





return to: Bartholins duct anatomy; Submandibular Stone and Bartholin's duct; Bartholin's duct on normal sialogram; Checklist Steroid Insufflation to Salivary Glands in Clinic
Salivary flow to the submandibular duct remnant may continue despite surgical absence of a submandibular gland. Salivary flow from the sublingual gland through the normal variant of Bartholin's duct emptying into the Wharton's duct would be expected to drain through a patent duct opening into the mouth. Stricture of the distal (intraoral) segment of Wharton's duct may result in impaired drainage of the sublingual gland and may warrant a formal ductoplasty ('sialodochoplasty') as in the example below done under local anesthesia.
Modified Operative Note
Anesthesia: Topical 4% spray to the floor of mouth followed by 1 cc of 2% lidocaine 100,000 epinephrine injected around the duct and its orifice
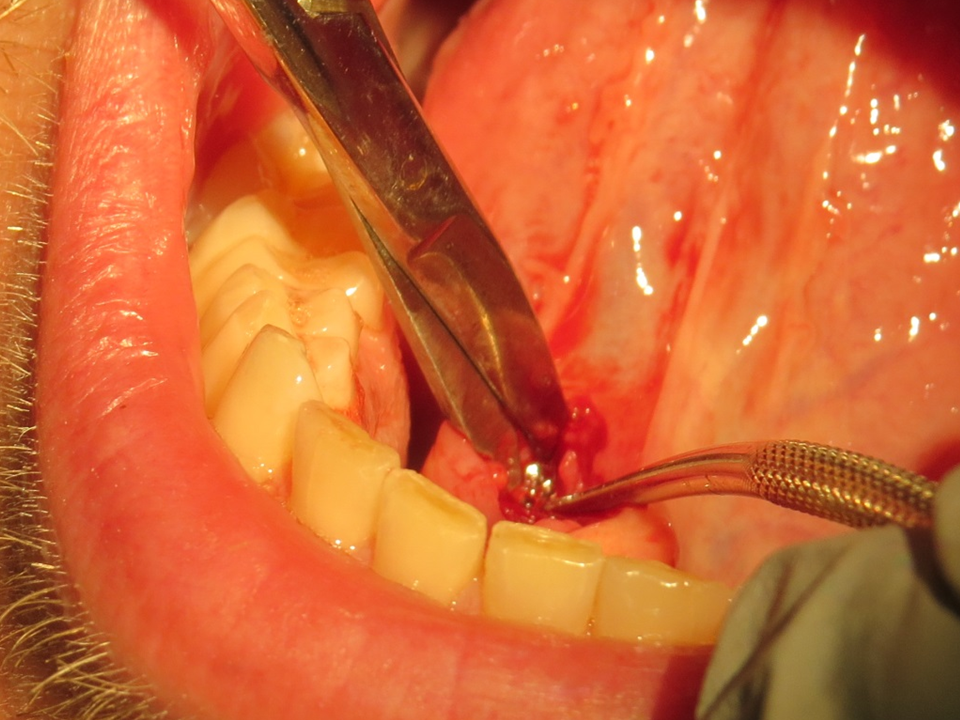
Description of Procedure: Following identification the patient informed consent and a brief timeout and confirmation of his premedication with Augmentin in the microscope room imaging of the floor of mouth identified occlusion of the right Wharton's duct orifice with the ballotable accumulation of fluid beneath the dilating the duct orifice. Forceps were removed used to remove the overlying mucosa and then the tip of the duct orifice was opening the duct in a spatulated fashion allowing for delivery of thick yellow mucoid unaffected (serous) type of material with forceps delivered deeply into the duct orifice showing no stone. A total of 7 7-0 PDS sutures were placed individually with microscopic control to marsupialize and mature the duct orifice
He tolerated the procedure well without complication was discharged home on oral Peridex rinses 4 times a day for the next 2 weeks as well as finishing his course of antibiotics with suggestions regarding Tylenol versus ibuprofen for pain and use of a teabag topically if he were to have any bleeding follow-up is targeted in 6 weeks there was no blood loss and no need for cautery.