See also: Nose Bleed Management and Epistaxis Control
Epistaxis; Nosebleed - Epistaxis: Anterior Ethmoid Artery Ligation (External - Open Approach)
Initiated by Caleb Escudero and Dr. Xiaoyang Hua 8-28-2023
Background
- Sphenopalatine artery (SPA) ligation can be considered in cases of recurrent posterior epistaxis refractory to conservative measures (Pop 2023). Compared to anterior epistaxis, patients with posterior epistaxis are at increased risk of prolonged hospitalizations (Supriya 2010). Conservative management in the form of posterior nasal packing is often attempted, but surgical hemostasis has been shown to reduce the risk of rebleeding (Soyka 2011). Hemostasis can be obtained with embolization by interventional radiology, but SPA ligation has been reported to have fewer complications (de Bonnecaze 2018).
- Whereas surgeons in the past advocated for an open transantral approach to ligate the SPA (usually with microscopic control), endoscopic ligature has become more popular since its first report in 1992 (Budrovich 1992). Endoscopic transnasal approaches are preferred by many surgeons, but some utilize transseptal or transantral approaches (El-Guindy 1998).
Anatomy
- The SPA is the terminal branch of the internal maxillary artery, which is an extension of the external carotid artery. The SPA leaves the pterygopalatine fossa through the sphenopalatine foramen (SPF) to enter the nasal cavity and supply the posterior nasal septum and lateral nasal wall (Pothier 2005). Although most commonly there are two branches of the SPA exiting the SPF, the pattern is variable and up to 10 branches can be seen (Prades 2008). Additionally, some patients have been found to have 2-3 foramen.
- The SPF is located on the lateral nasal wall, and is classically found at the transition between the middle and superior meatus (Prades 2008). However, some studies report the SPF is more often found in the superior meatus (Scanavine 2009). Due to the variability in its location, an important surgical landmark is the crista ethmoidalis (CE) of the palatine bone which is located within 1 mm of the SPF (Flint 2014). The distal tip of the CE has been shown to point towards the inferior margin of the SPF (Scanavine 2009).
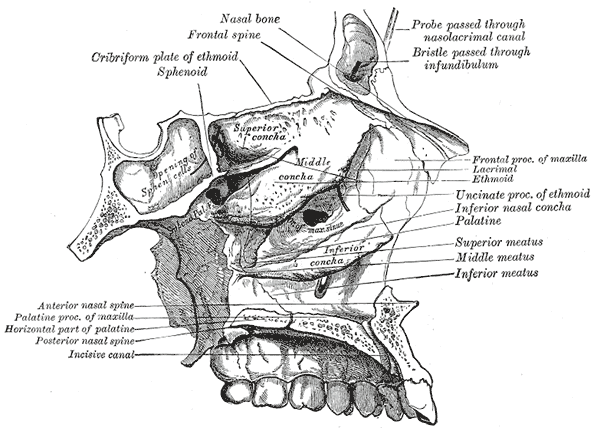
Gray, Henry. Anatomy of the Human Body. 20th edition, 1918. Plate 196. Lea and Febiger, pub. Philidelphia. Public Domain image. Accessed (open access) from https://commons.wikimedia.org/wiki/File:Gray196.png
{kind=link}
Preoperative Preparation
- Consent/Risks
- Rebleeding and nasal dryness
- Nasal septum, inferior turbinate necrosis
- Injury to V2
- CSF leak (Kishimoto 2018)
- Medications
- 1% lidocaine with epinephrine 1:100,000
- Afrin
- Floseal
- Nasopore or surgicel
- Equipment
- Endoscopy tower
- Bipolar
- Cottle elevator
- Kerrison punch
- Ball tipped maxillary sinus seeker
- Nasal Endoscopy Room Setup
- Place pieces of cotton with a topical vasoconstrictor into the nasal cavity 5 minutes before the start of the procedure.
- Turn the bed 180 degrees.
- Tuck patient arms at side.
- Some surgeons place the patient in reverse trendelenburg with at least 15 degrees of elevation to reduce mucosal bleeding.
- Prep and drape the surgical area.
Operative Procedure
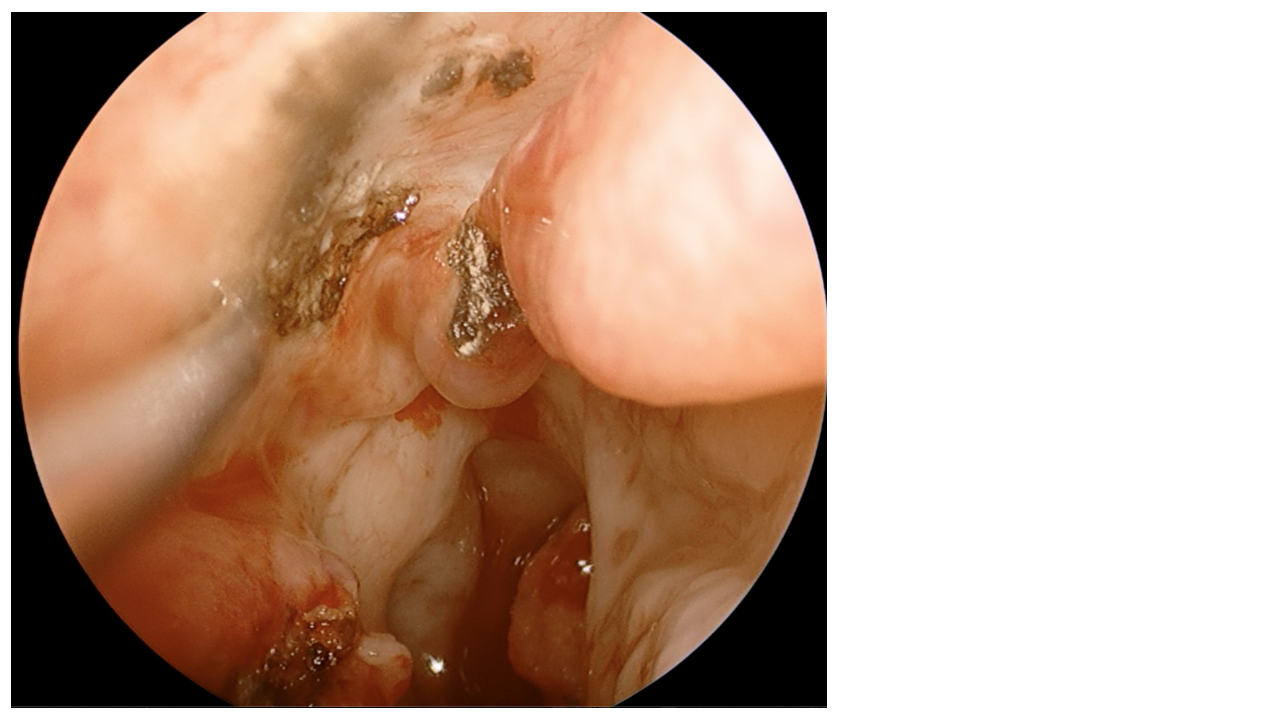
- Remove any nasal packing present and utilize 0° endoscope to remove any visible blood clots.
- Apply 1% lidocaine with epinephrine (1:100,000) to the lateral nasal wall at the level of the middle turbinate insertion and uncinate process. Some surgeons prefer a transoral greater palatine foramen injection.
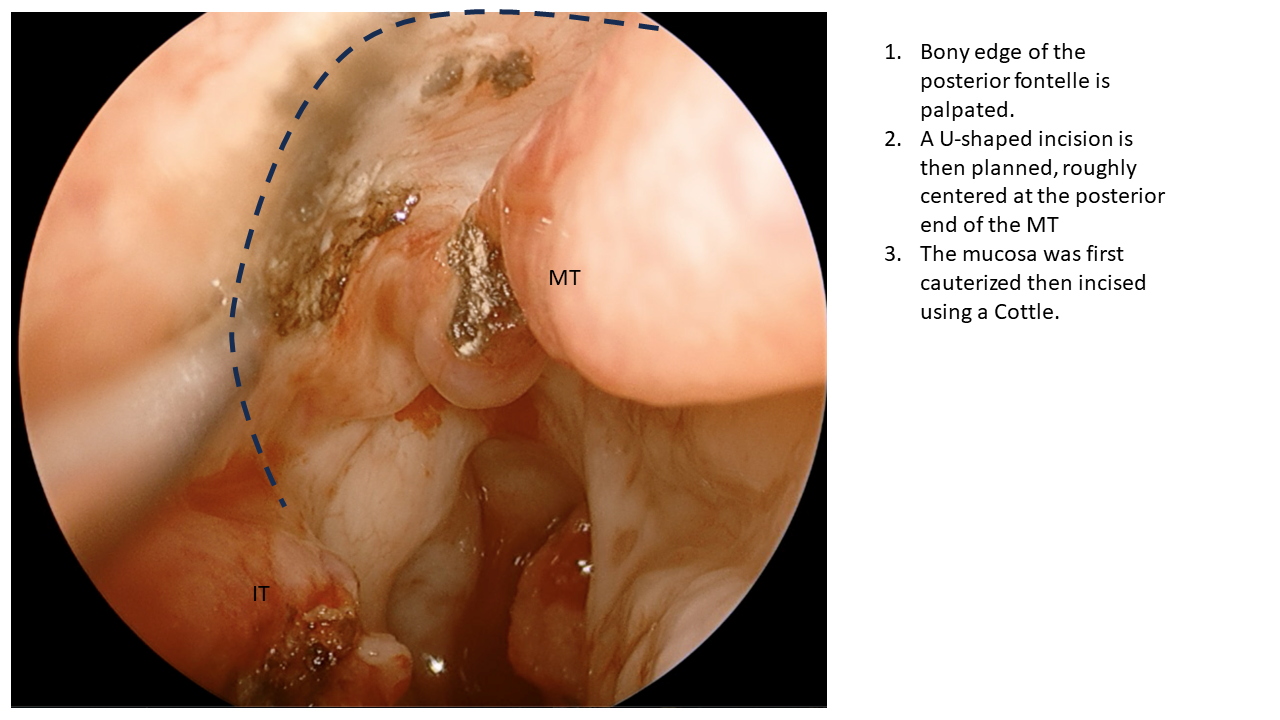
- Identify and palpate the bony edge of the posterior fontelle.
- Plan a U-shaped incision centered at the posterior middle turbinate. Some surgeons prefer to create an antrostomy.
- Cauterize the mucosa with the bipolar, then incise using a Cottle elevator.
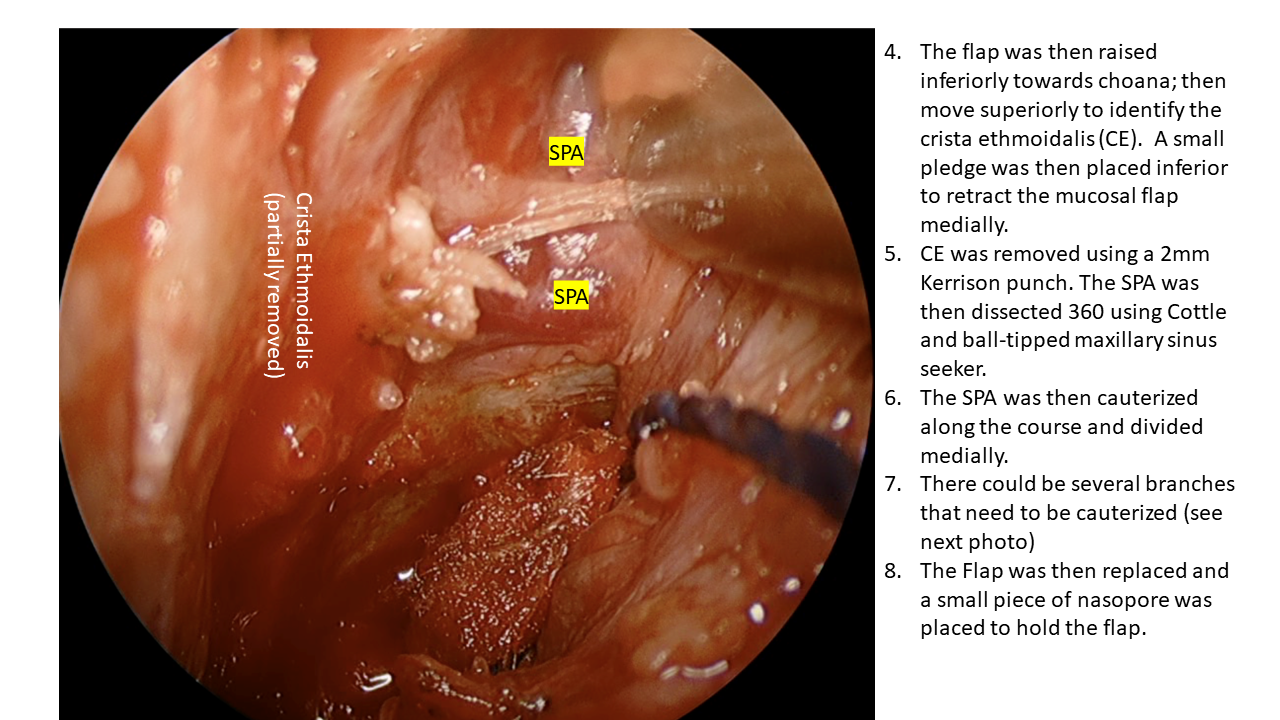
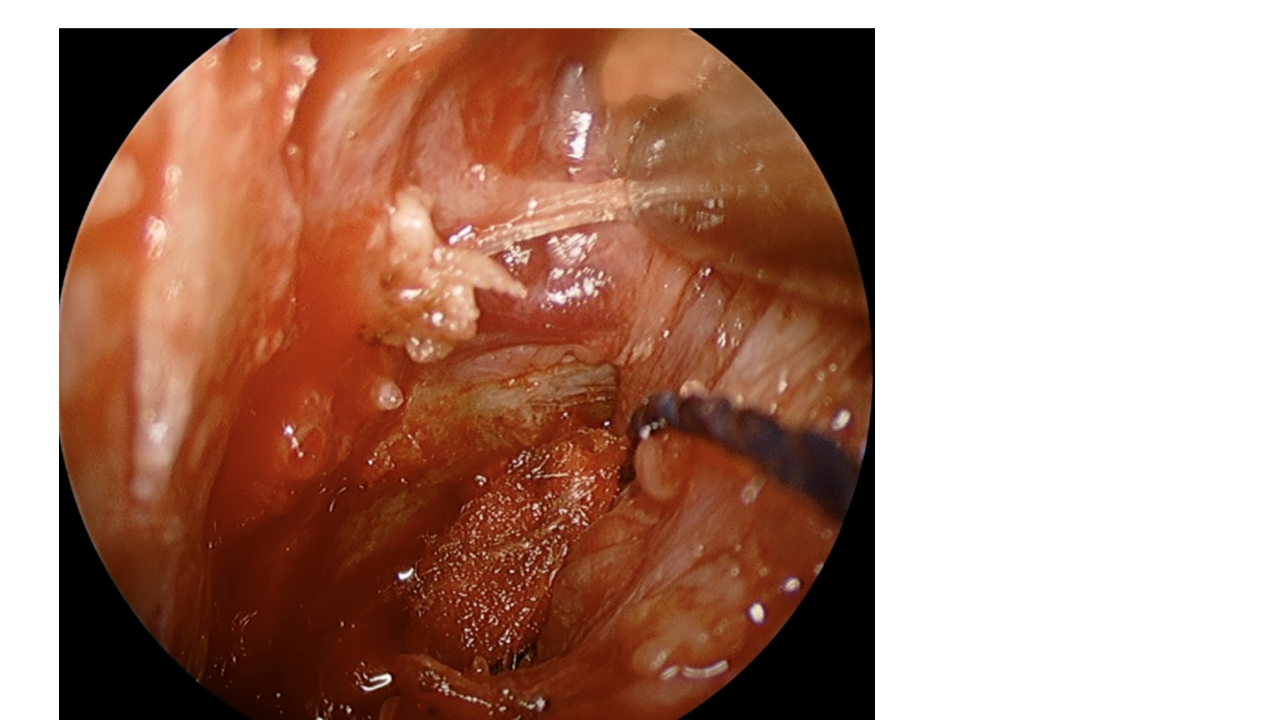
- Raise the mucosal flap inferiorly towards the choana, then move the flap superiorly. This will help identify the CE and the SPA.
- Remove the CE using a 2mm kerrison punch and a Currette. We find that it is helpful to place a small pledge (neuro-patty) inferiorly to retract the flap medially.
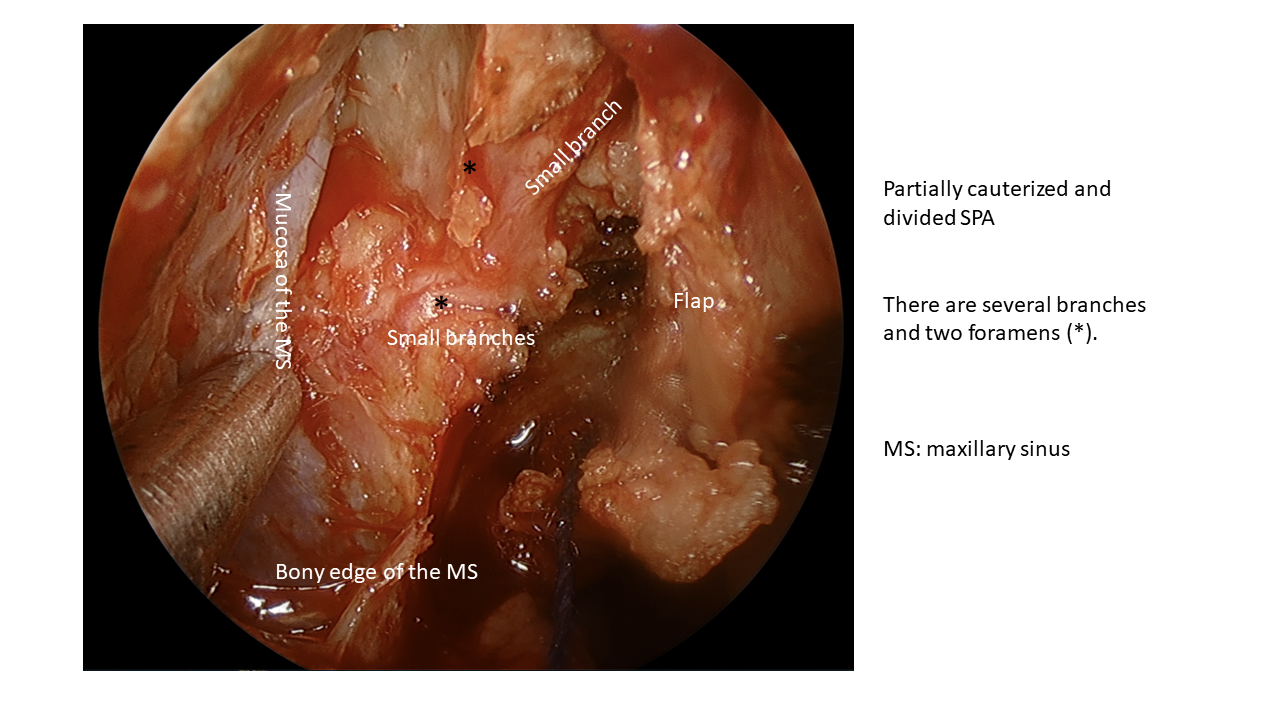
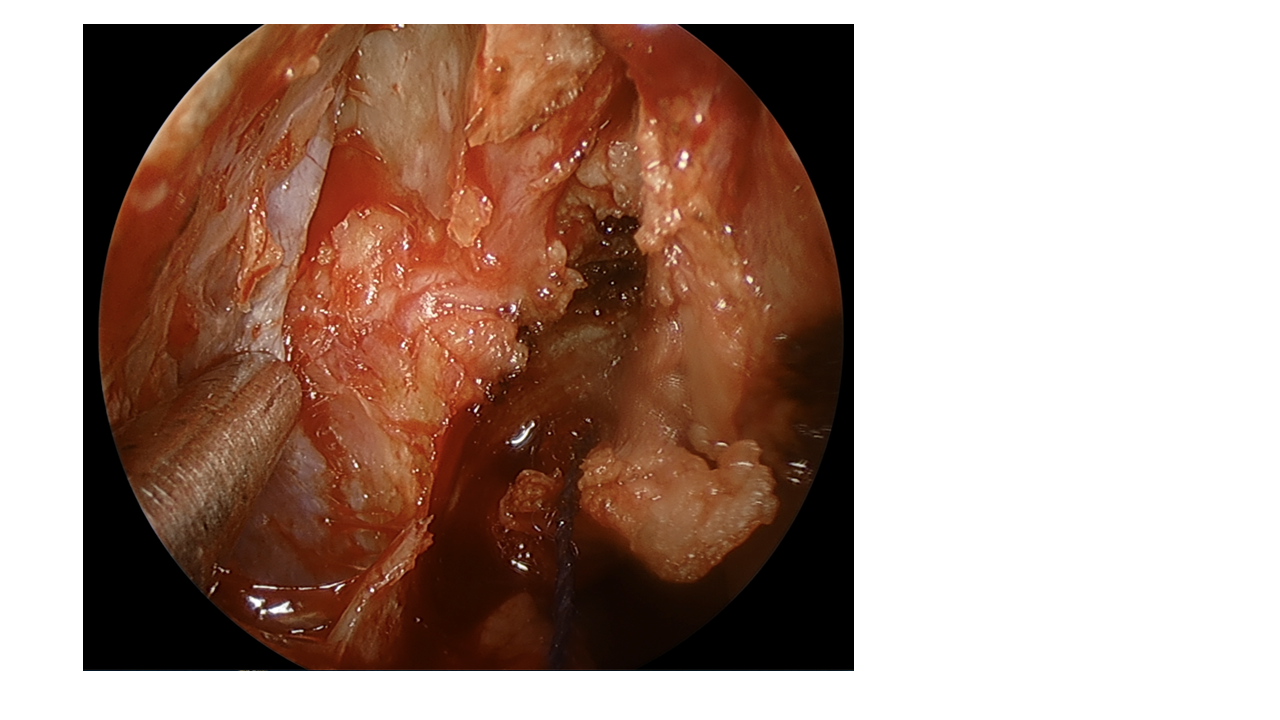
- Dissect out the SPA and its branches. We recommend cauterizing and dividing the anterior branch to ensure that hidden branches behind are identified.
- Cauterize the SPA along its course with the bipolar and divide medially. It is very important to cauterize all branches until the anterior face of the sphenoid sinus is encountered.
- Cautery has been shown to result in a lower rebleeding rate compared to clipping (Kitamura 2018).
- If hemoclips are used, it is important to dissect the vessels out 360 degrees.
- Replace the flap and secure it with a small piece of nasopore or surgicel.
Postoperative Considerations
-
Monitor patient for rebleeding. Risk factors for rebleeding include diabetes and multiple preoperative posterior nasal packing attempts (Pop 2023).
-
Most patients can be discharged the same day (Douglas 2007).
Effectiveness
- SPA ligation has been reported to be effective in 87-92% of cases (Kishimoto 2018, Wormald 2000).
- Bilateral SPA ligation has been shown to have lower rebleeding rates compared to unilateral ligation (Hervochon 2018).
- SPA ligation may reduce the risk of future severe epistaxis in anticoagulated patients.
References
Pop SS, Tiple C, Stamate MC, Chirila M. Endoscopic Sphenopalatine Artery Cauterization in the Management of Recurrent Posterior Epistaxis. Medicina (Kaunas). 2023 Jun 12;59(6):1128. doi: 10.3390/medicina59061128. PMID: 37374332; PMCID: PMC10300748.
Supriya M, Shakeel M, Veitch D, Ah-See KW. Epistaxis: prospective evaluation of bleeding site and its impact on patient outcome. J Laryngol Otol. 2010 Jul;124(7):744-9. doi: 10.1017/S0022215110000411. Epub 2010 Apr 20. PMID: 20403223.
Soyka MB, Nikolaou G, Rufibach K, Holzmann D. On the effectiveness of treatment options in epistaxis: an analysis of 678 interventions. Rhinology. 2011 Oct;49(4):474-8. doi: 10.4193/Rhino10.313. PMID: 21991575.
de Bonnecaze G, Gallois Y, Bonneville F, Vergez S, Chaput B, Serrano E. Transnasal Endoscopic Sphenopalatine Artery Ligation Compared With Embolization for Intractable Epistaxis: A Long-term Analysis. Am J Rhinol Allergy. 2018 May;32(3):188-193. doi: 10.1177/1945892418768584. Epub 2018 Apr 20. PMID: 29676168.
Budrovich R, Saetti R. Microscopic and endoscopic ligature of the sphenopalatine artery. Laryngoscope. 1992 Dec;102(12 Pt 1):1391-4. doi: 10.1288/00005537-199212000-00016. PMID: 1453849.
El-Guindy A. Endoscopic transseptal sphenopalatine artery ligation for intractable posterior epistaxis. Ann Otol Rhinol Laryngol. 1998 Dec;107(12):1033-7. doi: 10.1177/000348949810701207. PMID: 9865634.
Pothier DD, Mackeith S, Youngs R. Sphenopalatine artery ligation: technical note. J Laryngol Otol. 2005 Oct;119(10):810-2. doi: 10.1258/002221505774481354. PMID: 16259659.
Prades JM, Asanau A, Timoshenko AP, Faye MB, Martin Ch. Surgical anatomy of the sphenopalatine foramen and its arterial content. Surg Radiol Anat. 2008 Oct;30(7):583-7. doi: 10.1007/s00276-008-0390-x. Epub 2008 Jul 23. PMID: 18648719.
Flint, P.W., Haughey, B.H., Lund, V.J., Niparko, J.K., Robbins, K.T., Thomas, J.J., Lesperance, M.M., Cummings Otolaryngology-Head and Neck Surgery; Elsevier Inc.: Amsterdam, The Netherlands, 2014; pp. 733-744
Scanavine AB, Navarro JA, Megale SR, Anselmo-Lima WT. Anatomical study of the sphenopalatine foramen. Braz J Otorhinolaryngol. 2009 Jan-Feb;75(1):37-41. doi: 10.1016/s1808-8694(15)30829-6. PMID: 19488558; PMCID: PMC9442255.
Kishimoto Y, Sogami T, Uozumi R, Funakoshi M, Miyamoto SI, Kitamura M, Suzuki C, Muto M, Tateya I, Omori K. Complications After Endoscopic Laryngopharyngeal Surgery. Laryngoscope. 2018 Jul;128(7):1546-1550. doi: 10.1002/lary.26953. Epub 2017 Oct 10. PMID: 28994120.
Douglas R, Wormald PJ. Update on epistaxis. Curr Opin Otolaryngol Head Neck Surg. 2007 Jun;15(3):180-3. doi: 10.1097/MOO.0b013e32814b06ed. PMID: 17483687.
Wormald PJ, Wee DT, van Hasselt CA. Endoscopic ligation of the sphenopalatine artery for refractory posterior epistaxis. Am J Rhinol. 2000 Jul-Aug;14(4):261-4. doi: 10.2500/105065800779954455. PMID: 10979501.
Hervochon R, Khoueir N, Le Clerc N, Clément J, Kania R, Herman P, Verillaud B. Unilateral vs bilateral sphenopalatine artery ligation in adult unilateral epistaxis: A comparative retrospective study of 83 cases. Clin Otolaryngol. 2018 Dec;43(6):1591-1594. doi: 10.1111/coa.13183. Epub 2018 Jul 25. PMID: 29972723.