
")


")

")




















click on images above to enlarge; advance with cursor over lateral border to advance
return to: Subglottic stenosis
see also: Four-flap Epithelial Lined Tracheotomy; Case example four flap epithelial lined tracheotomy with thyroid isthmusectomy and anterior cervical lipectomy; Four-flap Epithelial Lined Tracheotomy; Passy Muir Valve and Provox XtraBase baseplate following four flap epithelial lined tracheotomy with thyroid isthmusectomy and anterior cervical lipectomy
Case Example
Emergent tracheotomy done 3 1/2 years ago due to inability to intubate at time of CABG (coronary artery bypass grafting). Tracheotomy tube was removed 3 months after it was placed due to poor tolerance "continuous coughing'. Despite successful use of CPAP, progressive shortness of breath warranted evaluation June 2011 with:
- Spiromtery with peak inspiratory flow rate = 1.95 liters/second
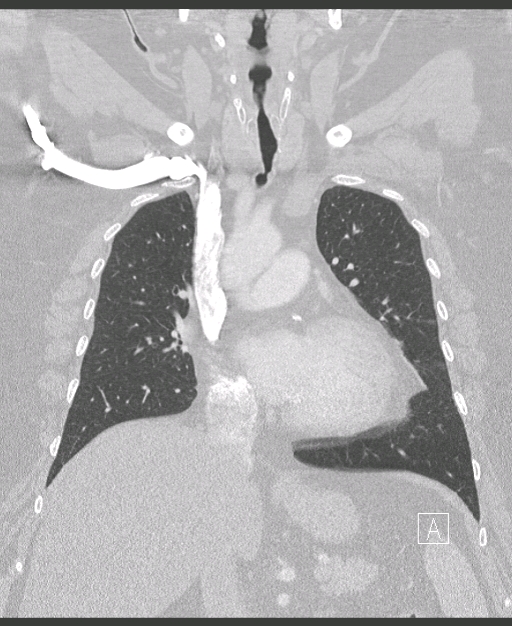
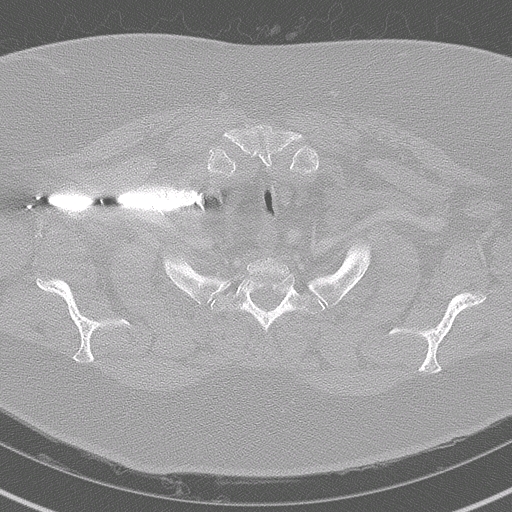
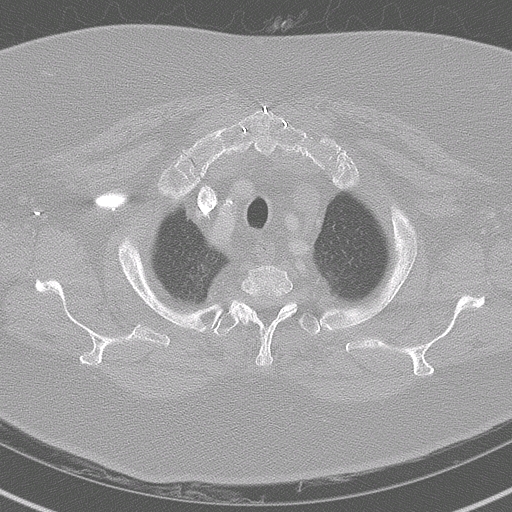
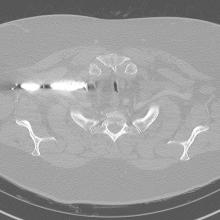
- Chest CT: narrowing involving the trachea at the level of the sternal notch extending over a length of 13 mm. The trachea measures 16 x 6 mm in maximum diameter at the narrowest part.
Note: Complicating factors of morbid obesity with underlying pulmonary abnormalities and sleep apnea warranted treatment with an open tracheotomy. In the absence of these comorbidities, other options could have possibly avoided a tracheotomy. Other options include tracheal resection or removal of anterior tracheal scar with interposition of tissue (strap muscles, sternocleidomastoid muscle). Endoscopic management was not felt to be a useful option due to the comorbidites above coupled with the soft lateral 'malacic' tracheal walls that readily accommodated a rigid dilator, but collapsed again on its removal.
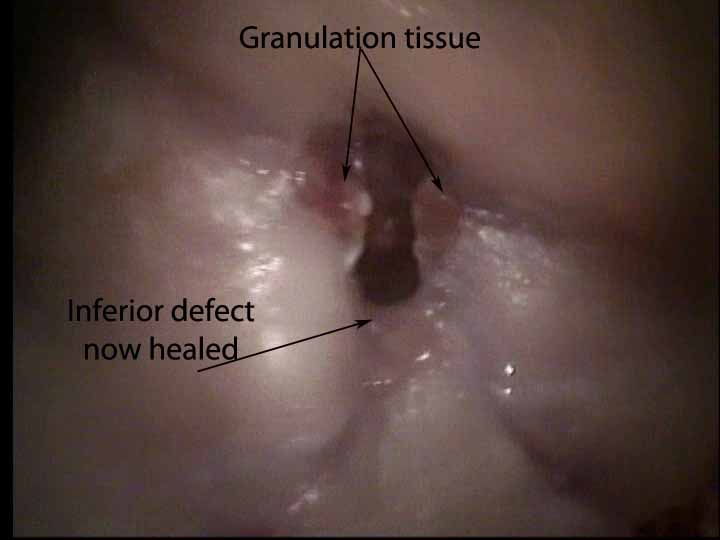
Initial appearance of intact healing was followed by breakdown of the inferior flap dealt with by outpatient packing twice daily with iodoform gauze.
 |
 |
 |
 |
|
Appearance 1 1/2 years postop |
|||
") |
 |
 |
") |
|
The Dedo laryngoscope is placed into the posterior glottis with the tip separating the posterior membranous vocal cords (jet anesthesia) |
Microdirect laryngoscopy with long 0 degree scope shows scarring anteriorly drawing lateral walls medially |
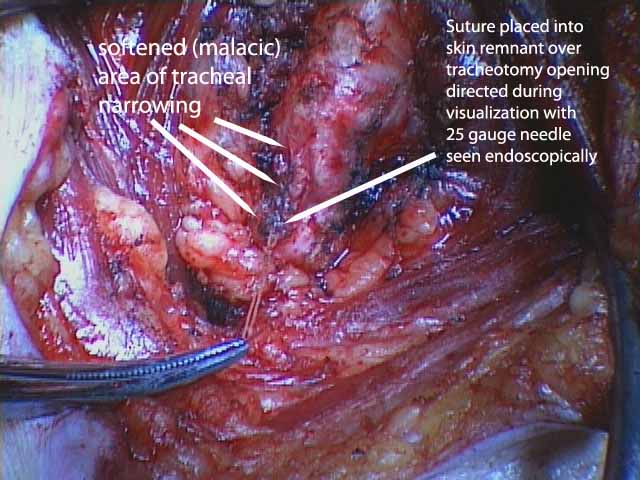
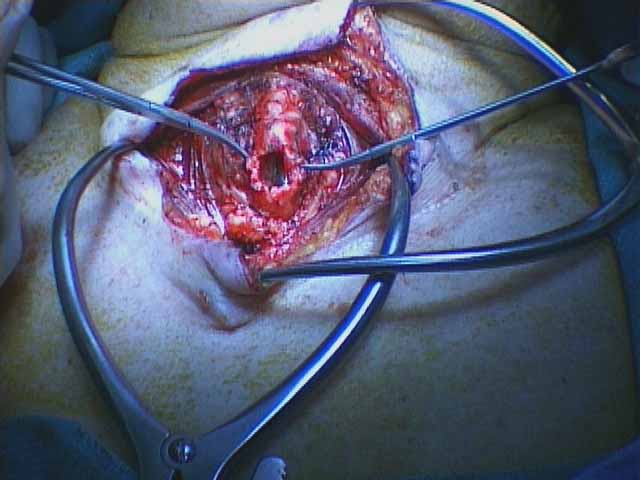
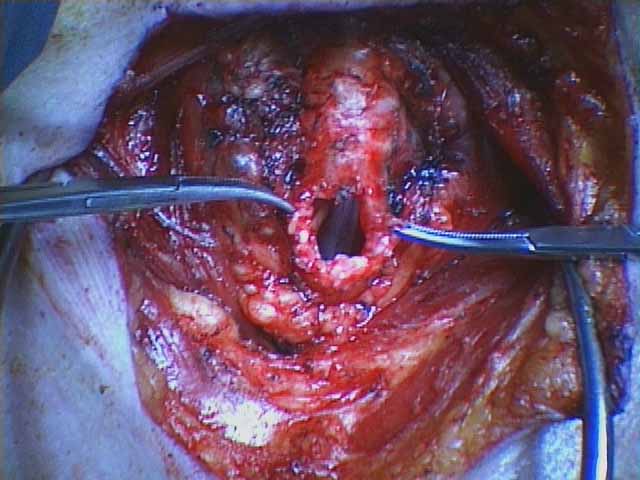
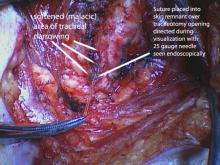
Appropriate site of entry into trachea for tracheotomy determined with 25 gauge needle placed percutaneously through previous tracheotomy site |
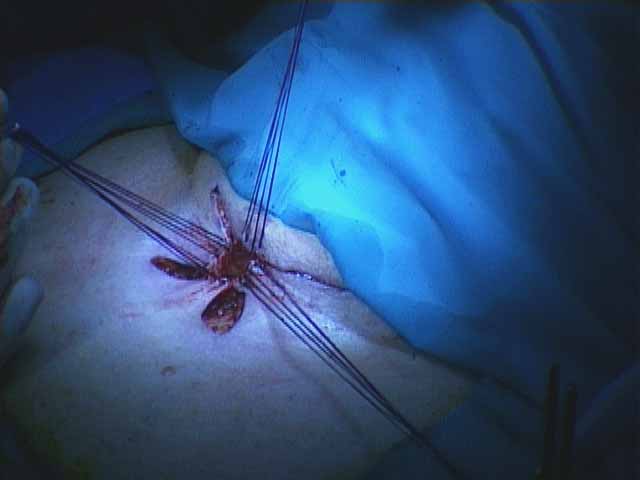
Four-flap epithelial lined tracheotomy outlined (with anterior cervical lipectomy and thyroid isthmusectomy) |
 |
") |
 |
 |
|
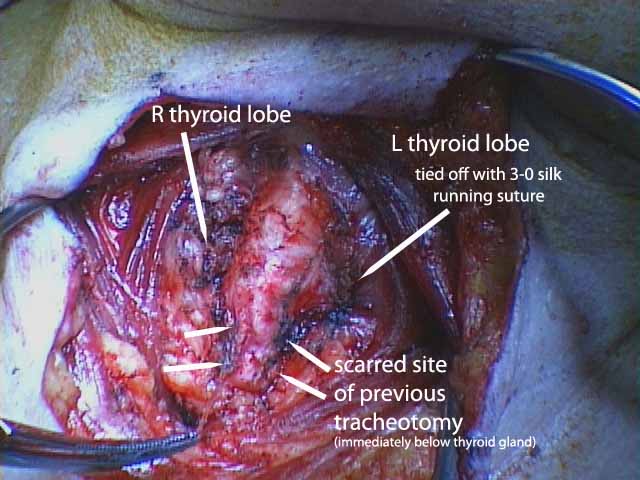
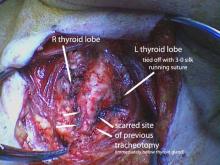
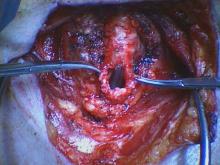
Two gelpy retractors used to identify large multinodular goiter after anterior cervical lipectomy accomplished along with midline separation of strap muscles |
A large portion of the midline thyroid is removed and sent for pathologic assessment (permanent section) |
||
 |
 |
 |
 |
 |
 |
 |
 |
|
Postoperative Day #5 at time of tracheotomy change from #6 cuffed Shiley to #6 metal Jackson |
With #6 metal cuffless Jackson tracheotomy good phonation achieved to be improved with use of Passey-Muir valve. |
||
 |
 |
 |
 |
|
POD #13 lower flap breakdown requiring iodoform gauze packing |
POD #13 |
POD #13 |
POD #13 |
 |
 |
 |
 |
|
POD #15 |
POD #15 |
POD #15 |
POD #15 |
 |
 |
 |
 |
|
POD #15 continued packing with iodoform gauze |
POD #15 |
POD #27 Packing no longer necessary |
POD #27 probe with qtip shows opening between skin and trachea now closed |
 |
 |
 |
 |
|
POD #27 |
POD #27 |
POD #64 |
POD #64 |
|
Followup 1 1/2 years postop |
References
Chang C and Thomas P: Adult-onset iatrogenic tracheomalacia. Ear,Nose & Throat Journal: June 2008, vol. 87 Issue 6, p312-313
Christenson TE, ARtz GJ, Goldhammer JE, Spiegel JR, and Boon MS: Tracheal Stenosis AFter Placement of Percutaenous Dilational Tracheotomy. Laryngoscope, 118:222-227,208
Law RC, Carney AS, Manara AR: Long-term outcome after percutaneous dilational tracheostomy: endoscopica nd psriometry findings. Anaeshtesia 1997;52: 51-56
Lulenski GC, Batsakis JG. Tracheal incision as a contributing factor to tracheal stenosis. An Experimental study. Ann Otol rhinol Laryngol 1975;84:781-786 (excellent study from the U of Michigan in animal model demonstrating stenosis similar to that above occurring after vertical incision for tracheotomy; scarring did not occur with an inferiorly based U-shaped flap. HH)
James P, Parmar S, Hussain K, Praveen P. Tracheal Stenosis after Tracheostomy. Br J Oral Maxillofac Surg. 2021 Jan;59(1):82-85. doi: 10.1016/j.bjoms.2020.08.036. Epub 2020 Aug 19. PMID: 33160732.