

click on image above to enlarge, advance with cursor over border
see also: Local Anesthesia for Rigid Endoscopy
return to: Laryngeal Surgery (Benign Disease) Protocols
Note: last updated before 2013
GENERAL CONSIDERATIONS
- Indications
- Symptomatic glottic insufficiency
- Laryngeal paralysis or laryngeal paresis in patient whom recovery of vocal cord mobility is uncertain .
- Glottic insufficiency with mobile vocal folds (ie, presbylaryngis)
- Symptoms
- Dysphonia
- Dysphagia
- Poor cough
- Symptomatic glottic insufficiency
- Contraindications
- Inability to perform direct laryngoscopy
- Unstable cervical spine
- Unable to obtain exposure of the larynx (ie, retrognathic)
- May consider other approaches
- Percutaneous injection through cricothyroid membrane
- Transoral injection employing indirect mirror exposure of larynx
- Inability to perform direct laryngoscopy
PREOPERATIVE PREPARATION
- Evaluation
- Essential for most cases
- Speech pathology assessment (see Laryngeal diagnostics protocol)
- Videolaryngoscopy with voice recording (see Videostroboscopy protocol)
- Consider for selected cases
- Trial of voice therapy
- Laryngeal electromyography (see Laryngeal EMG (Electromyography) protocol)
- Offer to patient with history of neck arthritis or neck surgery/injury: Lateral neck radiographs in flexion and extension.
- Offer to most patients with dentition: Dental prosthetics evaluation preoperatively to fashion a tailored (custom made) acrylic dental splint
- To prevent dental injury more effectively than the standard plastic "gump".
- To patients with difficult exposure in whom the acrylic guard will permit a greater degree of force applied to dentition through "fulcrum laryngoscopy" (see suggested reading "Dental Protection During Rigid Endoscopy").
- Essential for most cases
- Consent
- Describe procedure and expected recovery
- Laryngeal fat injection is designed to medialize the paralyzed vocal cord and can be used either alone or in combination with another medialization procedure, such as arytenoid adduction.
- Identify that the fate of injected fat is uncertain. Although studies have suggested it may persist for many years, others believe it usually resorbs after 6 months. Repeated injections may be required to maintain adequate vocal fold medialization.
- Identify that voice quality will evolve after fat placement. The best voice may not occur immediately postoperative because of deliberate overinjection, but rather some time later in the postoperative period.
- Potential complications
- Bleeding, infection, reaction to anesthetic
- Damage to adjacent structures
- Lips, teeth, tongue, larynx from direct laryngoscopy
- Hoarseness, airway obstruction, continued dysphagia with aspiration
- Hematoma or infection at the abdominal site for fat harvest
- Describe procedure and expected recovery
NURSING CONSIDERATIONS
- Room Setup
- Instrumentation and Equipment
- Medications (specific to nursing)
- Antibiotic ointment
- 1% lidocaine with 1:100,000 epinephrine (to inject periumbilical for fat harvest)
- 4% lidocaine
- Prep and Drape
- Prep
- Prep to abdomen in periumbilical region and towels to square off for harvesting the fat
- Drape
- Medium sheet above and below harvest site
- Split sheet around harvest site
- Head drape oriented to protect taped eyes
- Cloth drape across chest
- Prep
- Drains and Dressings
- Adaptic
- Fluffs
- Elastoplast tape
- Rubber gand or 1/4 in Penrose drain
- Special Considerations
- Bruening syringe with 18-gauge or 19-gauge needle with a backup syringe in case of malfunction
- Laryngoscopes
- Dedo and Storz laryngoscopes are most commonly used.
- Hollinger anterior commissure laryngoscope may be used with difficult exposure of the larynx.
- Preservative-free sterile saline used to rinse fat prior to injection.
- 4% lidocaine in syringe with 25-gauge needle to apply topically to laryngeal surface through laryngoscope after fat injection to reduce chance of laryngospasm.
ANESTHETIC CONSIDERATIONS
- General Anesthesia
- Communication with anesthesia essential
- Oral endotracheal intubation with small (5.5 to 6.0) endotracheal tube (MLT tube = micro-laryngeal/tracheal tube)
- Short-term paralysis (estimate 5-minute case)
- Consideration for alternative methods
- . Jet anesthesia
- . Apnea
- . Local anesthesia with sedation (see Local Anesthesia for Rigid Endoscopy protocol)
- Communication with anesthesia essential
- Preoperative Systemic Medications
- Glycopyrrolate 0.1 to 0.2 mg IM on call to operating room
- The drying effect improves exposure; consider avoiding in patients with xerostomia.
- The vagolytic effect diminishes the risk of laryngospasm.
- Consider Decadron 8 to 10 mg IV when IV started to diminish edema.
- Contraindications: diabetes, ulcer disease, other
- Anti-staphylococcal antibiotics preoperatively and for 5 days postoperatively.
- Glycopyrrolate 0.1 to 0.2 mg IM on call to operating room
- Positioning
- May be done with head toward anesthesia or rotated 90°.
- Head of bed elevated 15 to 30° neck extended with head in sniffing position.
OPERATIVE PROCEDURE
- Fat Harvest (without liposuction)
- Inject 1% xylocaine with 1:100,000 epinephrine to the umbilicus and laterally to one side.
- Incise from 12:00 to 6:00 on one side of the inner aspect of the umbilicus to avoid causing a visible scar.
- Fat is removed with forceps, scalpel, and scissors.
- Electrocautery is not used until all fat is harvested.
- The abdominal incision is closed with subcuticular 4-0 vicryl to avoid need for suture removal.
- A rubber band or Penrose drain may be needed if dissection is extensive or bloody.
- A pressure dressing is applied employing Elastoplast.
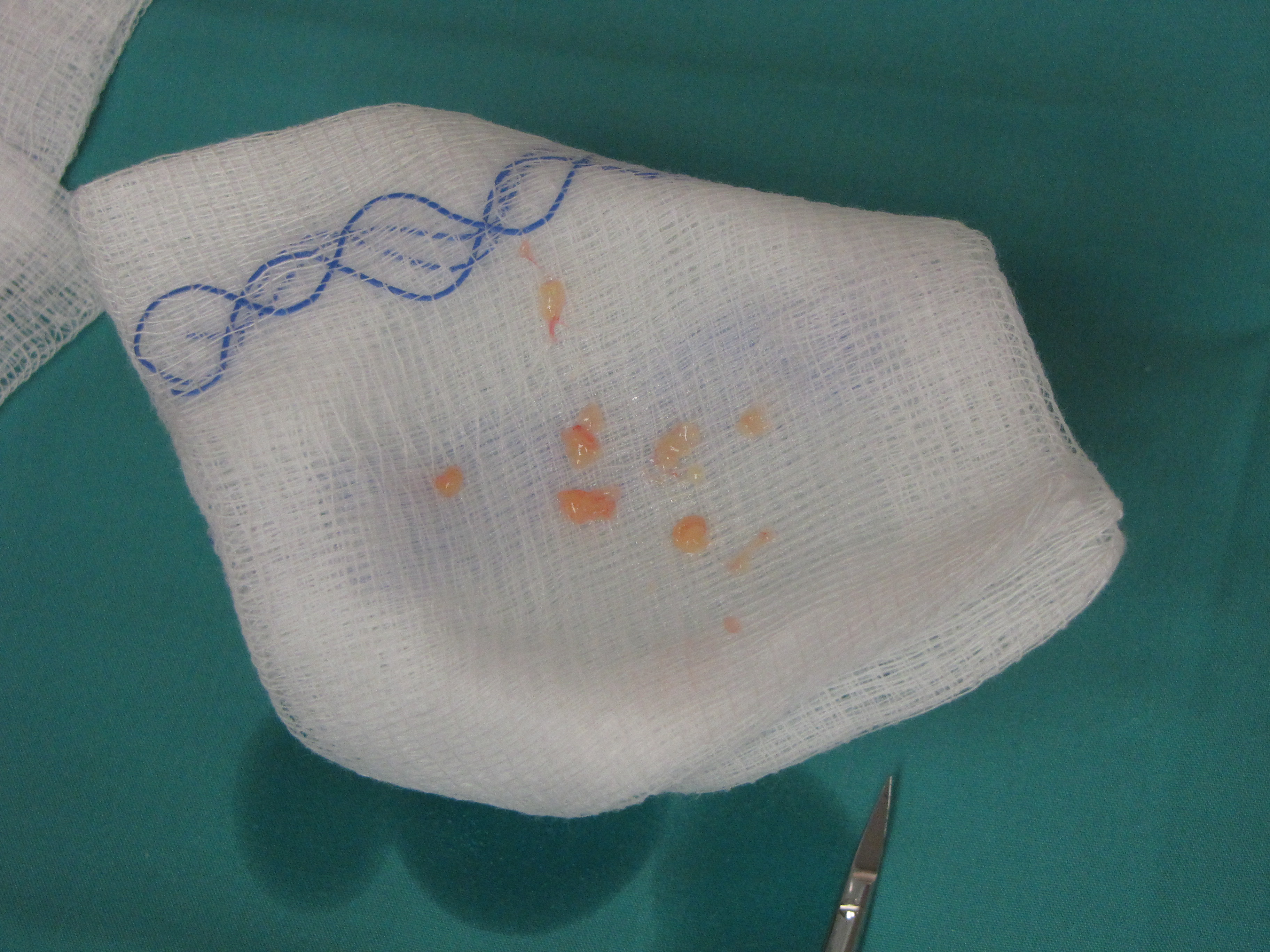
- Fat is minced with small scissors into 1 to 2 mm cubes, copiously irrigated with saline and loaded into the barrel of the Bruening syringe.
- If the procedure is being performed under local anesthesia, topical and infiltrative anesthesia is applied, and the sedated patient is appropriately monitored.
- A stab incision is marked adjacent to the umbilicus and injected with 1% xylocaine with 1:100,000 epinephrine.
- The surgical field is infiltrated using 0.5% xylocaine with 1:200,000 epinephrine. A 15.5-gauge liposuction cannula is selected. The cannula is connected to a suction "trap" for harvesting of the abdominal fat. The fat is obtained using conventional liposuction techniques with attention to avoiding injury to the dermis.
- The abdominal stab incision is closed and a pressure adhesive dressing placed on the abdomen.
- The fat is atraumatically placed on a gauze swab and gently cleaned with copious saline irrigation. It is then transferred to a Bruening syringe. The handle of the Bruening syringe is advanced until fat is just coming out of the syringe tip (19-gauge needle).
- Fat Injection (direct laryngoscopy)
- May be performed under local anesthesia (see Local Anesthesia for Rigid Endoscopy protocol). There is little benefit derived from injection under local anesthesia when general anesthesia can be employed. Purposeful overinjection is performed, hence a good phonatory result following injection is not the endpoint. As a result, we now rarely perform this procedure under local anesthesia.
- Fat injection is performed through an 18-gauge or 19-gauge Bruening syringe needle.
- The location for fat injection may vary according to the indications for vocal fold augmentation. For most cases of glottic incompetence due to laryngeal paralysis, the injection is performed laterally into the paraglottic space. The fat characteristically diffuses from the site of injection to involve areas not specifically targeted. Due to the consistency of the fat, this feature of lipoinjection is generally not a problem.
- The vocal fold is deliberately overmedialized by up to 50% to allow for subsequent absorption of fat.
- Fat Injection (percutaneous with transnasal flexible fiberoptic laryngoscopy guidance)
- A 19-gauge needle is the smallest bore we use to inject fat due both to concerns regarding trauma to fat by use of a smaller needle and the technical difficulty in passing fat through a smaller needle. As a result, injection through the mucosa of the vocal fold necessarily creates a large hole through which the injected fat may extrude. Precise placement of injected fat is more difficult by the percutaneous method, but does instill the fat deeply through a longer tract that helps to prevent extrusion. Due to the "forgiving" nature of injected fat, absolutely accurate placement (as is critical with Teflon injection) has not been necessary in our hands. The experience gained with percutaneous EMG-guided Botox injection to the thyroarytenoid muscles has permitted us to use this same approach (without EMG guidance) for laryngeal fat injection.
- The nose is decongested with pontocaine and epinephrine topically applied. One percent lidocaine with 1:100,000 epinephrine is injected into the skin overlying the cricothyroid membrane.
- A "stab" incision is made with a #15 scalpel over the cricothyroid membrane to accommodate the 19-gauge needle (without depth marker) of the Bruening syringe. A spinal needle (18- gaugeor 19-gauge) introduced with its stylet in place offers the advantage of improved ease of insertion without accumulation of debris in the open needle tip. Removal of the stylet permits placement of a 1 cc syringe loaded with fat for injection. Larger syringes generally do not permit adequate delivery of the fat through the spiral needle. Alternatively, in patients with thick necks, a small incision may be made with separation of the strap muscles in the midline to permit accurate placement of the syringe through the cricothyroid membrane.
- The television monitor (attached to the camera recording images from the flexible nasopharyngoscope) is positioned at the patient's head to permit the surgeon to view deformation of the vocal fold during needle placement to assess its position. The needle is placed 2 mm lateral to the midline and advanced through the cricothyroid membrane supero-lateral in a submucosal fashion without entering the airway. Movement of the needle is identified by the recorded image seen on the television screen. Once needle placement is verified, fat is injected to result in as much medialization as is safe for the airway (generally 50% overinjected). Some resorption is expected. Reinjection may be necessary.
POSTOPERATIVE CARE
- The procedure is usually done as an outpatient
- If there is any question about adequacy of the airway, plan overnight observation in hospital (23-hour stay).
- Consider evaluating larynx with indirect mirror examination or flexible fiberoptic laryngoscope before discharge.
- Begin oral feedings when alert
- If dysphagia with aspiration was an important component of the symptoms preoperatively, consider evaluating with a "cookie swallow" (OPMS) before feeding.
- Continue oral antibiotics for 5 to 7 days.
- Voice rest
- Absolute for 48 hours
- Relative for 2 weeks: Employ "arm's length rule" wherein the patient does not address a person unless they are within an arm's length away.
- Follow-up individualized based on symptoms
- If dysphagia is a significant component, consider "cookie swallow" on postoperative day 1.
- If voice is the only concern, then follow-up in 2 weeks; with videostroboscopic exam 6 weeks postoperatively.
REFERENCES
Bauer CA, Valentino J, Hoffman HT. Long-term result of vocal cord augmentation with autogenous fat. Ann Otol Rhinol Laryngol. 1995;104:871-874.
Hoffman H. Review of Brandenburg et al. Vocal cord injection with autogenous fat: a long-term magnetic resonance imaging evaluation. In Laryngoscope. 1996;106:174-180. Otolaryngology J Club. 1996;3:255-258.
Hoffman HT, McCulloch TM. Anatomic considerations in the surgical treatment of unilateral laryngeal paralysis. Head Neck. 1996;18:174-187.
Olsen GT, Moreano EH, Arcuri MR, Hoffman H.T. Dental protection during rigid endoscopy. Laryngoscope. 1995;105:662-663.
McCulloch TM, Andrews BT, Hoffman HT, Graham SM, Karnell MP and Minnick C:Long-term follow-up of fat inje tion laryngoplasty for unilateral vocal cord paralysis. Laryngoscope 2002 Jul;112(7 Pt 1):1235-8