
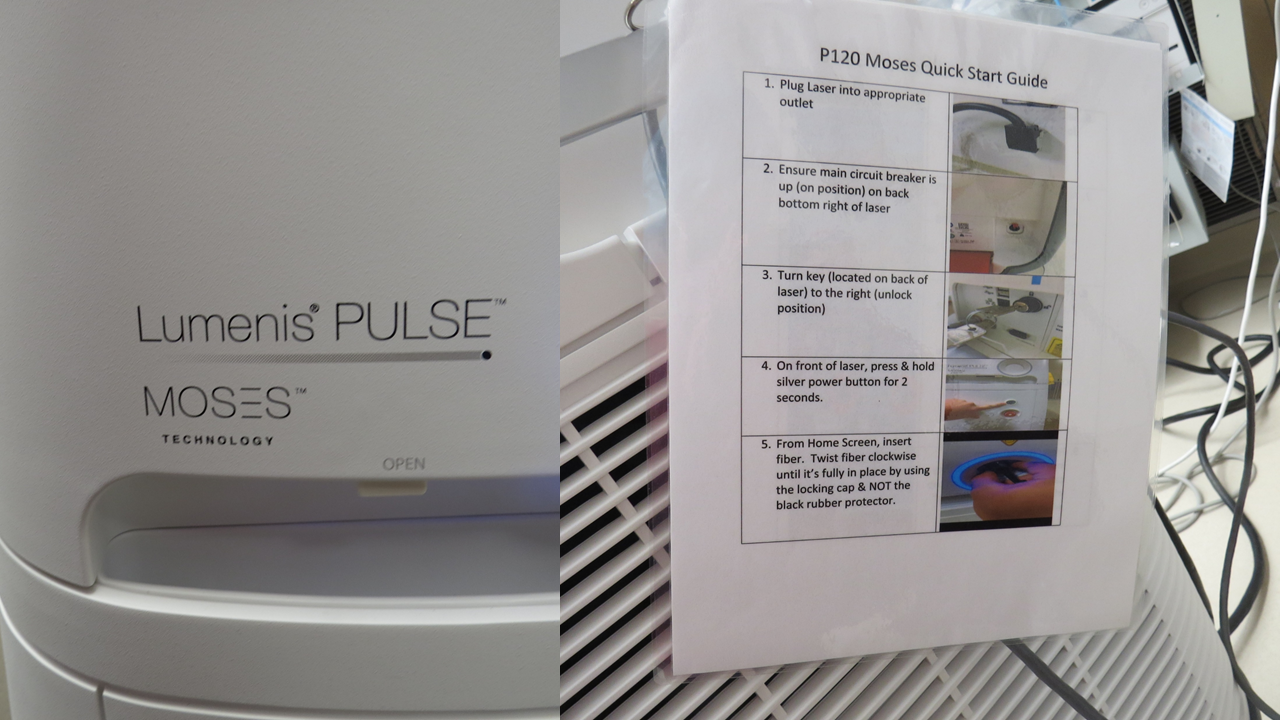
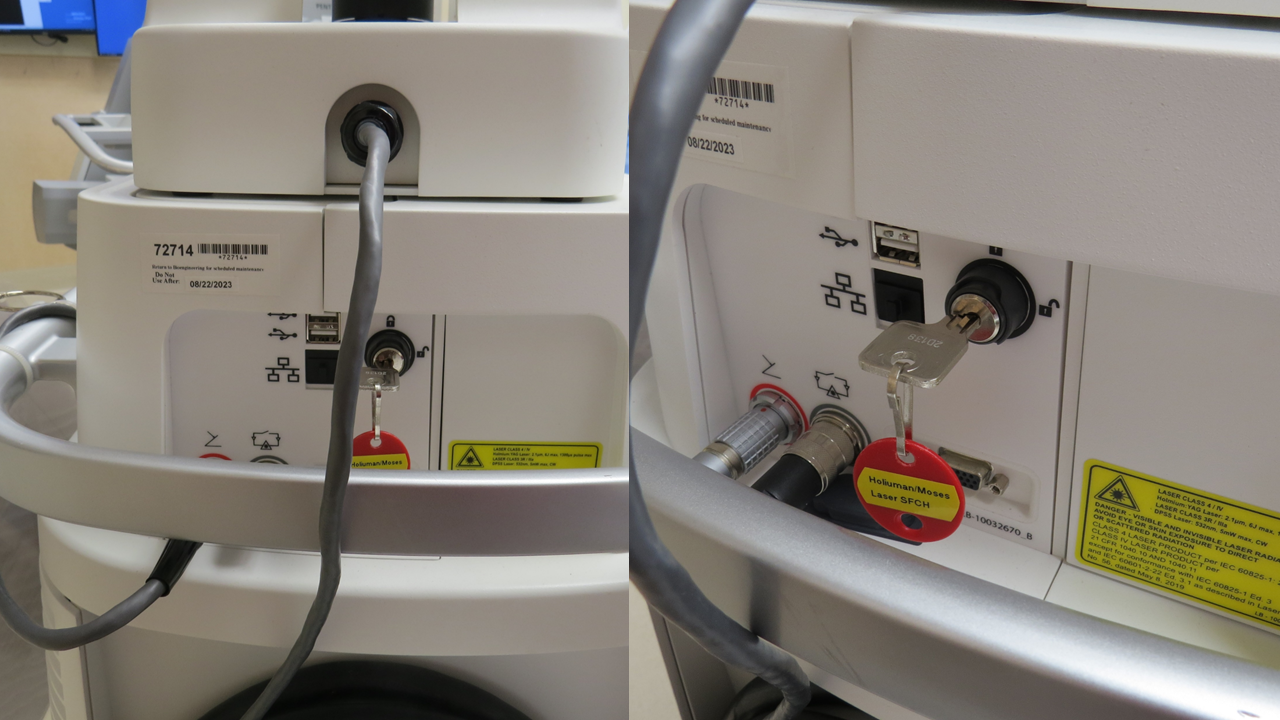
return to: Sialendoscopy or Laser Surgery Protocols; Sialendoscopy Room Set Up and Equipment for Submandibular Glands
Background
The first medical laser lithotripsy papers appeared in 1985 with development dominated by Urologic applications with the majority of articles addressing endoscopic laser lithotripsy continuing from the field of Urology.
Holmium lasers have dominated the field of lithotripsy (Kronenberg 2015)
- Wavelength of 2,100 nm is almost completely absorbed by water within 0.4 mm of the laser fiber tip
- Intensity adjustable (pulse energy, pulse frequency): Total Power (Watts) = Pulse energy (Joules) x Pulse frequency (Hz - cycles per second)
- Pulse energy most important factor determining ablation volume (pulse frequency and total power less important role)
- Short-pulse mode more ablative than long-pulse mode
- Harder stone material more difficult to ablate than softer stone material
The fibers used to deliver Holmium laser energy are important - with studies identifying tip degradation (Mues 2009)
Tissue effects of holmium laser:
- Concern regarding laser damage to the adjacent salivary gland duct warranted Schrötzlmair et al (2015) to evaluate a fresh excised section of submandibular duct tissue (in vitro) exposed to Ho:YAG laser in single pulse mode with energies of 0.5,1.0 and 1.5 J per pulse through a 200µm fiber with 'near contact light' - with histologic examination identifying no tissue damage observed at 0.5J per pulse but higher energies of 1.0 and 1.5J per pulse creating a circumscribed hole in the mucosa. Through similar in vitro analysis they identified adequate fragmentation of submandibular salivary stones with 500mJ (0.5J) per pulse was adequate without appreciated improvement in ablation at higher energies. They appropriately defer to clinical series to deteremine whether use of the Ho-YAG laser at 0.5J (500mJ) is "sufficient for complete stone fragmenation in vivo at a tolerable duration of surgery" see:
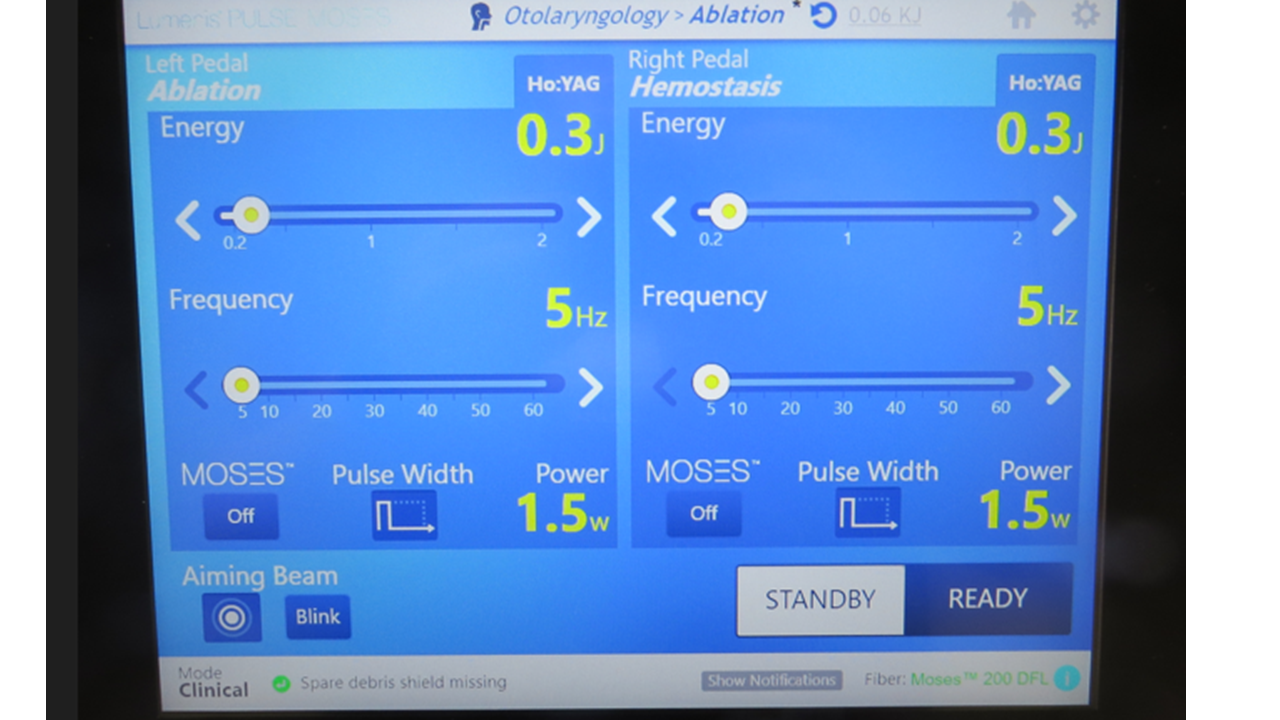
Laser Settings (Holmium)
Koch et al (Koch 2019) reported retrospective study of 87 stones in 66 patients treated at two institutions (12 stones - 50% submandibular in Erlangen, Germany; 75 stones 86.7% submandibular in Taipei, Taiwan) identified success in complete fragmentation of all treated stones leading to recommended settings:
Ho:YAG laser - 3 to 4.8 Watts, frequency of 3-6 Hz, energy level of 0.5 to 1.2 Joules
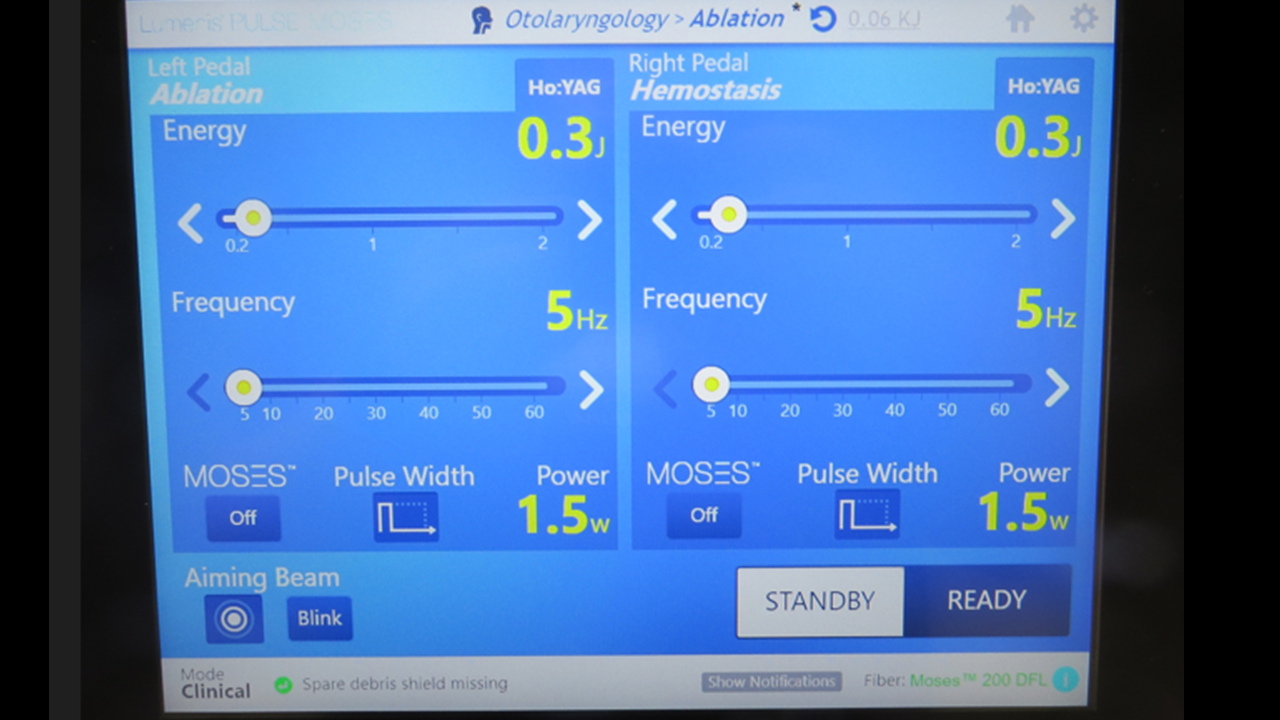
Ho:YAG laser setting: Frequency, Power, Energy
Koch et al (Koch 2019): 3-6 Hz (cps), 3-4.8 Watts, 0.5-1.2 Joules
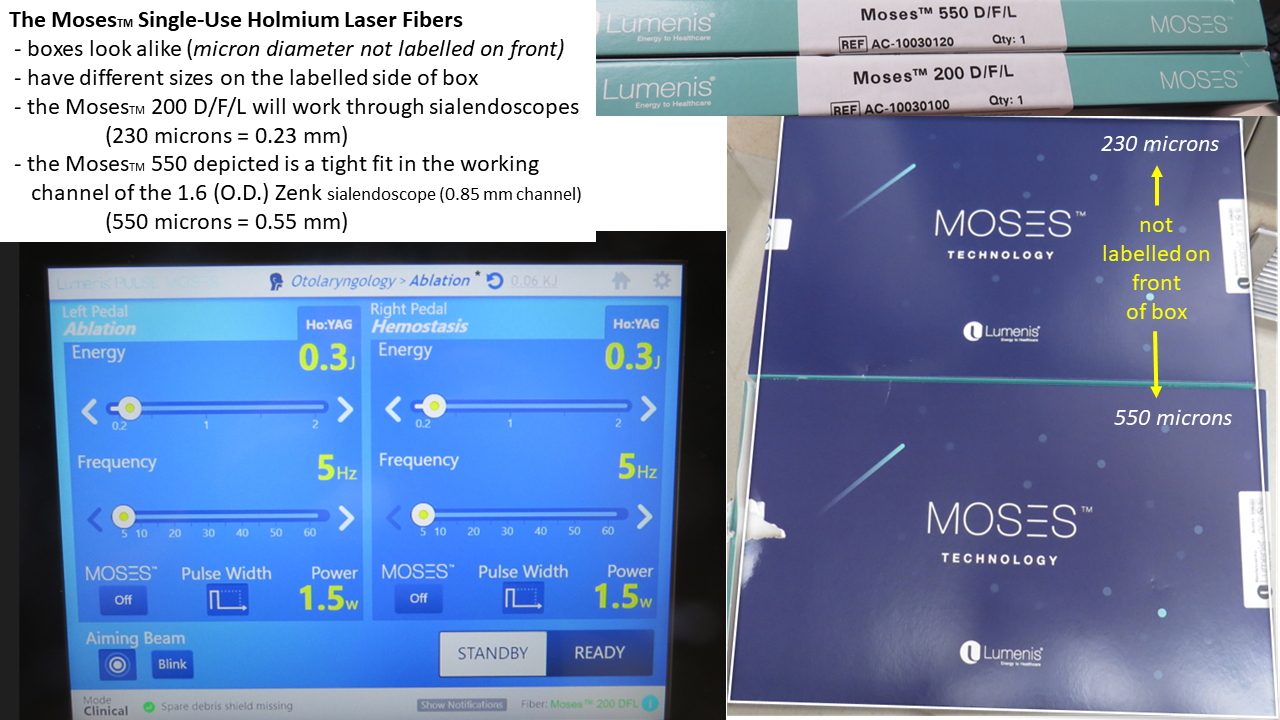
Other recommended settings 5 1.5 Watts

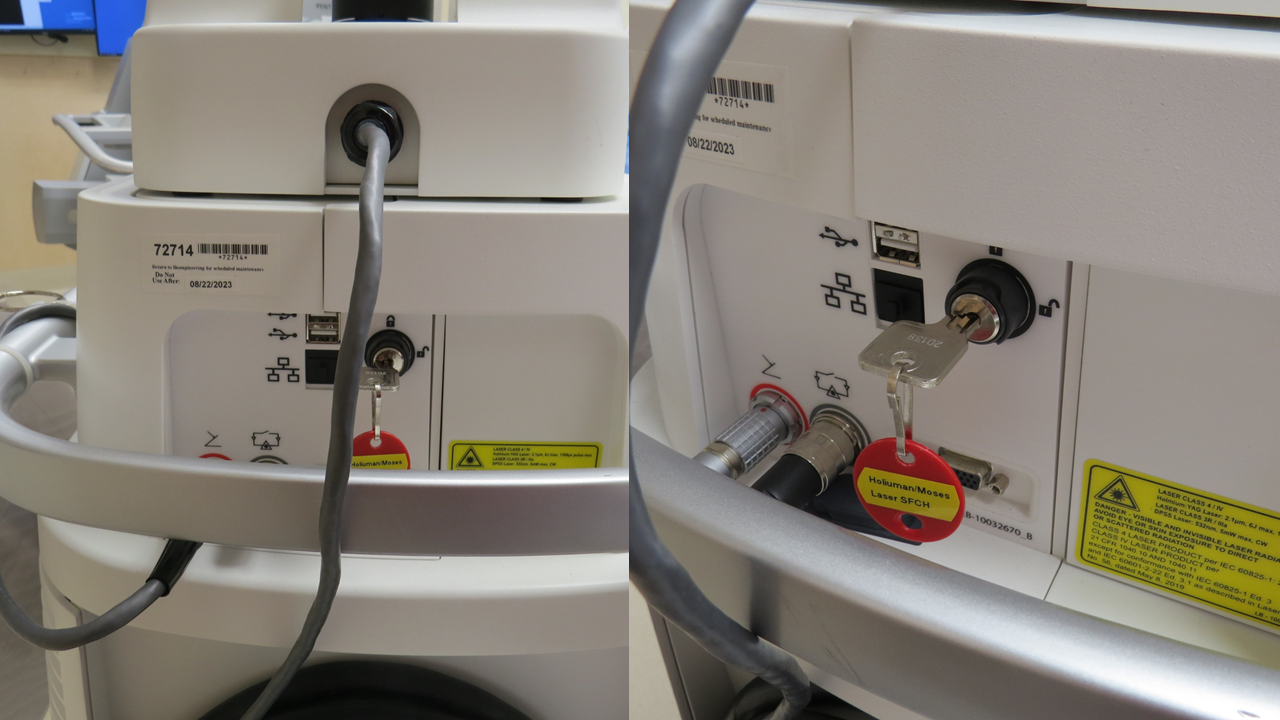
newer laser:
Definitions
Watt (W) = a unit of power. One watt is equal to one joule per second (1 J/sec) or 1 kg-m2.s-3 and is used to quantify the rate of energy transfer
Joule (J) = a unit of energy. One watt-second is equal to one joule. (Wikipedia contributors "Watt" 2023)
Power is a physical quantity distinct from Energy. Power is the amount of energy transferred per unit time.
References
Kronenberg P and Traxer O: Update on lasers in urology 2014: current assessment on holmium:ytterium-aluminum-garnet (Ho:YAG) laser lithotripter settings and laser fibers
Mues AC, Teichman JMH, Knudsen BE: Quantification of holmium:yttrium aluminum garnet optical tip degradation. J Endourol 23(9):1425-1428
Knudsen BE, Pedro R, Hinck B et al (2011) Durability of reusable homium: YAG laser fibers: a multicenter study. J Urol 185(1):160-163
Pierre S, Preminger GM: Holmium laser for stone management World J Urol 2007 June;25(3):235-9
Koch M, Hung Sh, Su CH, Lee KS, Iro H, and Mantsopoulos K: Intraductal lithotripsy in sialolithiasis with two different Ho:YAG lasers: presetting parameters, effectivenss, success rates Eur Rev Me Pahmacol Sci, 2019 Jul:23(13):5548-5557.
Schrötzlmair F, Müller M, Pongratz T, Eder M, Johnson T, Vogeser M, von Holzschuher V, Zengel P, Sroka R. Laser lithotripsy of salivary stones: Correlation with physical and radiological parameters. Lasers Surg Med. 2015 Apr;47(4):342-9. doi: 10.1002/lsm.22333. Epub 2015 Mar 18. PMID: 25788338.
Wikipedia contributors, "Watt," Wikipedia, The Free Encyclopedia, https://en.wikipedia.org/w/index.php?title=Watt&oldid=1192253276 (accessed December 29, 2023).
Additional references (obtained from Dr. Witt - modified from Chapter 22 Laser Fragmentation of Salivary Stones ( Author: Robert A. Irvine) in Book: Surgery of the Salivary Glands Publisher (Editor Robert L Witt) : Elsevier Date: 2021
Extracorporeal and intracorporeal lithotripsy of salivary gland stones: basic investigations. Zenk J; Koch M; Iro H. Otolaryngologic Clinics of North America. 42(6):1115-37, Table of Contents, 2009 Dec.
Laser lithotripsy of salivary stones: Correlation with physical and radiological parameters. Schrotzlmair F; Muller M; Pongratz T; Eder M; Johnson T; Vogeser M; von Holzschuher V; Zengel P; Sroka R. Lasers in Surgery & Medicine. 47(4):342-9, 2015 Apr.
Ho:Yag laser for sialolithiasis of Wharton's duct. Martellucci S; Pagliuca G; de Vincentiis M; Greco A; Fusconi M; De Virgilio A; Gallipoli C; Gallo A. Otolaryngology - Head & Neck Surgery. 148(5):770-4, 2013 May.
Sialendoscopy with holmium:YAG laser treatment for multiple large sialolithiases of the Wharton duct: a case report and literature review. Sun YT; Lee KS; Hung SH; Su CH. Journal of Oral & Maxillofacial Surgery. 72(12):2491-6, 2014 Dec.
A serious complication of laser lithotripsy. Sahin-Yilmaz A; Oysu C. Journal of Oral & Maxillofacial Surgery. 73(5):798-9, 2015 May.
Sialoendoscopy with and without holmium:YAG laser-assisted lithotripsy in the management of obstructive sialadenitis of major salivary glands.[Erratum appears in Br J Oral Maxillofac Surg. 2014 Jul;52(6):579] Sionis S; Caria RA; Trucas M; Brennan PA; Puxeddu R. British Journal of Oral & Maxillofacial Surgery. 52(1):58-62, 2014 Jan
Sialendoscopy for salivary stones: principles, technical skills and therapeutic experience. F. Carta, P. Farneti, S.Cantore, G. Macri, N. Chuchueva, L. Cuffaro, E. Pasquini, R. Pudexxu Acta Otorhinolaryngologica Italica 2017;37:102-112
Salivary lithotripsy in the era of sialendoscopy. [Review] Capaccio P; Torretta S; Pignataro L; Koch M. Acta Otorhinolaryngologica Italica. 37(2):113-121, 2017 Apr
Thulium-YAG laser sialendoscopy for parotid and submandibular sialolithiasis. Durbec M; Dinkel E; Vigier S; Disant F; Marchal F; Faure F.
Lasers in Surgery & Medicine. 44(10):783-6, 2012 Dec
Sialendoscope-assisted trans oral removal of hilo-parenchymal and sub-mandibular stones: surgical results and subjective scores. Capaccio, P, Gaffuri, M, Rossi, V, Pignataro, L, Acta Otorhinolaryngologica Italica 2017; 37:122-127.
Optimal Power Settings for Holmium:YAG Lithotripsy. Jason Sea, Lee M Jonat, Ben H. Chew, Jinze Qiu, Binqing Wang, John Hoopman, Thomas Milner and Joel M. H. Teichman, J. Urology 187; 914-9, March 2012