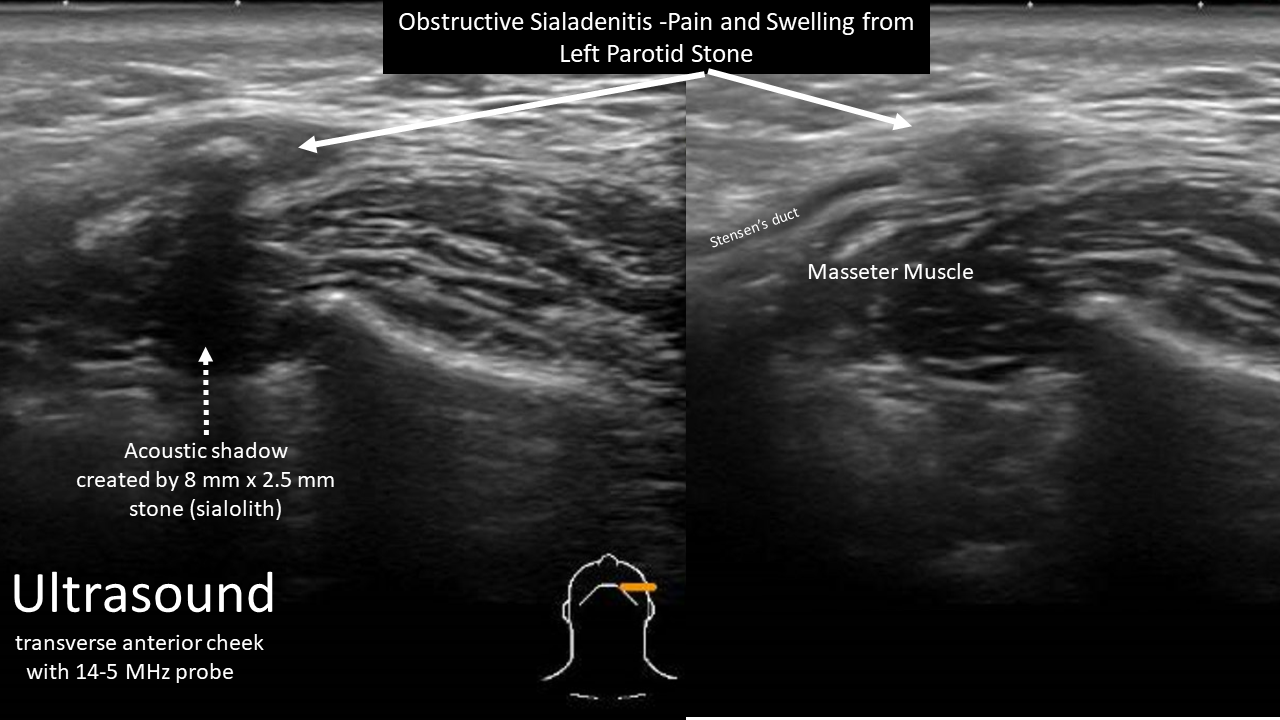
Preop Dx: Left parotid sialadenitis with sialolithiasis
Postop Dx: Same
Procedure:
Complex (open) left parotid sialodochoplasty including intracorporeal laser (Holmium) lithotripsy with
Sialendoscopy
A. 1.6 mm Zenk scope used to deploy forceps, baskets (used both the N-circle and N-gage) and laser
B. 0.8 mm Zenk to place type 3 Sialo drain 6F x 120 mm trimmed to length of 5 cm with tapered tip and confirmed placement with scope during placement
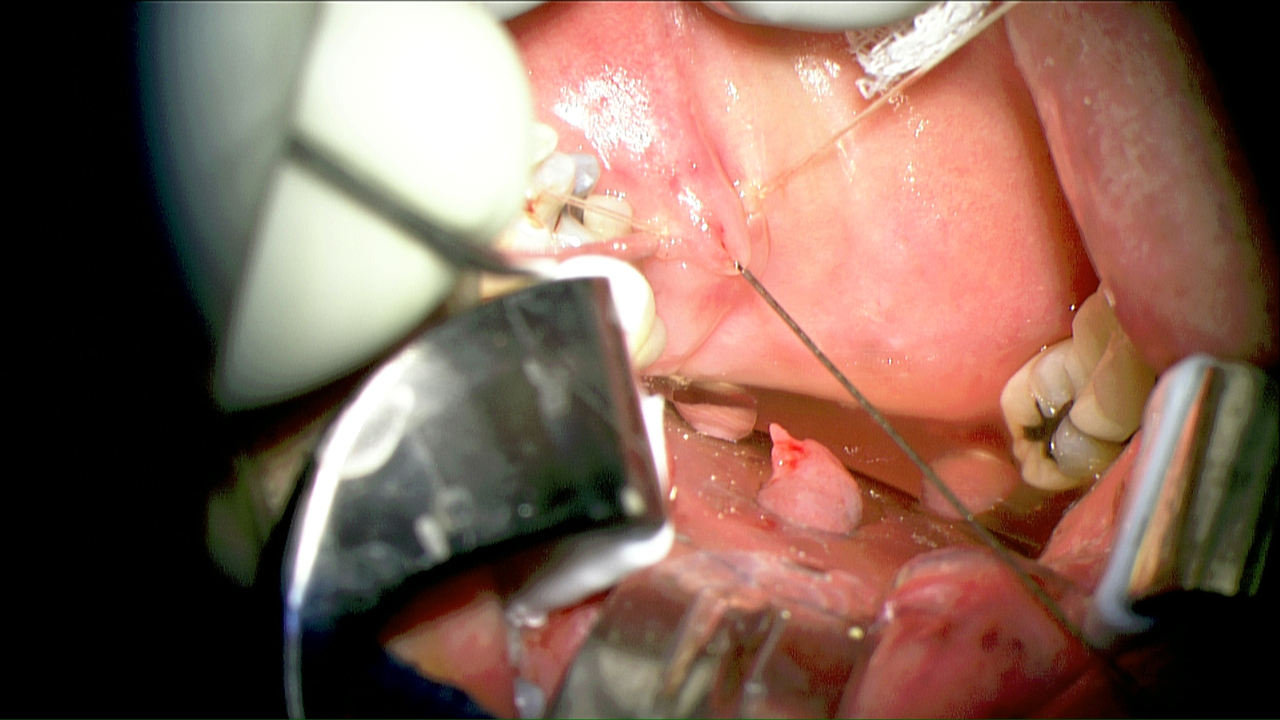
Removal of stone through combination of holmium laser (see below), basket, forceps and then direct removal with open ductoplasty employing microscope and 1.6 mm sialendoscope with basket retrieval of largest most proximal fragment
Open ductoplasty initiated with 5-0 vicryl stay sutures then placement of sialodrain secured with two separate 5-0 nylon to secure
Kenalog 10 (5 cc) placed through sialodrain
Anesthesia: Glide scope (required for access)
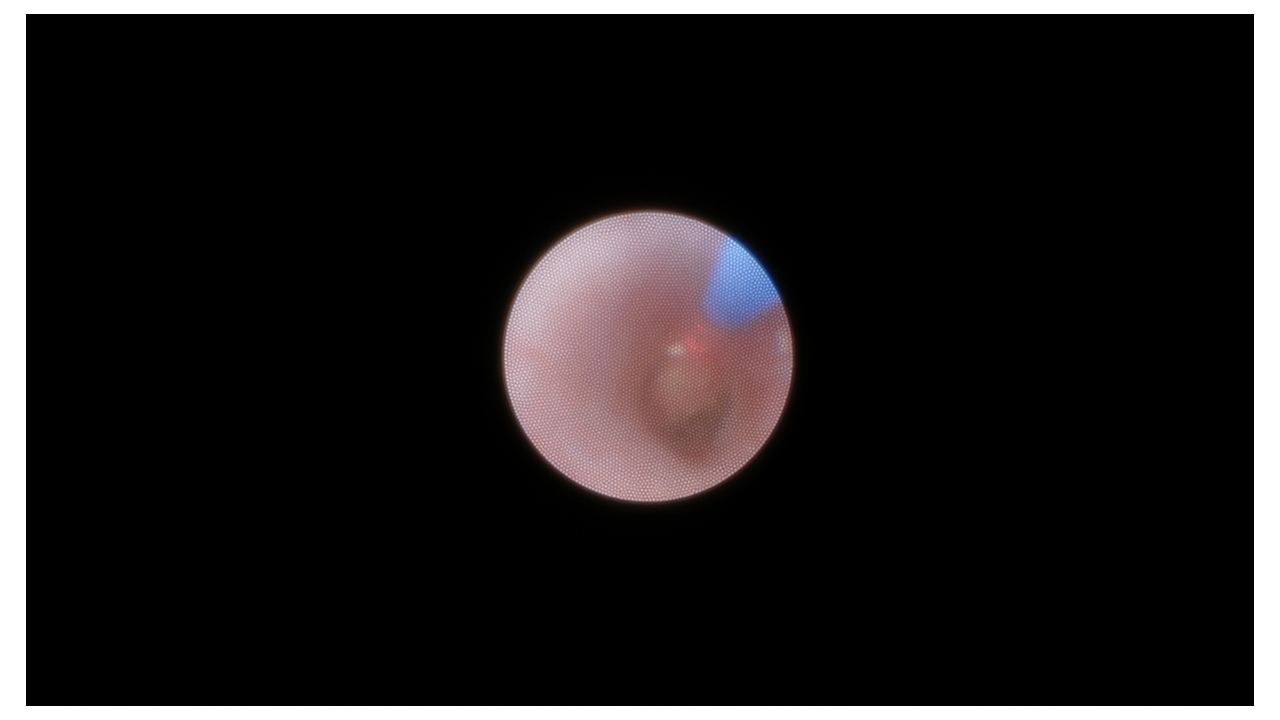
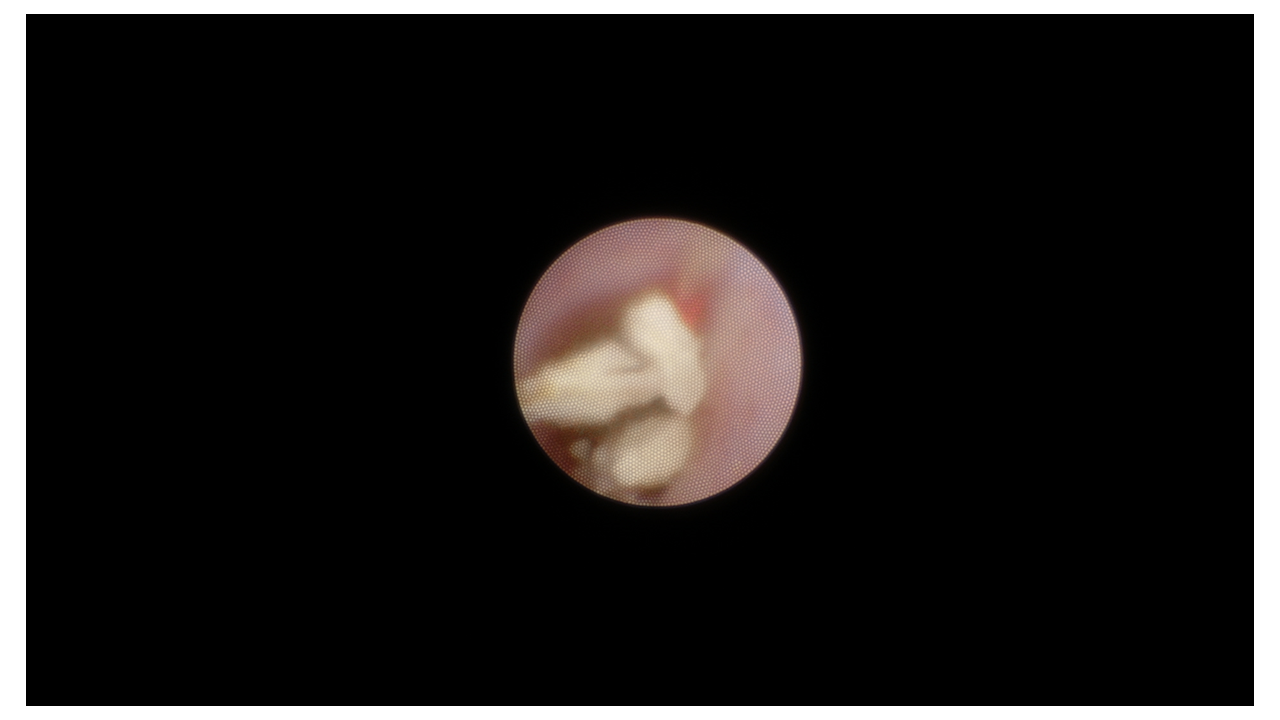
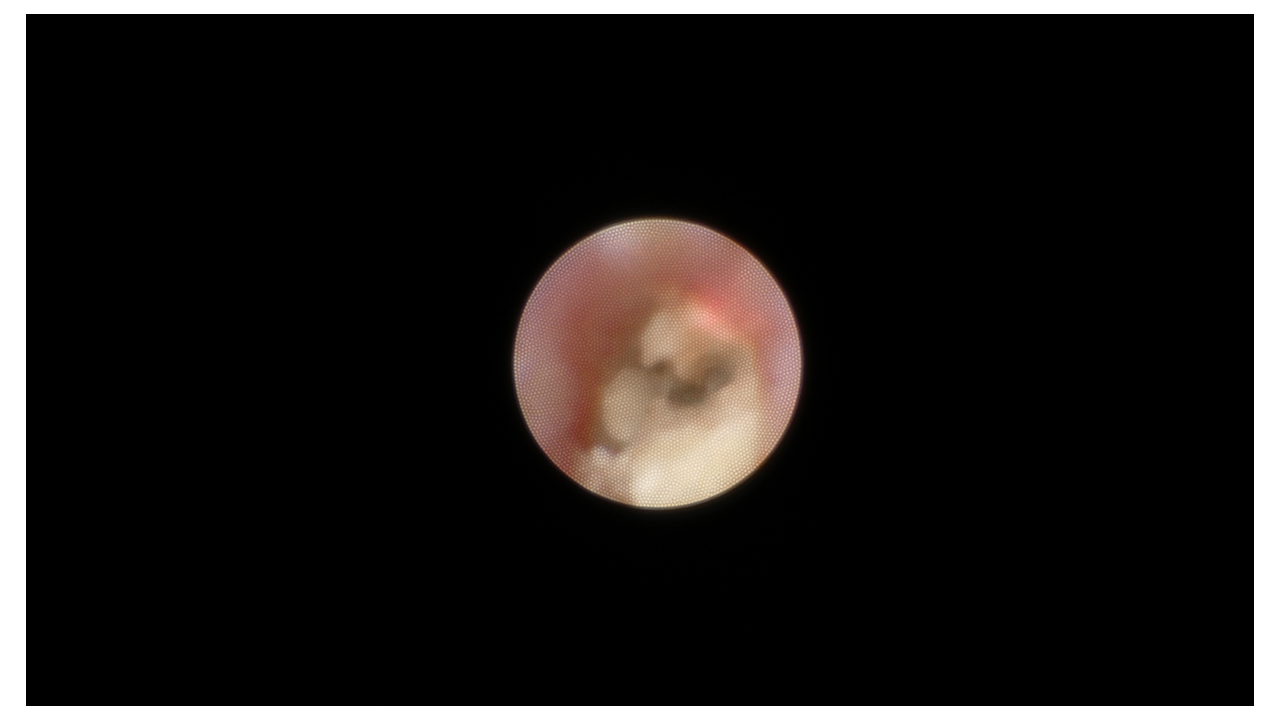
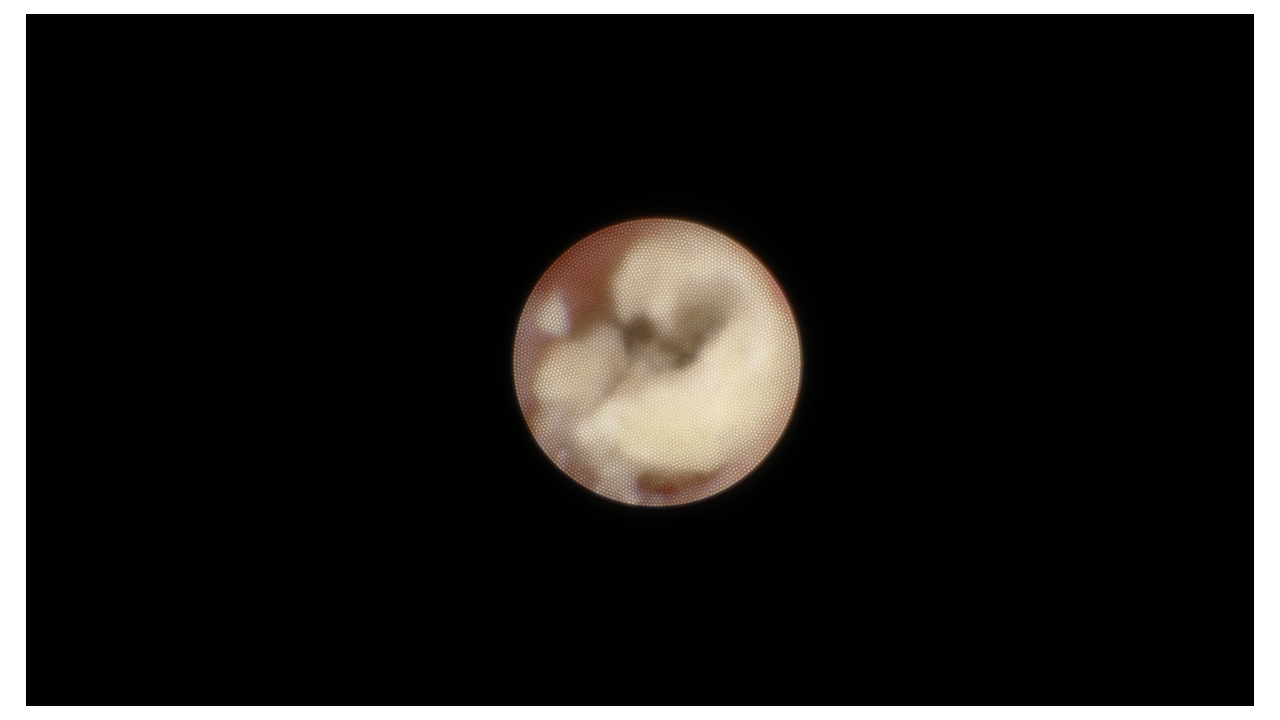
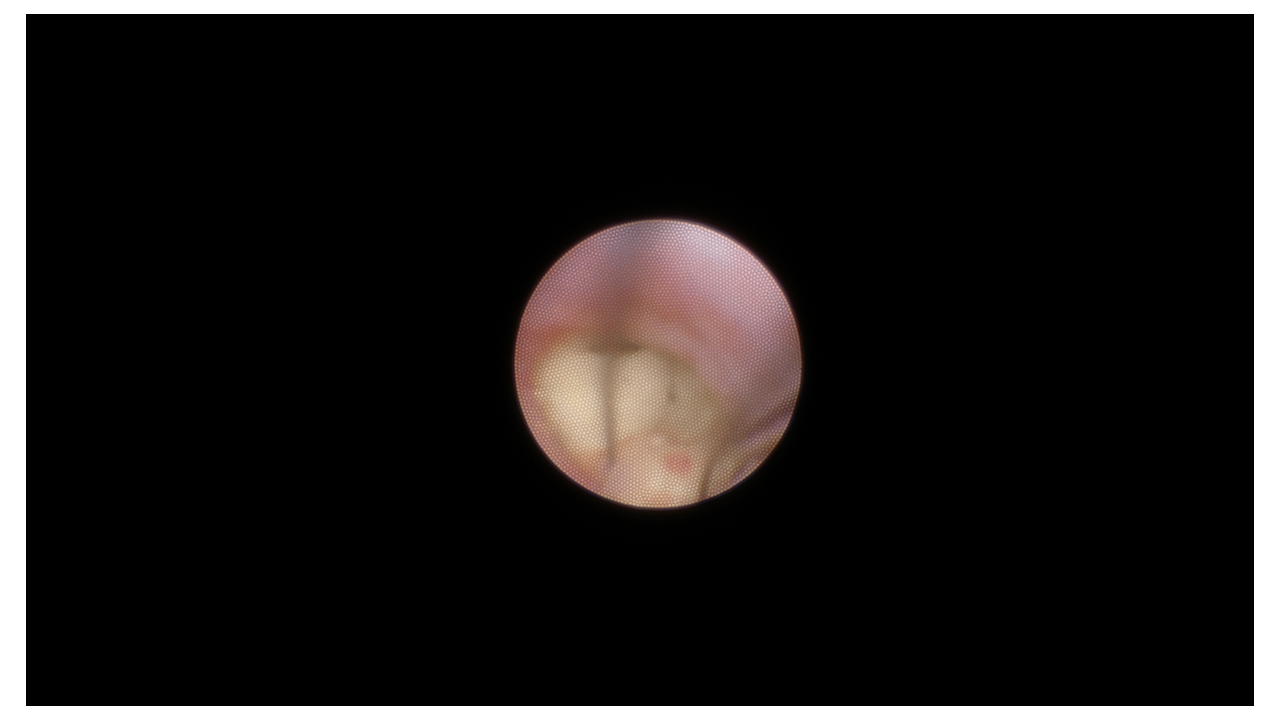
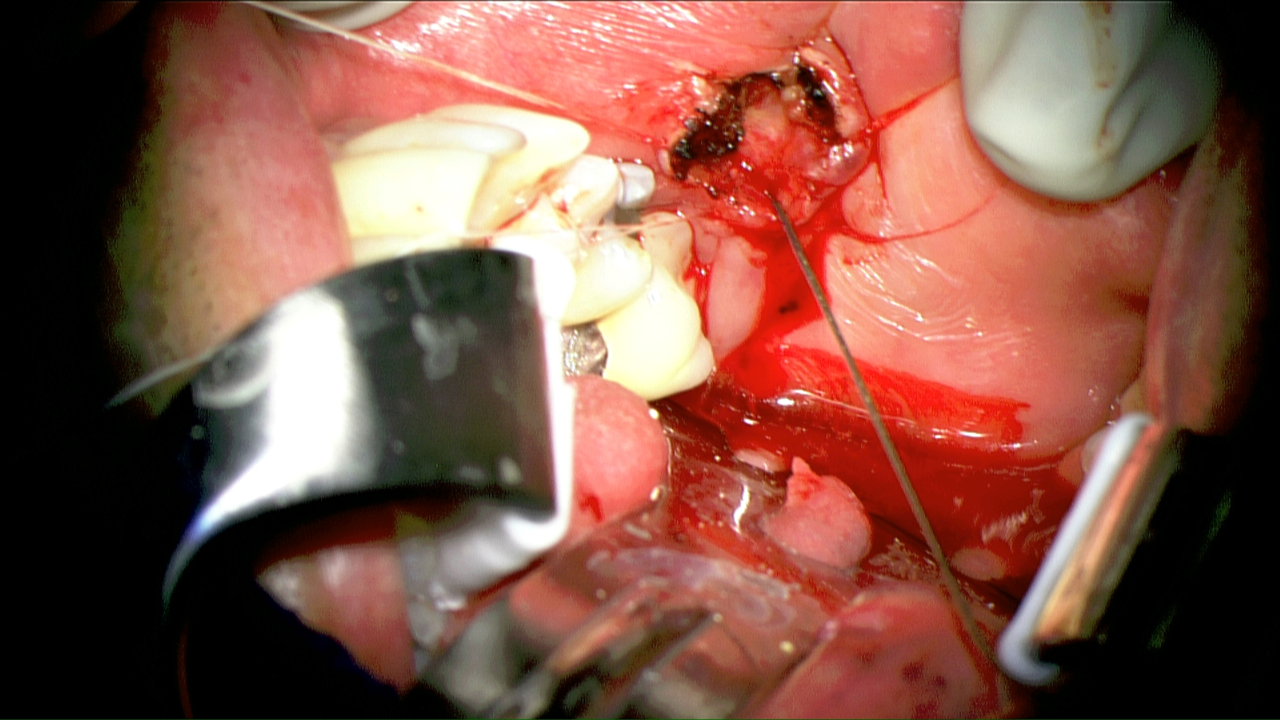
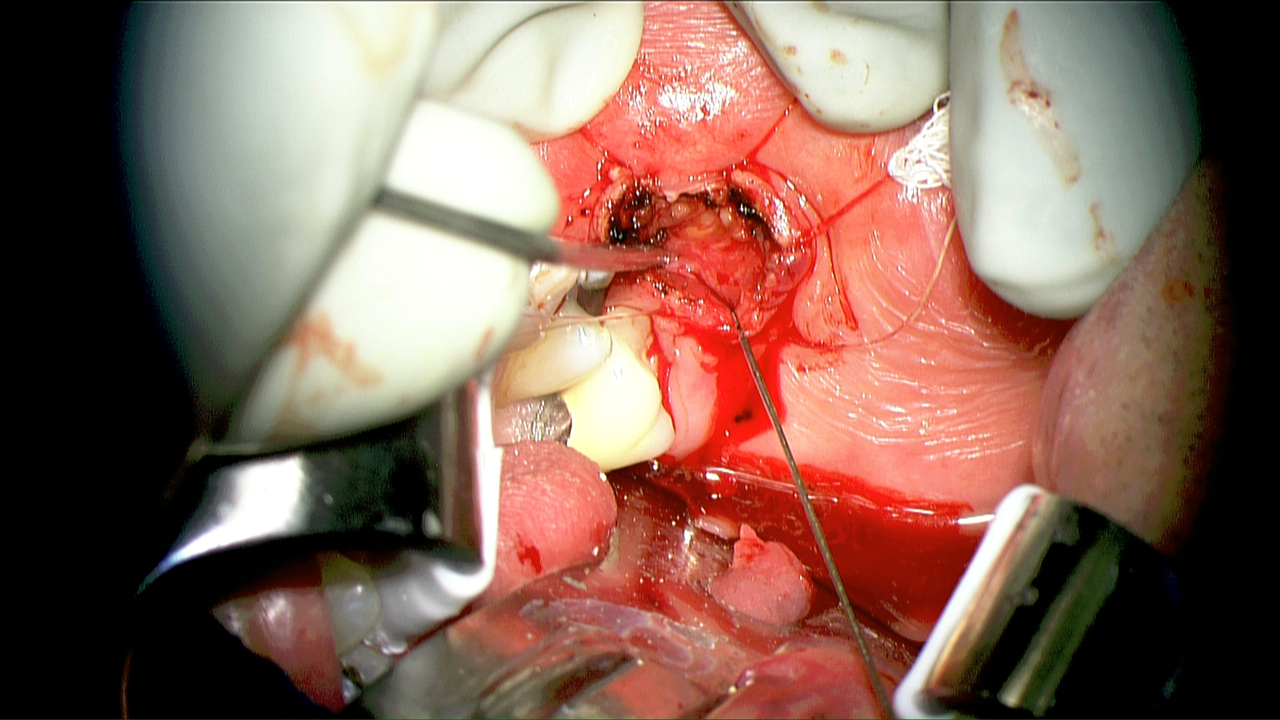
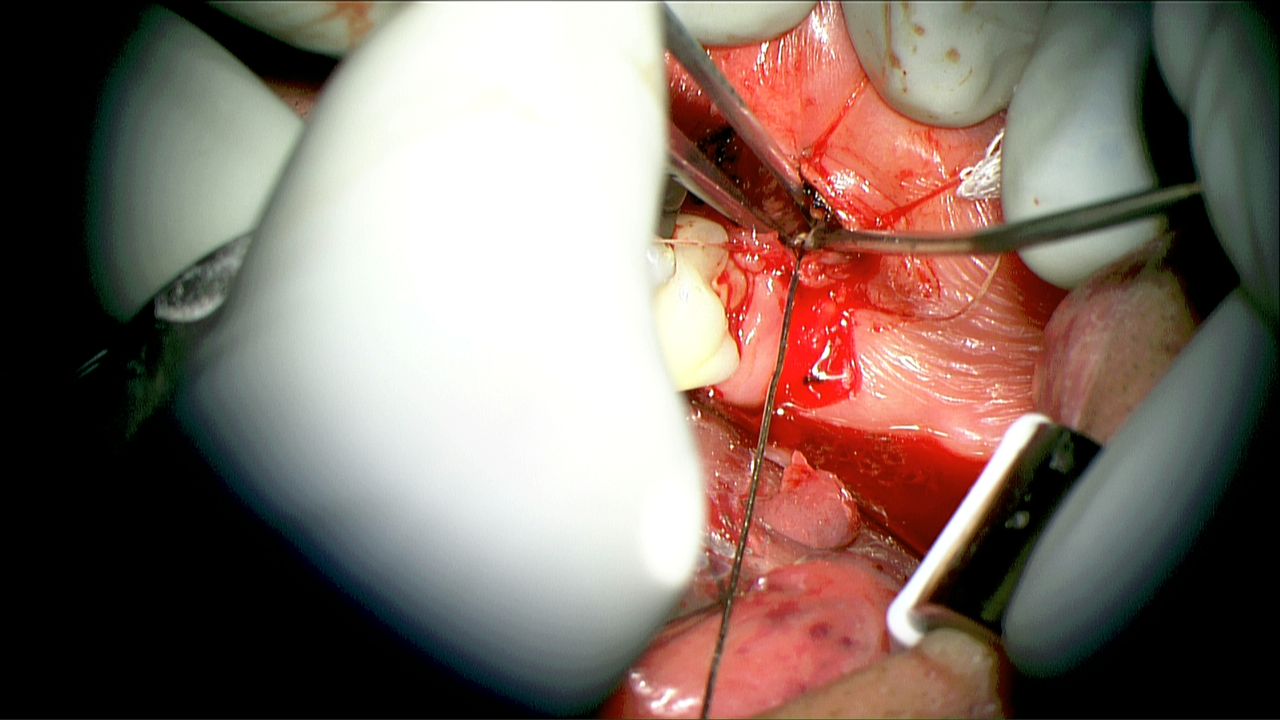
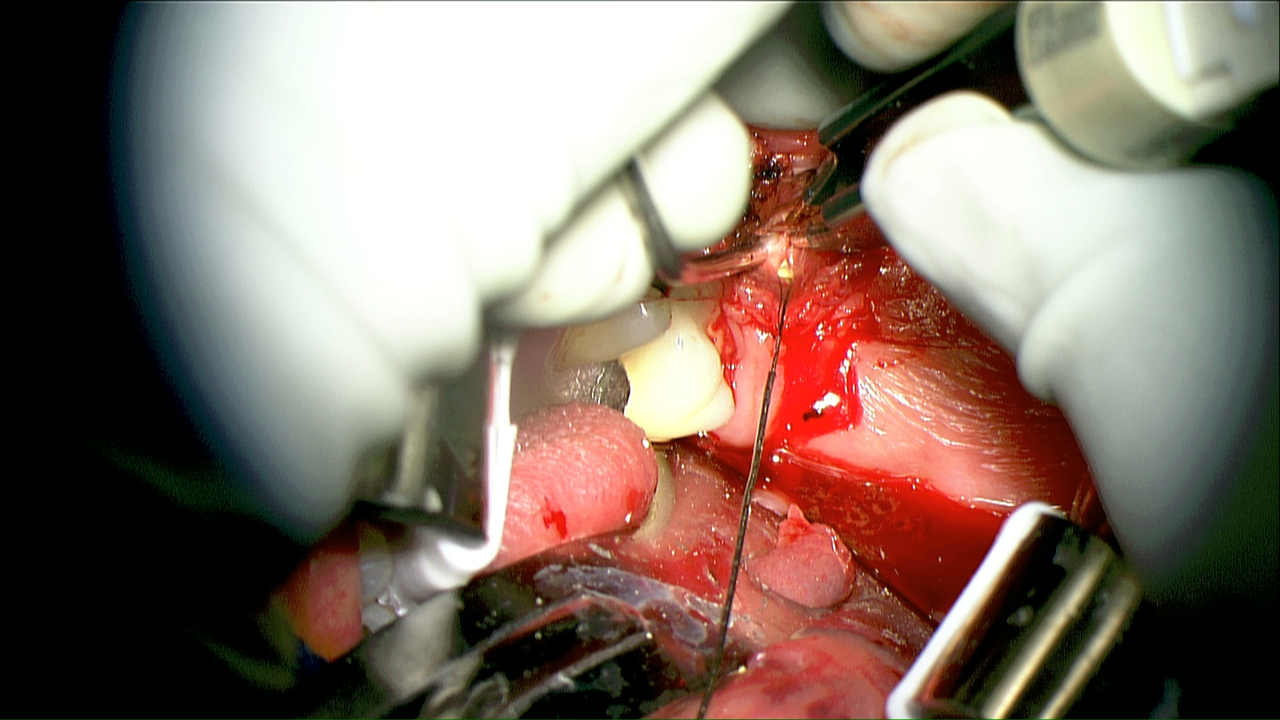
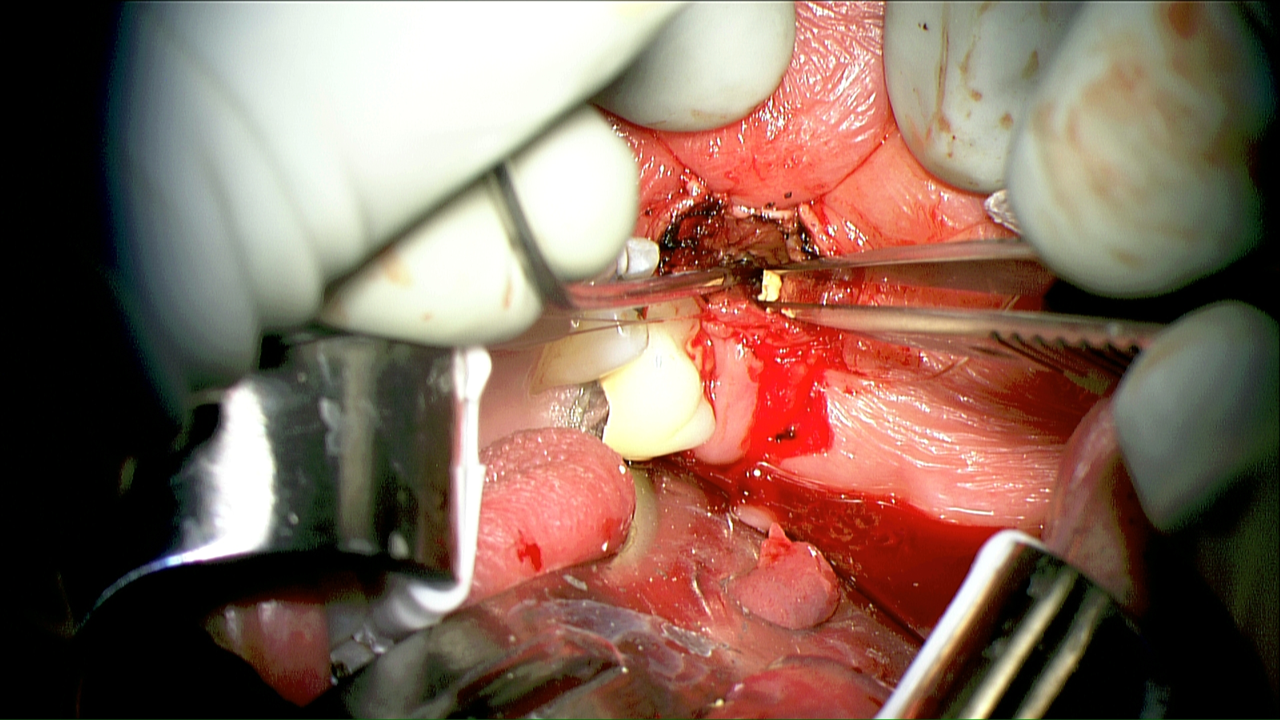
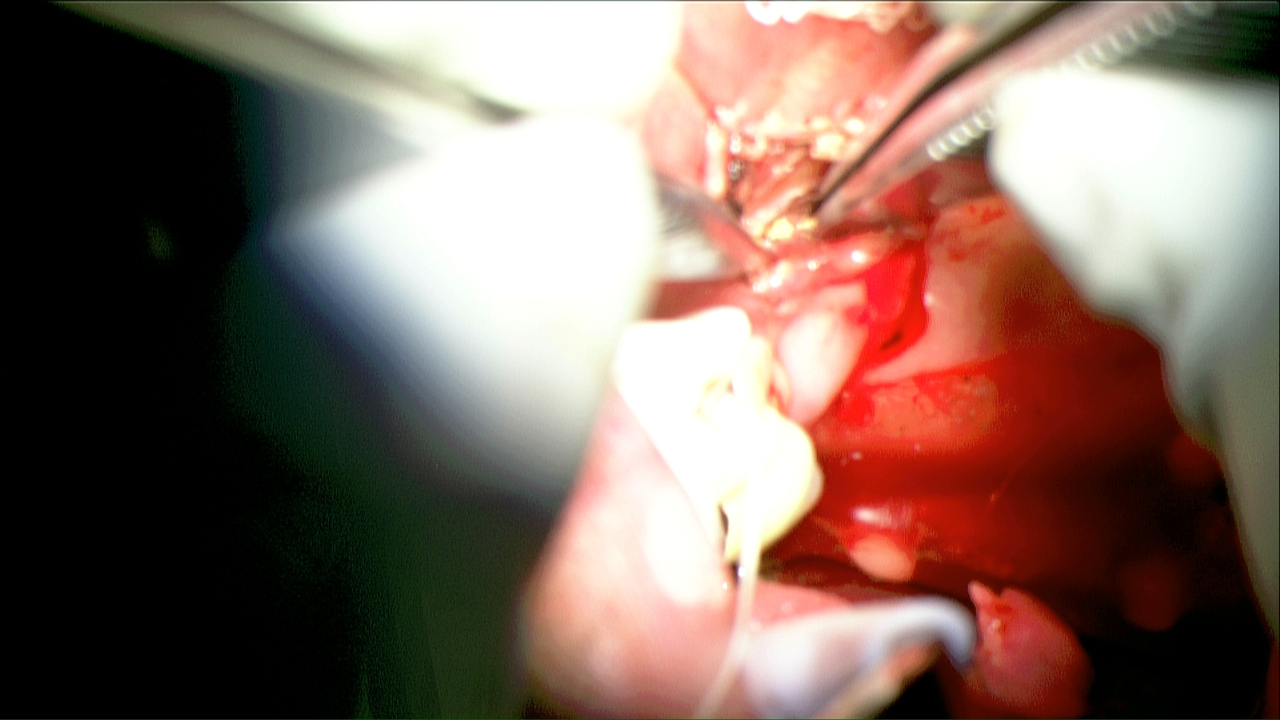
Findings as per above and photos below - in addition:
Efforts at laser made slight progress but required open approach facilitated by 'trapping' the mid and anterior aspect of stone with the N-circle basket with continuous applied traction (as per 'fishing line') permitting placement of stay sutures and superior opening of duct orifice to permit both direct removal of stone (forceps) and placement under microscope control of basket around final stone remnant for clearance
Duct inspected with 1.6 mm Zenk scope after above showing no residual stone - some laser injury to duct bypassed with stent (sialodrain)
.31 Kj Holmium layer application intracorporeal lithotripsy 0.3 J to 0.5 completed with 0.6 J, Rate 5 pulses per second, Power = 1.5
Plan: Augmentin 875 mg po bid for 10 days; medrol dose pack, peridex oral rinses swish and spit qid for 3 weeks (until time of f/u); f/u 3 weeks for stent removal (predate with phone call two days before)
References
Su CH, Lee KS, Tseng TM, Hung SH. Post-sialendoscopy ductoplasty by salivary duct stent placements. Eur Arch Otorhinolaryngol. 2016 Jan;273(1):189-95. doi: 10.1007/s00405-015-3500-5. Epub 2015 Jan 8. PMID: 25567347.
Magdy EA, Seif-Elnasr M, Fathalla MF. Combined sialendoscopic/mini-preauricular microscopic approach for large proximal parotid sialolithiasis. Auris Nasus Larynx. 2021 Oct;48(5):983-990. doi: 10.1016/j.anl.2021.01.018. Epub 2021 Feb 10. PMID: 33581935.
Han PS, Kim Y, Yoo TS, Lee S, Inman JC. Sialodochoplasty Stents: Cost Analysis and Outcomes. J Oral Maxillofac Surg. 2017 Mar;75(3):536-542. doi: 10.1016/j.joms.2016.09.008. Epub 2016 Sep 15. PMID: 27725105.
Van Sickels JE. Management of parotid gland and duct injuries. Oral Maxillofac Surg Clin North Am. 2009 May;21(2):243-6. doi: 10.1016/j.coms.2008.12.010. PMID: 19348990
Irawati N, Clark JR. Microsurgical reconstruction of Stensen's duct using autologous vein graft and venous coupler after ablative head and neck surgery. ANZ J Surg. 2021 May;91(5):1017-1018. doi: 10.1111/ans.16769. Epub 2021 Apr 13. PMID: 33848041.