











Note: last updated before 2013
GENERAL CONSIDERATIONS
Pleomorphic Adenomas of the hard and soft palate are extremely rare. This represents a tumor of the minor salivary gland that may be locally aggressive, and accounts for 40-70% of all major and minor salivary gland tumors.
IMAGING
see also: Pathology: Pleomorphic Adenoma
Radiology: Pleomorphic Adenoma Rads
Surgery: Buccal Fat Flap Reconstruction of Palate Defects
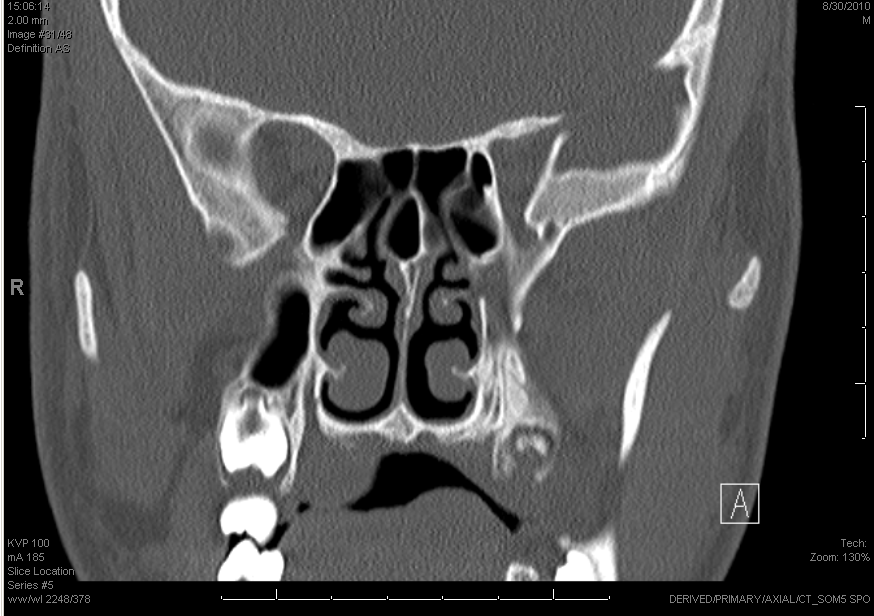
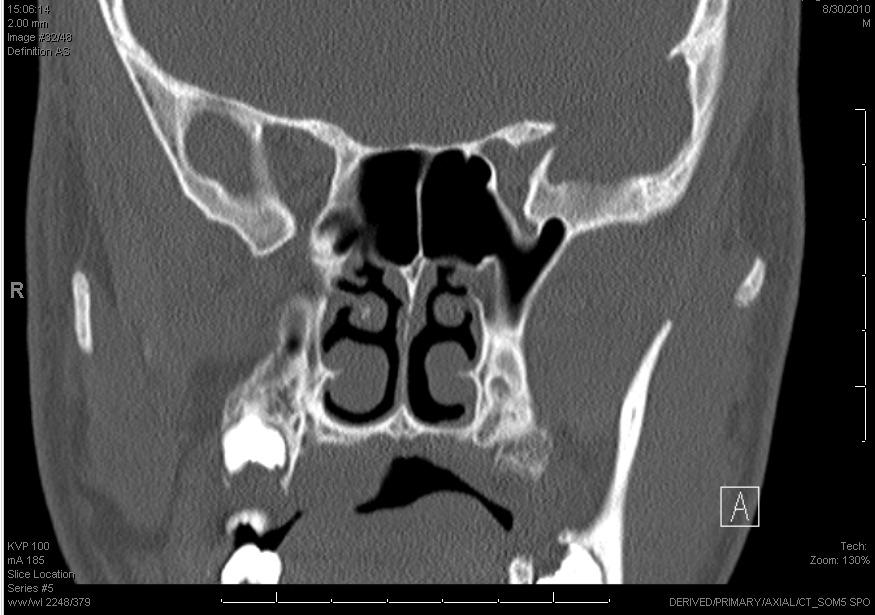
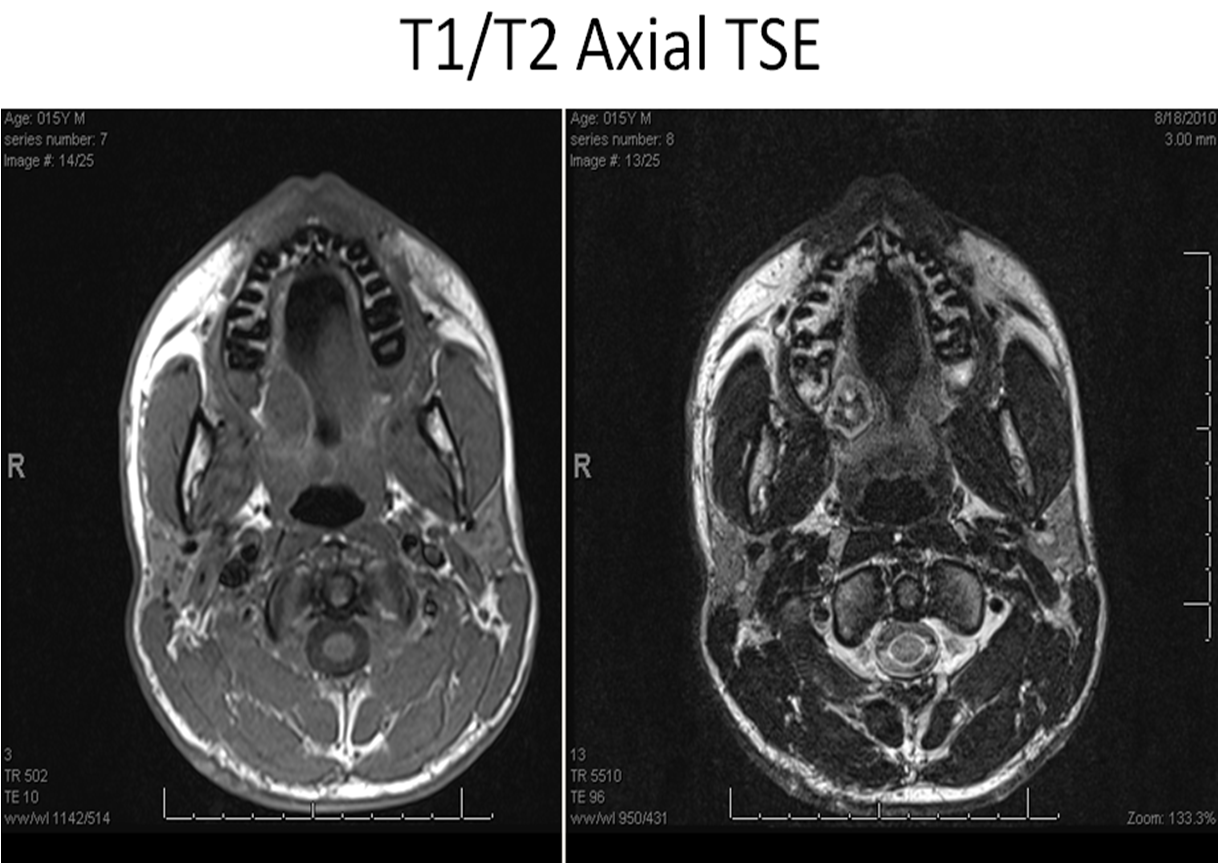
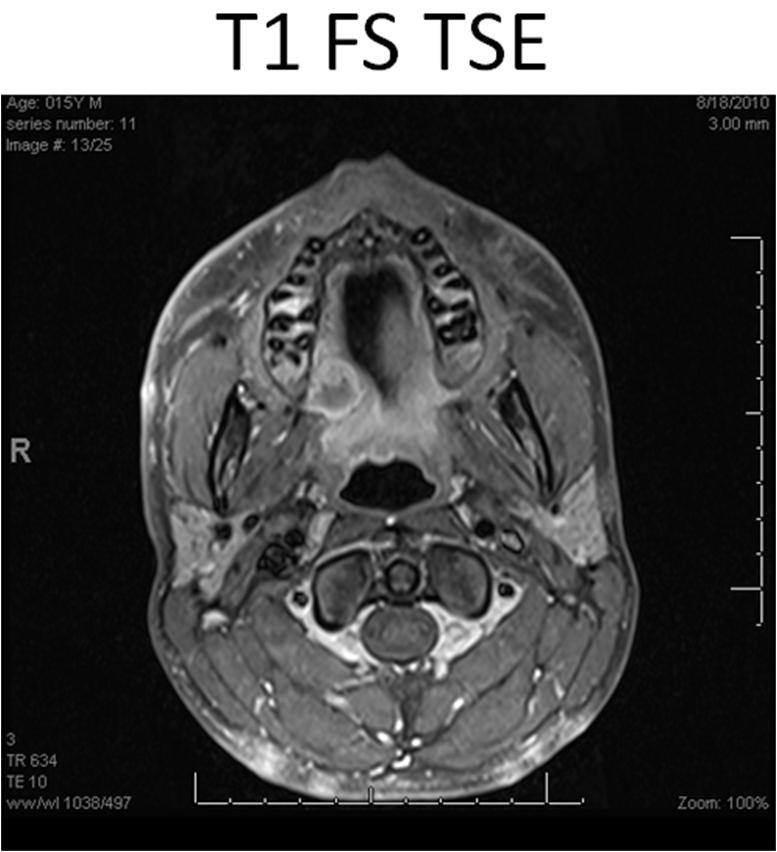
Considerations for imaging include both a CT scan and an MRI. CT scan will evaluate for any bony destruction or involvement of the mass
- MRI is used to evaluate extent of disease. This tumor commonly extends through the soft palate into the nasopharynx, or may track up the greater palatine foramen.
NURSING CONSIDERATIONS
- The 0 degree endoscope must be set up to allow the surgeons to evaluate the nasopharynx
- The tonsil tray is utilized
- The Colorado tip monopolar cautery is used
- Bien drill with a large diamond head burr is used to drill the soft palate.
ANESTHESIA CONSIDERATIONS
- The appropriate sized MLT tube should be used, and taped at midline to the lower lip. We will utilize the Crowe-Davis device for exposure.
OPERATIVE PROCEDURE
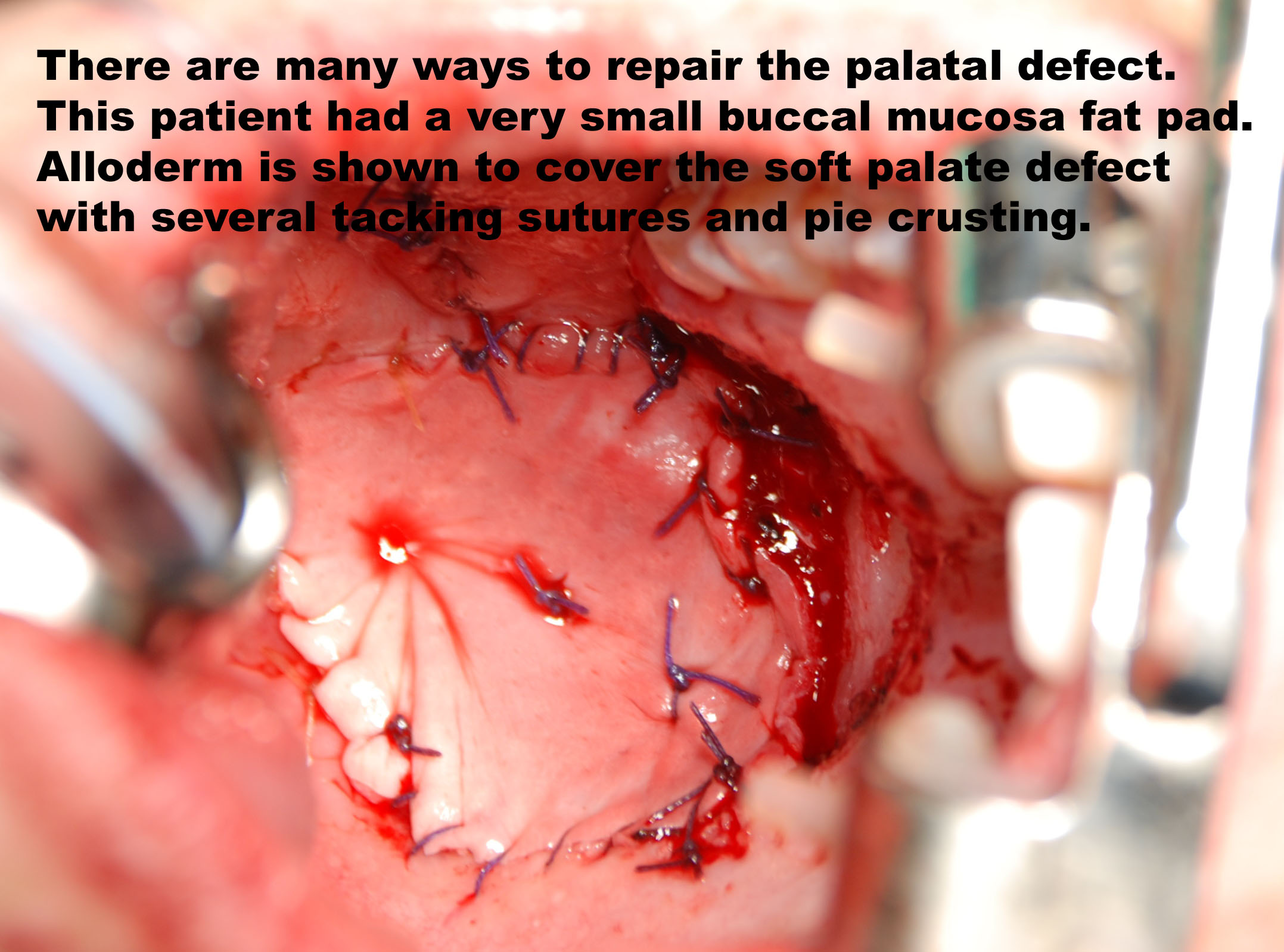
- Appropriate reconstruction should be considered prior to the procedure. The pedicled buccal fat pad graft is a great way to close the palatal defect. This is particularly useful if the floor of the nasopharynx is entered secondary to extention of the tumor. The fat pad may be placed, with a Merocel pack placed in the nasopharynx over the graft.
- Thin Alloderm may be placed over the soft palate to reduce contraction of the palate. This is performed to prevent VPI.
- Avitene was used to cover the bone of the hard palate and close the greater and lesser palatine foramen. This is performed after frozens are confirmed.
- An Obturator is created for support of the reconstruction. Two 2.0 mm KLS screws that are 13 mm in length are placed through the hard palate to secure the obturator in place. Care is taken to avoid any tooth roots.
REFERENCES
Lopes MA, Kowalski LP, Da Cunha Santos G, Paes de Almeida O. A clinico pathologic study of 196 intraoral minor salivary gland tumours. J Oral Pathol Med 1999; 28:264-267.
Loyola AM, De Araujo VC, De Souza SOM, De Araujo NS. Minor salivary gland tumors. A retrospective study of 164 cases in a Brazilian population. Eur J Cancer B Oral Oncol 1995;31:197-201
Worthington P. The management of the palatal pleomorphic adenoma. Br J Oral Surg 1974; 12:132-140
Johnson LP A review of the use of Avitene in otolaryngologic surgery. Otolaryngol Head Neck Surg. 1980 Jan-Feb;88(1):8-9.
Kramer GM, Pollack R. Clinical application and histologic evaluation of microfibrillar collagen hemostat (Avitene) in periodontal surgery. Int J Periodontics Restorative Dent. 1982;2(1):8-16.
Alkan A, Inal S. Closure of palatal defects following excision of palatal pleomorphic adenomas. J Contemp Dent Pract. 2008 Sep 1;9(6):99-107. Review.