





click on image above to enlarge; advance with cursor over lateral border
return to: Case example Submandibular Gland Resection
Modified Operative Note
Indications: Pleomorphic adenoma of the left submandibular gland.
Procedure Details:
Informed and written consent was obtained. The patient was then transferred to the OR and placed in the supine position. He was endotracheally intubated by anesthesia. The bed was rotated 180 degrees and he was prepped and draped in a sterile fashion. A horizontal incision was marked out 2 fingerbreadths below the inferior border of the mandible that extended from the anterior border of the sternocleidomastoid muscle to the midportion of the ipsilateral anterior belly of digastric muscle. A number 15 blade was used to create the initial incision. The platysma was identified and incised to expose the anterior border of the SCM with preservation of the great auricular nerve.
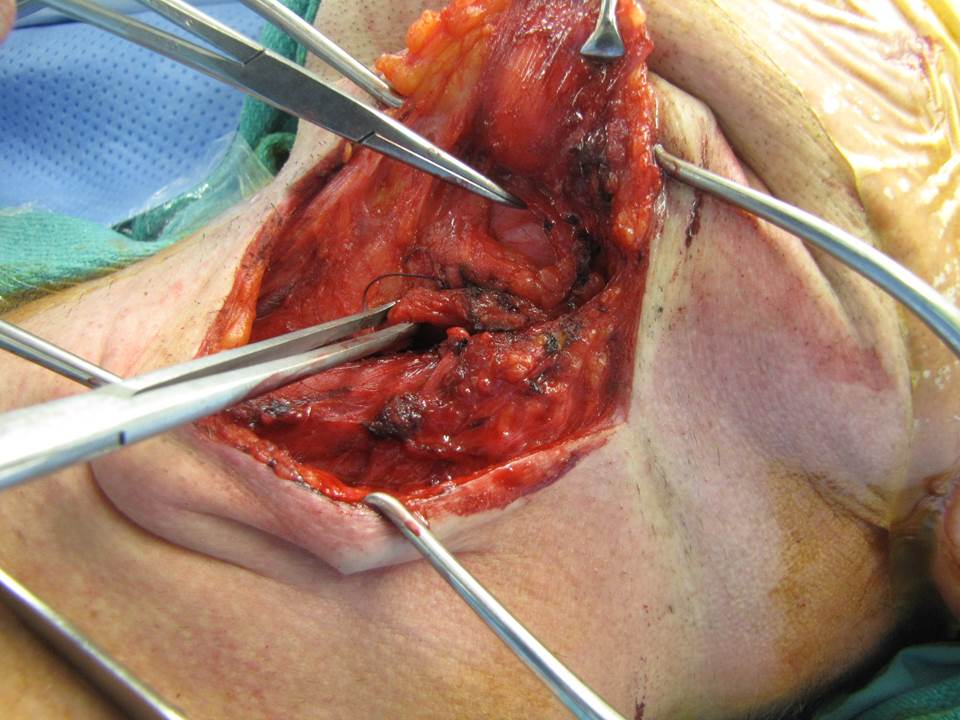
The posterior inferior aspect of the submandibular gland was then identified immediately anterior to the sternocleidomastoid muscle. The marginal mandibular nerve was then identified and preserved at this time with the assistance of the Checkpoint nerve stimulator while raising the superior platysmal flap.
The gland was exposed and retracted inferiorly. The digastric muscle was identified along its course extending to its anterior belly.
Soft tissue was preserved over the gland to improve the margin of resection and the anterior aspect of the gland was mobilized from and anterior to posterior approach to expose the mylohyoid muscle.
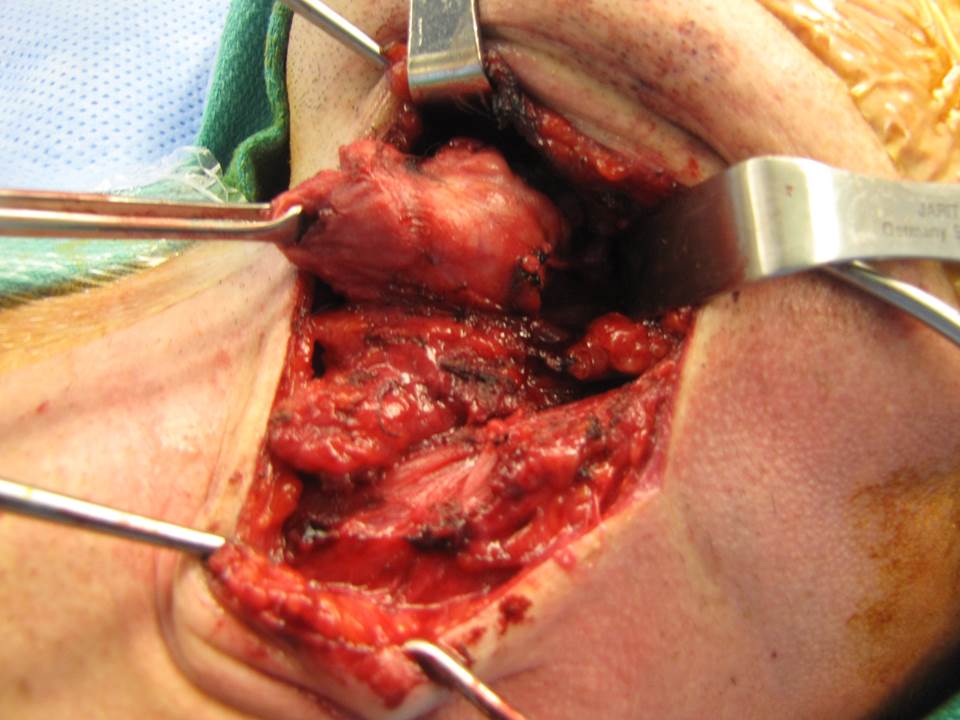
An Army-Navy retractor was then placed under the posterior border of the mylohyoid muscle to retract anterosuperior to expose the lingual nerve and submandibular duct. The submandibular ganglion was suture ligated, releasing the lingual nerve.
Wharton's duct was traced anteriorly and transected after placement of a hemoclip on the duct under the lingual nerve.
The gland was dissected posteriorly to encounter and ligate the branch from the facial artery perfusing the gland. Soft tissue attachments were severed with care to ensure the marginal mandibular branch of the facial nerve was retracted superiorly.
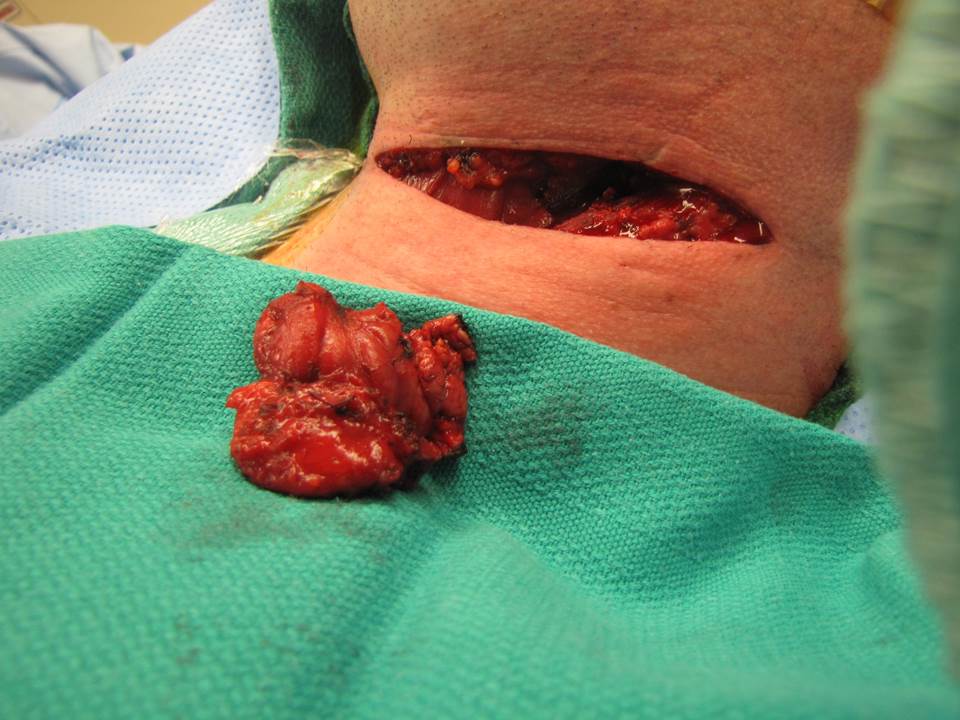
Final removal of the gland from the wound bed. With removal of adjacent level IIa lymph nodes.
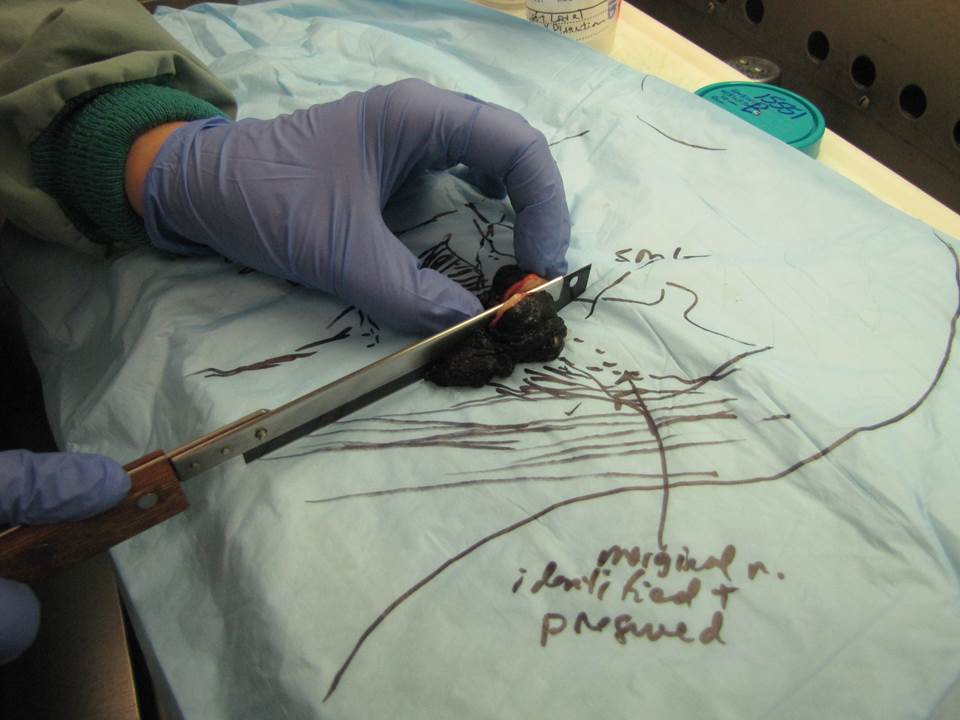
Specimen evaluated in pathology lab showing adequate gross margins where closest dissection to tumor over gland (where marginal mandibular nerve elevated)
Frozen section of resected specimen: c/w pleomorphic adenoma with clear margins
Final hemostasis was obtained.
A JP drain was placed posteriorly from the surgical dissection site. (versus option of penrose drain)
The wound was then closed with 3-0 Vicryl sutures deep, and 5-0 nylon for skin (alternatively, if closed suction drainage, then a 4-0 Monocryl suture may be placed in a subcuticular fashion with dermabond was then placed over the wound for final closure as in the photos above.