return to: Facial Fracture Management Handbook
by Dr. Gerry Funk
Lateral Orbital Wall Fractures
Anatomy and Mechanism of Injury
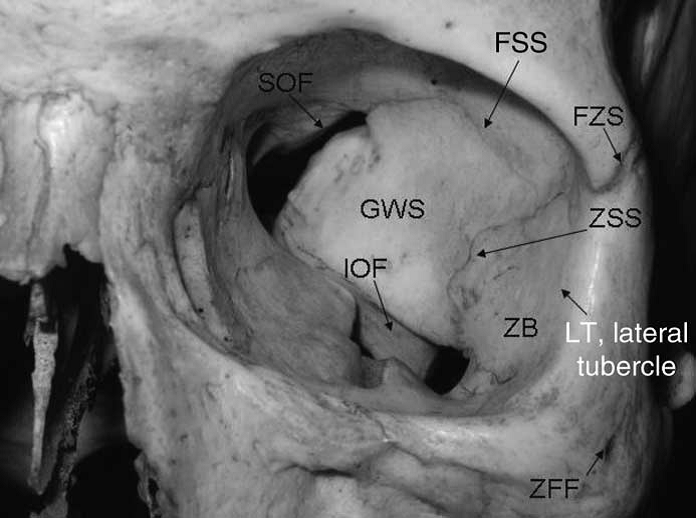
The lateral orbital wall is composed of the frontal process of the zygoma, the orbital plate of the greater wing of the sphenoid and the frontal bone. A small strut of lesser sphenoid wing forms the lateral orbital wall between the superior orbital fissure and the optic canal.

1 Foramen ethmoidale, 2 Canalis opticus, 3 Fissura orbitalis superior, 4 Fossa sacci lacrimalis, 5 Sulcus infraorbitalis, 6 Fissura orbitalis inferior, 7 Foramen infraorbitale
"Orbita mensch" by User:Uwe Gille - own work, copy from http://de.wikipedia.org/wiki/Bild:Orbita_mensch.jpg. Licensed under Creative Commons
{kind=link}
Attribution-Share Alike 3.0 via Wikimedia Commons - http://commons.wikimedia.org/wiki/File:Orbita_mensch.jpg#mediaviewer/Fil...
{kind=link}
The area of concern in lateral orbital wall fractures is primarily the orbital plate of the sphenoid. In axial section this bone is seen to make up the sphenotemporal buttress. Impact forces directed medially at the lateral orbital wall result in a medial impaction of the lateral orbital wall into the orbit and possibly into the orbital apex. This may result in compression of the contents of the superior orbital fissure and also the intraorbital portion of the optic nerve.
Physical Exam
Head and Neck exam with special attention to:
1. Visual acuity should be measured with a near card and the time of the exam recorded.
2. Documentation of extraocular movements, proptosis and ptosis.
3. Pupil reactivity and assessment for an APD should be carefully made.
4. Check the sensation in the cranial nerve V1 distribution.
Emergency Intervention
If visual acuity is decreased an Ophthalmology consult should be obtained emergently. Arrangements for an emergency CT of the orbits should be made. This should be a fine cut (no more than 2 mm) noncontrast bone and soft tissue CT. Both axial and coronal sections should be obtained. The sphenotemporal buttress is best seen on axial cuts. If an APD is present and visual acuity is decreased the patient should be started on high dose steroids (3/4 mg/kg initial dose and then 1/3 mg/kg every eight hours). These patients should be observed very closely for the first few hours. If the patient has useful vision, better than 20/400, a period of observation during the first 12 to 24 hours is reasonable. If vision is decreasing or is significantly worse than 20/400 surgery to disimpact bone fragments in the orbital apex should be considered.
Radiologic work up
This is part of the emergency management as described above. The CT scan is needed emergently to differentiate between cases where bone fragments, which may easily be reduced, are compressing the contents of the orbital apex and cases of intracanalicular optic nerve trauma with no obvious fracture fragment impingement on the optic nerve. The CT scan may also demonstrate fractures of the optic canal, indicating direct injury to the optic nerve at that location. This radiographic information will direct the acute management of the patient.
Definitive Management
This is a rare injury and there are no absolute management guidelines, often the decision to operate or watch and wait must depend on the judgment and experience of the head and neck surgeon and ophthalmologist managing the case. Improvements in vision have been reported in cases that underwent decompression several days following injury and spontaneous improvements in the superior orbital fissure syndrome component are reported up to several months following injury (Zachariades et al. 1985, Funk et al. 1989). If vision remains worse than 20/400, an APD is present, the CT demonstrates medially impacted lateral orbital wall fragments, external ophthalmoplegia is present and there has been no improvement with 24 hours of high dose steroids surgery in most cases is warranted. A progressive decrease in vision on high dose steroids or vision significantly worse than 20/600 argues in favor of decompression surgery. It should be recognized that this is not a decompression of the optic canal but rather of the orbital apex.
The surgical reduction of these fractures is through a lateral temporal approach. A hemicoronal incision is used to gain access to the lateral orbital wall. An anterior approach is not used in order to avoid any retraction of the orbital contents. After exposure of the lateral orbital wall and sphenotemporal buttress through the hemicoronal incision the medially impacted fragments are gently mobilized laterally. Patients are covered with steroids following the surgery for 24 hours and then tapered pending the clinical response. A postoperative CT scan should be obtained to ensure that the medially impacted fragments have been disimpacted laterally (Funk et al. 1989).
References
Zachariades,N., Vairakzaris,E., Papavassiliou,I., et al: The superior orbital fissure syndrome. J. Maxillofac. Surg. 13: 125-128, 1985.
Funk,G.F., Stanley,R.B., Becker,T.S.: Reversible visual loss due to impacted lateral orbital wall fractures. Head & Neck 11: 295-300, 1989.