

Click on image above to enlarge; advance with cursor over border
return to: Trachea Surgical Protocols
see: Case Example Tracheal Stenosis after Tracheotomy with Four Flap Epithelial Lined Tracheotomy; Use of Tracheostomy Tube Cuff; Case Example Four-flap Epithelial Lined Tracheotomy (delayed healing process)
see another: Four flap epithelial lined tracheotomy with thyroid isthmusectomy and anterior cervical lipectomy - Clinical case example (slow, but more normal healing process aided with dilute betadine solution applications)
GENERAL CONSIDERATIONS
- Indications: Need for tracheotomy in patients with
- Anticipated need for long term tracheotomy
- Severe obstructive sleep apnea
- Other
- Obesity with thick neck
- To increase safety by easing replacement of the tracheotomy tube
- To maintain a clean tracheostome and decrease granulation formation
- Anticipated need for long term tracheotomy
- Contraindications
- Situations where endotracheal intubation can be easily achieved and can be used to stabilize the airway; the airway obstruction may be short-lived, and a tracheotomy may be avoided (selected cases of epiglottitis, angioneurotic edema of the airway).
- Relative contraindication is an uncontrolled coagulopathy.
- Situations where a conventional tracheotomy would be more appropriate.
PREOPERATIVE PREPARATION
- Emergent Cases
- The patient may need to undergo either awake fiberoptic intubation or awake tracheotomy.
- Cricothyrotomy under local anesthesia may be done through skin incisions targeted to be extending to into conversion into a four-flap epithelial lined tracheotomy (see case example)
- Perform in operating suite, if possible.
- If emergent cricothyroidotomy is performed, patient should be taken to the operating room once stabilized. This allows for revision of the tracheotomy and performance of direct laryngoscopy to assess for any laryngeal or tracheal injury.
- The cervical spine should be cleared or appropriately stabilized in all trauma cases.
- Planned Procedures
- Provide preoperative tracheotomy care teaching to patient and/or care provider.
- Assess patient's neck anatomy with attention to landmarks and presence of significant submental fat.
- Assess patient's body habitus and possible need for customized operating room table.
- Consent
- The patient should be consented for an epithelial-lined tracheostomy, anterior cervical lipectomy, thyroid isthmusectomy, and possible direct laryngoscopy.
- It should be emphasized to the patient that there is a higher likelihood (compared to conventional tracheotomy) of the need for another procedure to close the tracheostomy should the patient no longer require it.
- Explain the need for establishment of alternate airway to the patient.
- Describe the surgical technique
- If an awake tracheotomy is to be done, explain to the patient about talking/interactions between health care givers during the procedure.
- Explain that the patient will not be able to talk after the tube has been placed with the balloon inflated.
- Describe complications
- Bleeding, infection
- Scar formation
- Tracheal stenosis
- Accidental decannulation
- Pneumothorax/pneumomediastinum
- Injury to surrounding structures (esophagus, recurrent laryngeal nerve, major vessels)
- Tracheocutaneous fistula
- Post obstructive pulmonary edema association with concurrent diagnosis of obstructive sleep apnea
- Morbid obesity is associated with increased risk of tracheostomy complications, most due to postoperative displacement of tracheostomy tube
NURSING CONSIDERATIONS
- Room Setup
- See Basic Soft Tissue Room Setup
a. Use ENT supply pack instead of the Basic soft tissue pack - Table positioned with head toward anesthesiologist; may need to alter this if tracheotomy is being performed as part of another head and neck procedure.
- Head of bed should be elevated to 70o. A footboard for the operating room table is necessary to help the patient support their body weight.
- See Basic Soft Tissue Room Setup
- Instrumentation and Equipment
- Standard
- Special
- Syringe, Luer tip, 10/12 cc, disposable
- Medications (specific to nursing)
- 1% lidocaine with 1:100,000 epinephrine
- 4% lidocaine, plain
- Prep and Drape
- Standard prep, 10% providone iodine
- Drape
- Head drape
- Towels to square off incision site on neck, from chin to chest, from shoulder to shoulder
- Drape off mouth, either for anesthesia access to the endotracheal tube or to allow easy breathing by an awake patient
- Split sheet
- Drains and Dressings
- 2x 0.25"Penrose Drains
- 2x Sterile Rubber Bands
- Suture needed: 3.0 silk, vicryl and nylon. 4.0 chromic.
- Special Considerations
- Have a variety of types and sizes of trachs available. In particular, trachs with extra-long proximal or distal extensions may be necessary in patients with very thick necks.
- Test cuff on trach tube with 5 cc of air and place in cup of water. If bubbles are seen, the tube is faulty.
- Moisten tube with saline before giving to surgeon to insert.
- Be sure obturator is taped to patient's chest or shoulder before patient leaves the room.
- In very rare circumstances it may be reasonable to suture flanges of tracheotomy tube to skin to keep it in place. However, these sutures cause scarring and, most importantly, inhibit placement of drain sponges with the targeted 3-4 x per day dilute betadine care. Ideally will have made the tracheostome safe by suturing skin flaps to mucosa and cartilage in a manner to make tracheotomy placement safe and easy. Usually secure only with velcro trach straps.
- For revision of existing tracheostoma to a four flap epithelial lined tracheastoma, it is advisable to intubate from above whenever possible prior to initiating the procedure.
ANESTHESIA CONSIDERATIONS
- Be prepared for awake fiberoptic intubation, if indicated.
- indications: history of difficult airway or potential for difficult airway. Examples include OBESITY/OSA, trauma, deep neck space infection, tumors, history of radiation, congenital airway anomalies, cannot access cricothyroid membrane, cervical spine instability.
- Must have easy access to tube to allow removal at time of entry into trachea.
- Sterile tubing may be needed, depending on timing and order of tracheotomy relative to other procedures.
- In awake tracheotomy, IV sedation should be utilized with caution so as not to depress respiratory drive.
- Communication with anesthesia is of paramount importance. They should be aware of operative procedure points "15" and "18" below.
- In order to facilitate communication at our institution, the protocol for proposed procedure is emailed prior to procedure. Alternatively, a paper copy can be brought to OR room.
OPERATIVE PROCEDURE
- Table positioned with head toward anesthesiologist; may need to alter this if tracheotomy is being performed as part of another head and neck procedure.
- Head of bed should be elevated to 70o. A footboard for the operating room table is necessary to help the patient support their body weight.
- Ensure the patient is at the head to the bed to permit extension without shoulder role (do not place shoulder roll) - ensure bed is appropriate for the patients weight.
- Landmarks should be palpated: thyroid notch, cricoid, and suprasternal notch.
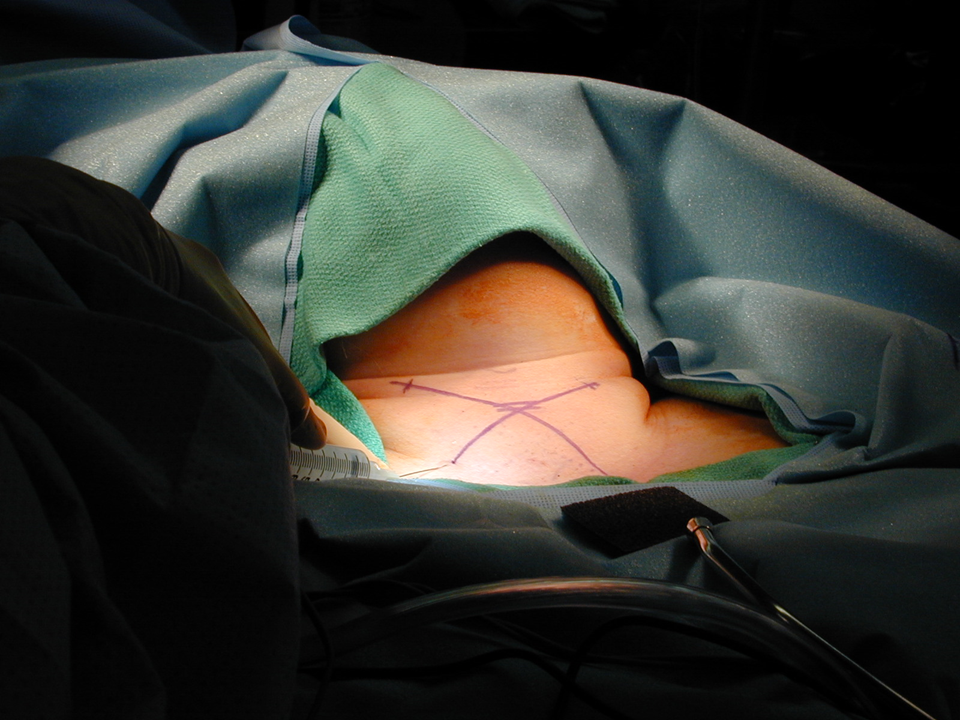
- Planned incision site should be marked and injected with 1% lidocaine with 1:100,000 epinephrine.
- A X-shaped incision made with the convergence of the limbs centered over the patient's cricoid cartilage. Each of the limbs should be approximately 6-8cm in length in order to achieve appropriate flap length.
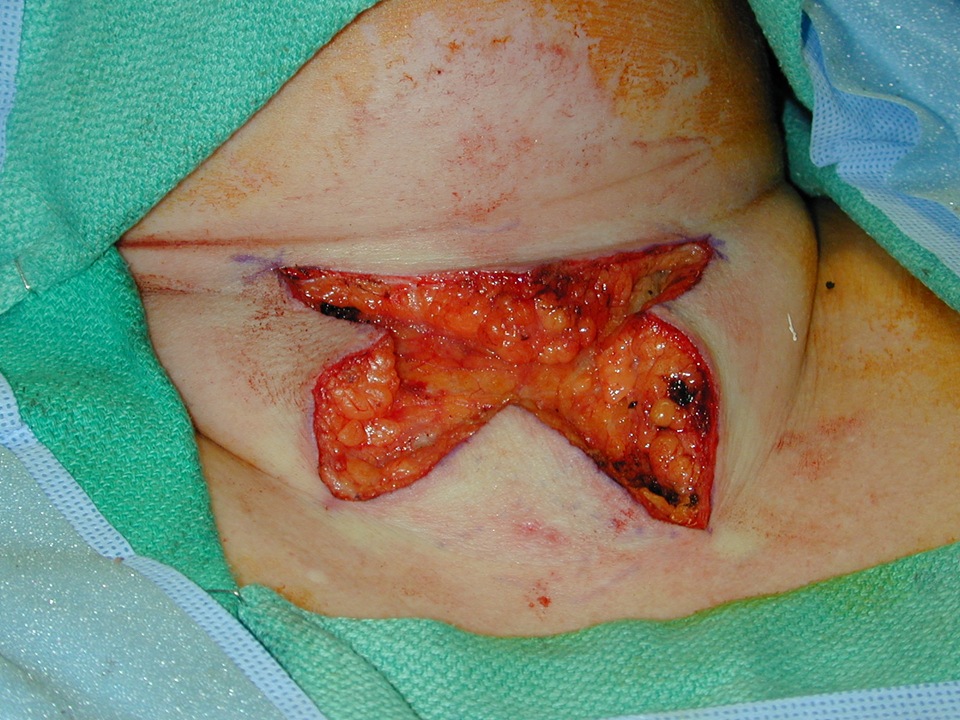
- Dissection is carried down through subcutaneous tissues with monopolar cautery.
- Each of the four limbs of the X are elevated individually and "defatted". The apex should be thinned to the level of the dermis with a thin layer of adipose tissue remaining on the rest of the flap. This helps to ensure flap viability. Blood vessels from the muscle to the overlying skin are not true musculocutaneous perforators, and the muscle does not have a true axial blood supply. The muscle and overlying skin receive blood from a variety of sources including the submental artery, branches of the proximal facial artery, postauricular artery, occipital artery, terminal cutaneous branches of the superior thyroid artery, superficial cervical artery, and transverse cervical artery.
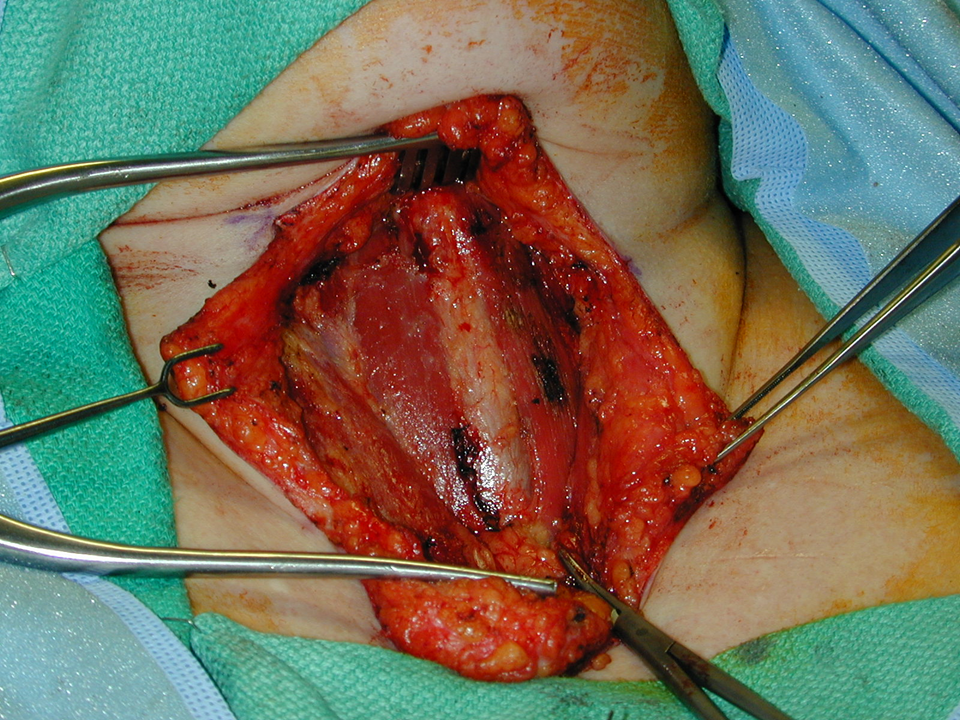
- The anterior cervical lipectomy is then performed with monopolar cautery through supra and sub-platysmal fat until the strap muscles are exposed.
- Anterior jugular veins can be retracted laterally or ligated, if necessary.
- Once the strap muscles are identified, they are divided by a combination of electrocautery and blunt dissection through the median raphe and retracted laterally.
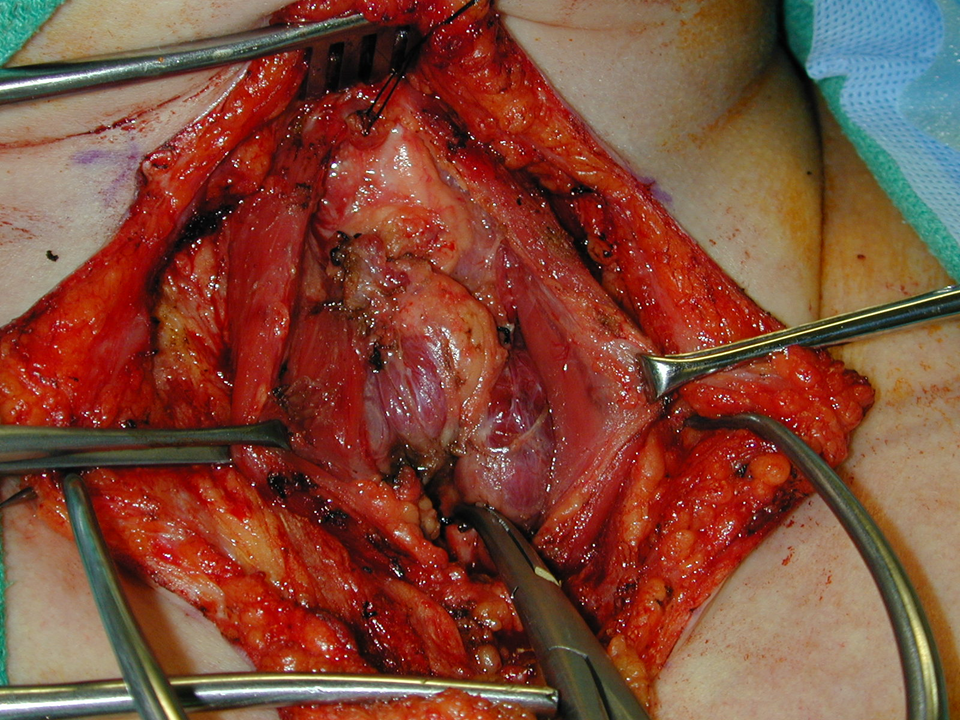
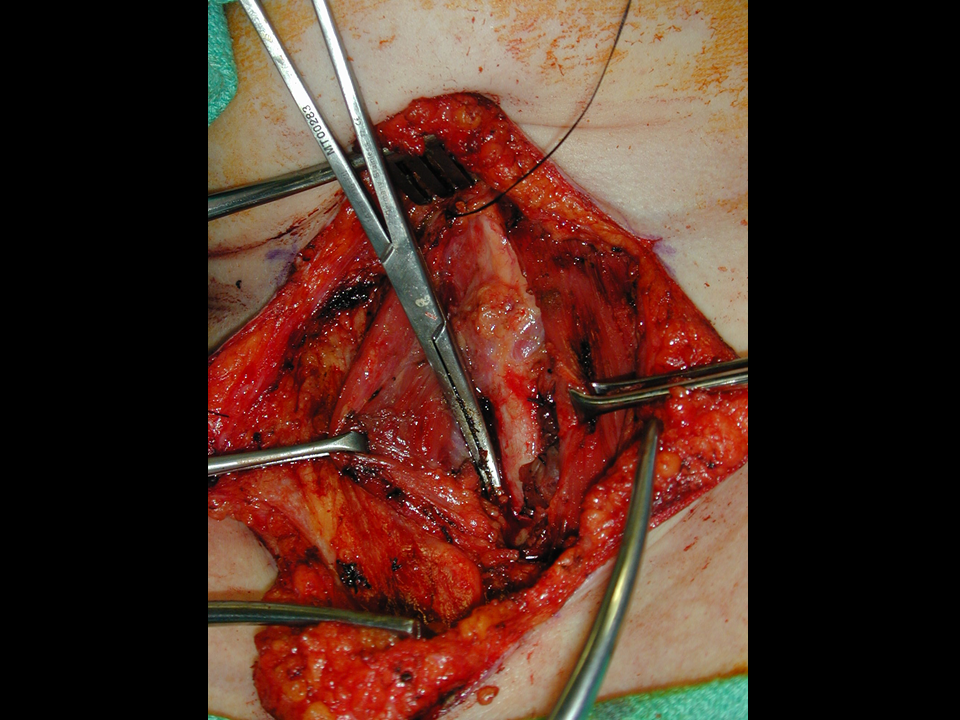
- The thyroid isthmus is then encountered. This should be dissected free from the underlying trachea and surrounding soft tissue.
- A formal thyroid isthmusectomy is then performed. A hemostat is used to clamp on the medial aspect of the right and left thyroid lobes, respectively after creating a tunnel by hemostat dissection between the gland and the underlying tracheal wall with care not to perforate into airway. The thyroid is then divided along the hemostat with monopolar cautery. The edges are then tied off with a running "baseball" suture of 3-0 silk.
- Once the anterior tracheal wall is identified, overlying soft tissue can be cleaned off the surface with Kitners.
- Entry into the trachea can now be performed - usually between the second and third tracheal rings. Alert the anesthesiologist, so that s/he may be prepared to remove the endotracheal tube when necessary. Entry into the trachea should be controlled, with an attempt made to avoid injury to the underlying endotracheal tube cuff, especially in the critically ill patient. One method of preventing injury to the endotracheal tube cuff is to have the anesthesiologist advance the tube 4 to 5 cm before entry into the trachea (''mainstem the tube') - usually most safely done through a membranous area between the rings with the tip of a small hemostat with extension laterally with a #15 (not #11) blade (done to ensure no puncture of the cuff of the tube.
- Superiorly and inferiorly-based Bjork flaps are then made by making parallel vertical cuts laterally through the second and third tracheal rings. Some surgeons prefer to perform a tracheal window which also works.
- Once the tracheal entry site is secured, the endotracheal tube is replaced back from where it had been 'mainstemmed' so the cuff is below the opened trach site.
- Once the trachea has been entered, any cauterization should be limited to use of the bipolar, not unipolar and be done with care. In an oxygen-rich field, an airway fire could result. If cauterization for hemostasis is necessary, the FiO2 of the inhalational agents should be lowered.
- The superior and inferior apices of the flaps should then be squared off to allow approximation to the Bjork flaps. The four flaps should then be examined to see if they will fit to the margin of the tracheostomy without excessive tension. If not, additional "defatting" of the flaps may be necessary.
- The superior and inferior skin flaps should then be sutured to the Bjork flaps with 3-0 or 4-0 Vicryl suture. There should be 3 sutures per flap with care taken to include the deep layer of cartilage (not mucosa) and superficial perichondrium as well as only the dermis of the skin flap.
- It may be necessary to suture the thyroid lobes laterally to the sternocleidomastoid muscle for retraction in order to allow the lateral skin flaps to be sutured to the tracheostomy. This should be done with a 3-0 Vicryl suture.
- The lateral skin flaps should be sutured to the edges of the tracheostomy in a similar manner to the superior and inferior flaps.
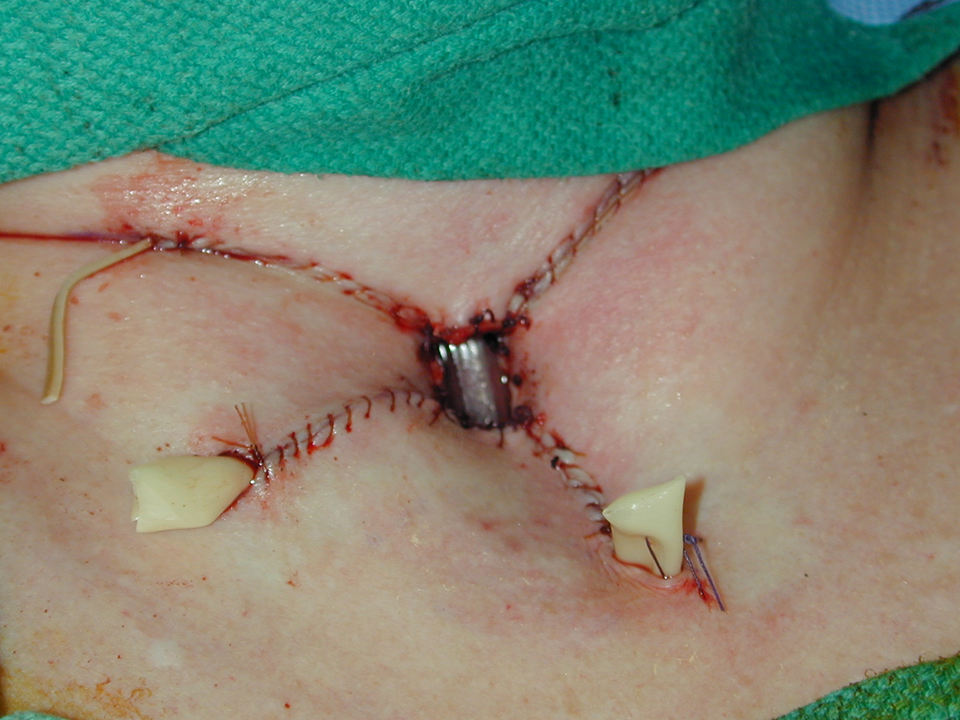
- The dermis of the incisions should then be reapproximated with 3-0 Vicryl sutures. It may be necessary to eliminate the dead space by incorporating strap muscles into the suture bite. The skin is closed with 4-0 Chromic Gut in a running fashion. The edges of the tracheostomy should similarly be closed with a running 4-0 Chromic Gut suture.
- . A 0.25" Penrose drain should be placed through the lateral aspect of each inferior incision and sutured in place with 3-0 nylon. A sterile rubber band should be placed through the lateral aspect of each superior incision and sutured in place with 3-0 nylon. Under certain circumstances, some surgeons do not place drains into the wound bed.
- The tracheostomy tube with obturator should then be placed. In most circumstances, use of the tracheal dilator for insertion is not necessary. The obturator is then removed, and an inner cannula is placed. The endotracheal tube is then removed. Placement of the tube should be confirmed by watching for CO2 return on the anesthesia monitor and/or auscultation of the lungs.
- The tracheotomy tube is then secured in place with tracheal ties. A drain sponge is then pulled around the tube with a hemostat. The tracheotomy incision is left open to avoid subcutaneous emphysema.
POSTOPERATIVE CARE
- A drain sponge should be placed around the tube to collect secretions.
- A dilute betadine-soaked drain sponge should be placed around the tube for 10 minutes twice daily and then replaced with a clean drain sponge.
- The cuff should be deflated after 24 hours in nonventilated patients.
- Drains may be removed, if there is not excessive drainage, by postoperative day 2 or 3.
- First tracheotomy change done on postoperative day 5.
- Tracheostomy care should be taught again to patient prior to discharge (see Tracheostomy Home Care Booklet Protocol).
- With significant weight loss or reversal of other medical problems, removal of the tracheotomy tube may permit spontaneous closure.
- A persistent tracheocutaneous fistula may result and can be closed as per protocol: Tracheocutaneous fistula closure
- One the tract is mature and if the patient is neither dependent on the tracheotomy for an airway nor dependent on mechanical ventilation may be a candidate for a Montgomery Canula.
REFERENCES
Lore JM. The trachea and mediastinum: tracheostomy. In: Atlas of Head and Neck Surgery. 3rd ed. Philadelphia, Pa: WB Saunders Co; 1988:811-818.
Wenig BL, Applebaum EL. Indications for and technique of tracheotomy. Clin Chest Med. 1991;1293:545-553.
Gross ND, Cohen JL, Anderson PE, Wax MK. Defatting Tracheostomy In Morbidly Obese Patients. Laryngoscope. 2002 Nov; 112 (11): 1940-4.