

Modified Operative Note
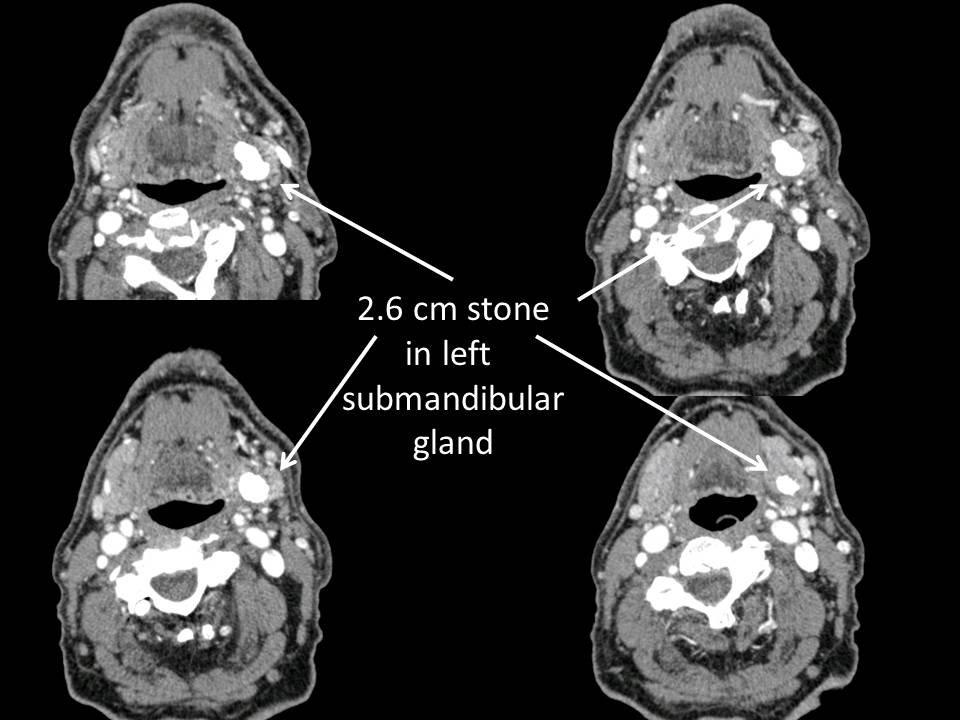
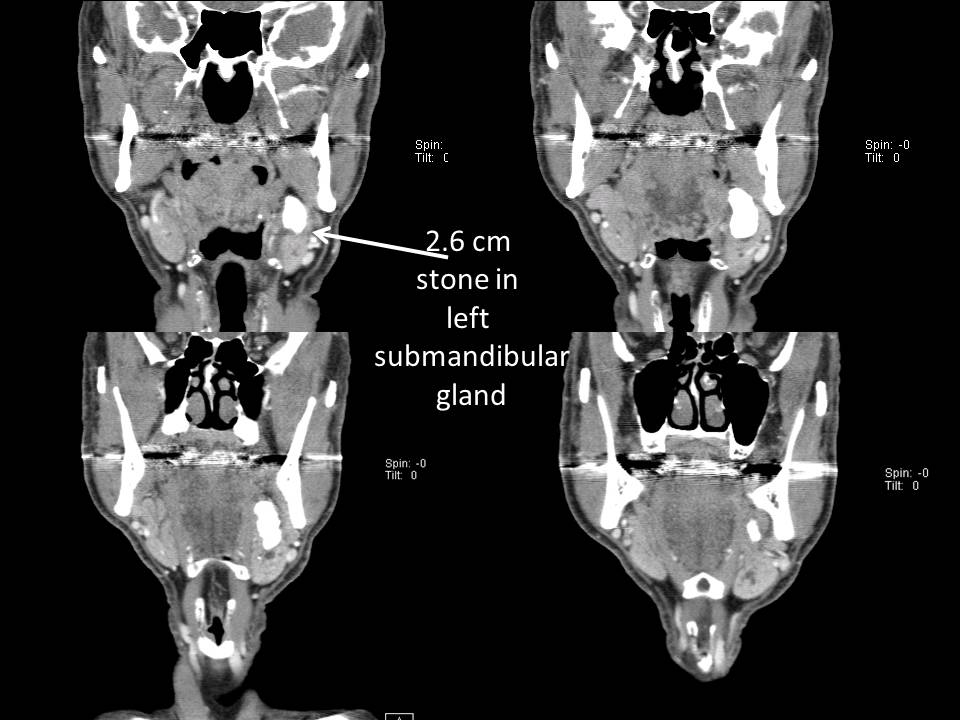
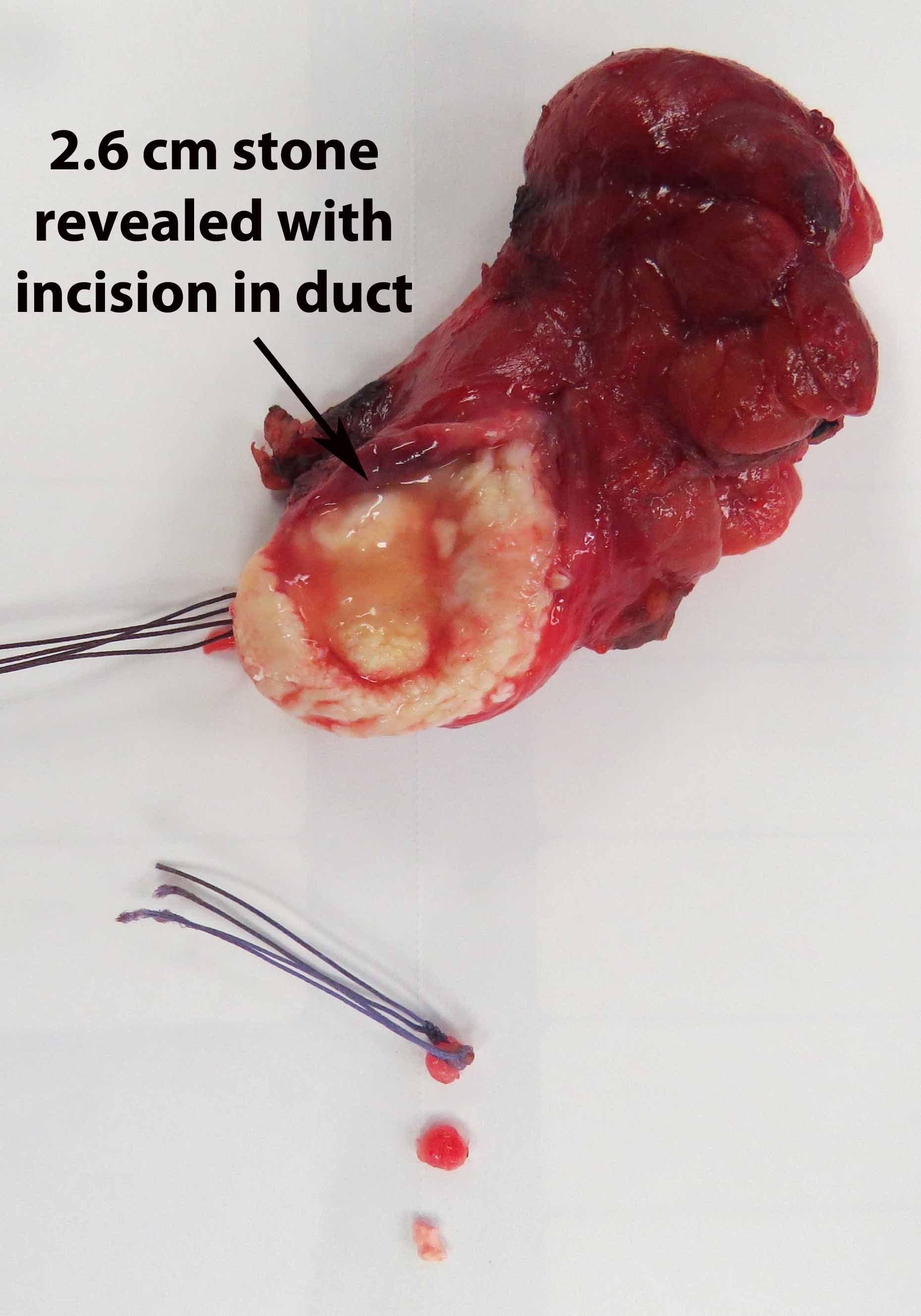
Pre Op Dx: 2.6 cm left submandibular stone with recurrent sialadenitis
Postop Dx: same - with second stone in distal submandibular duct
Procedure
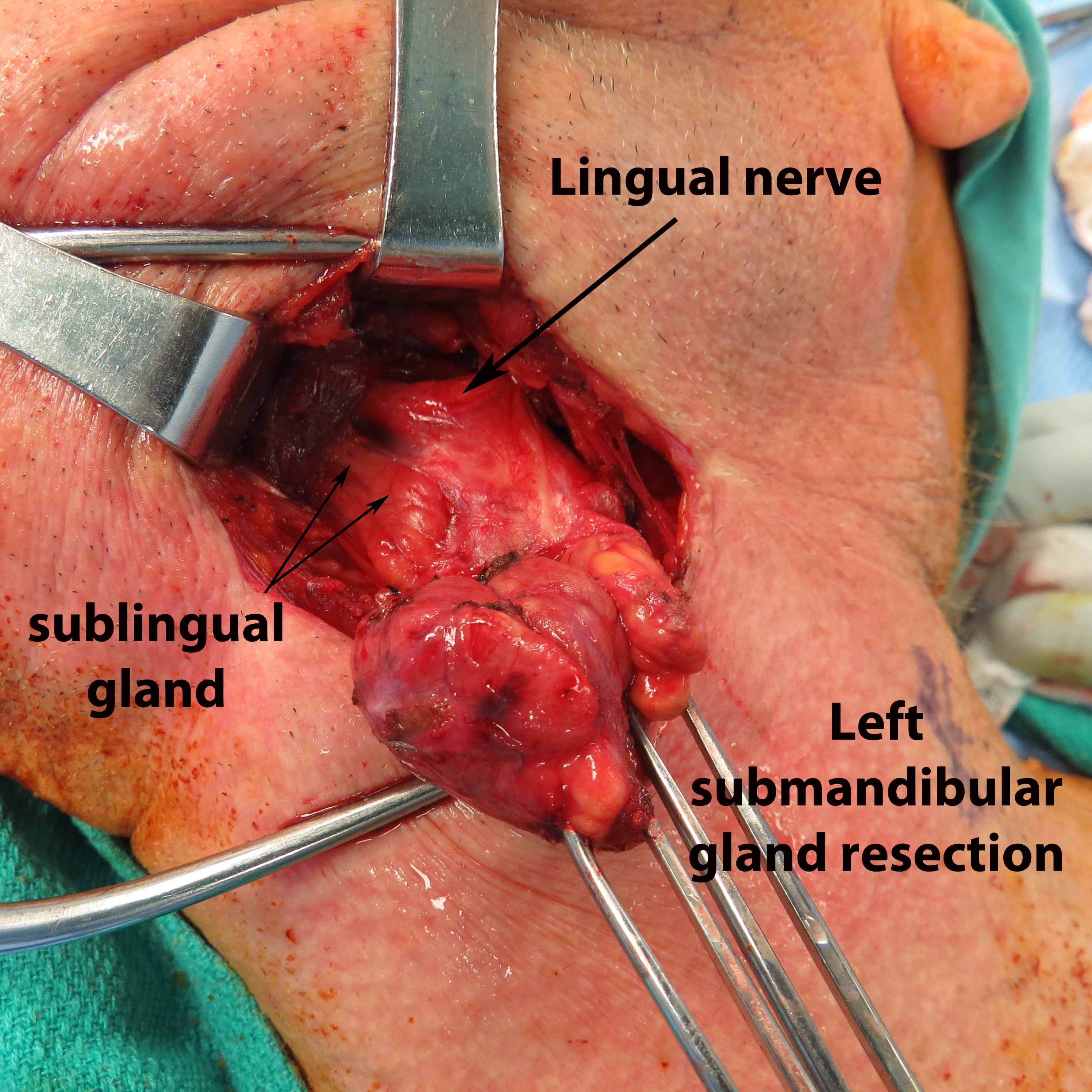
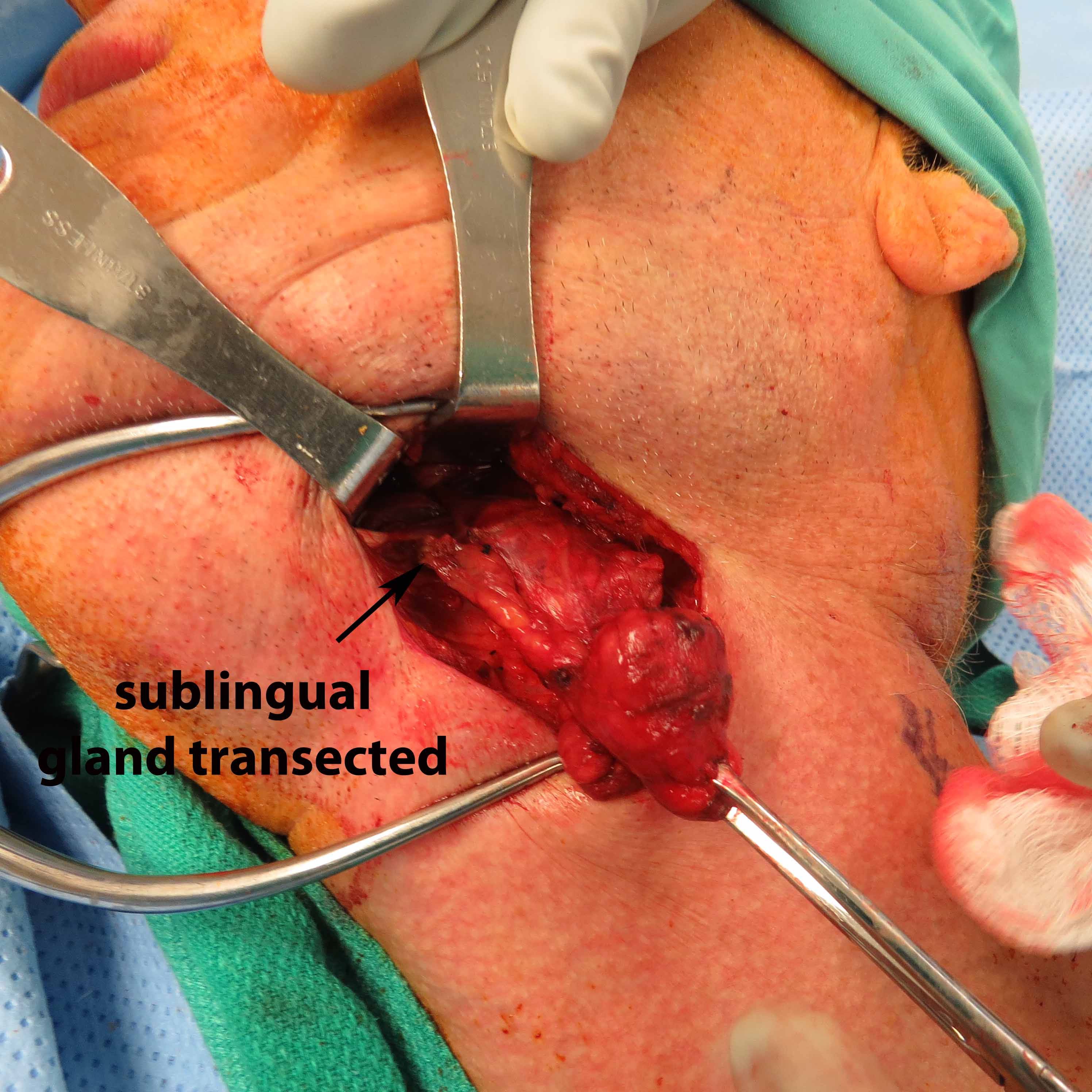
Sialodochoplasty (sialendoscopy) with resection of distal duct papilla to remove distal stone; Left submandibular gland resection
Findings:
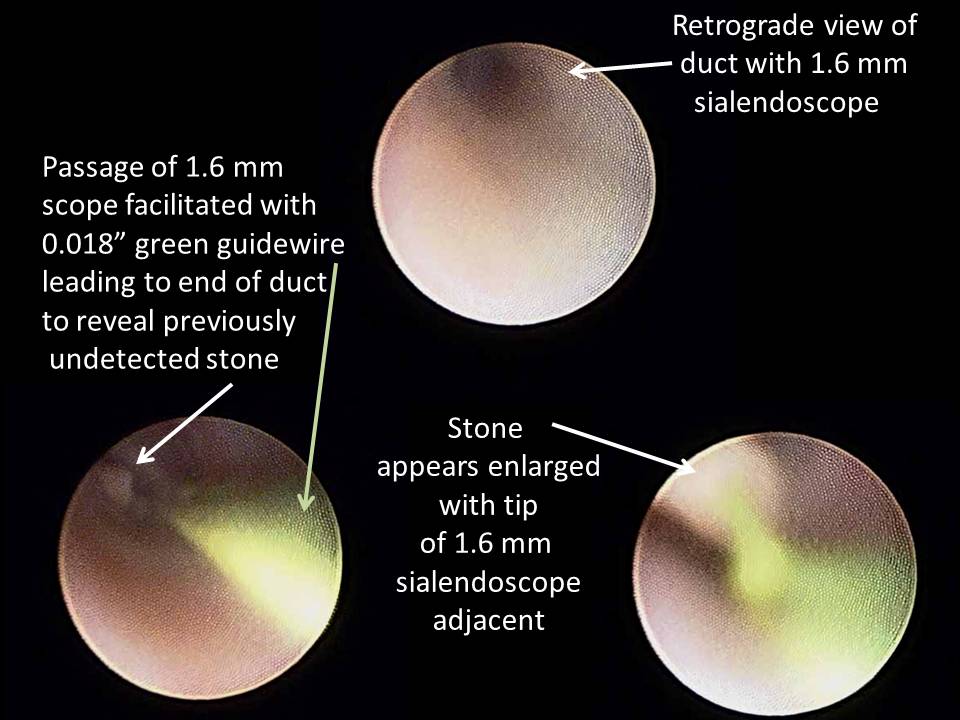
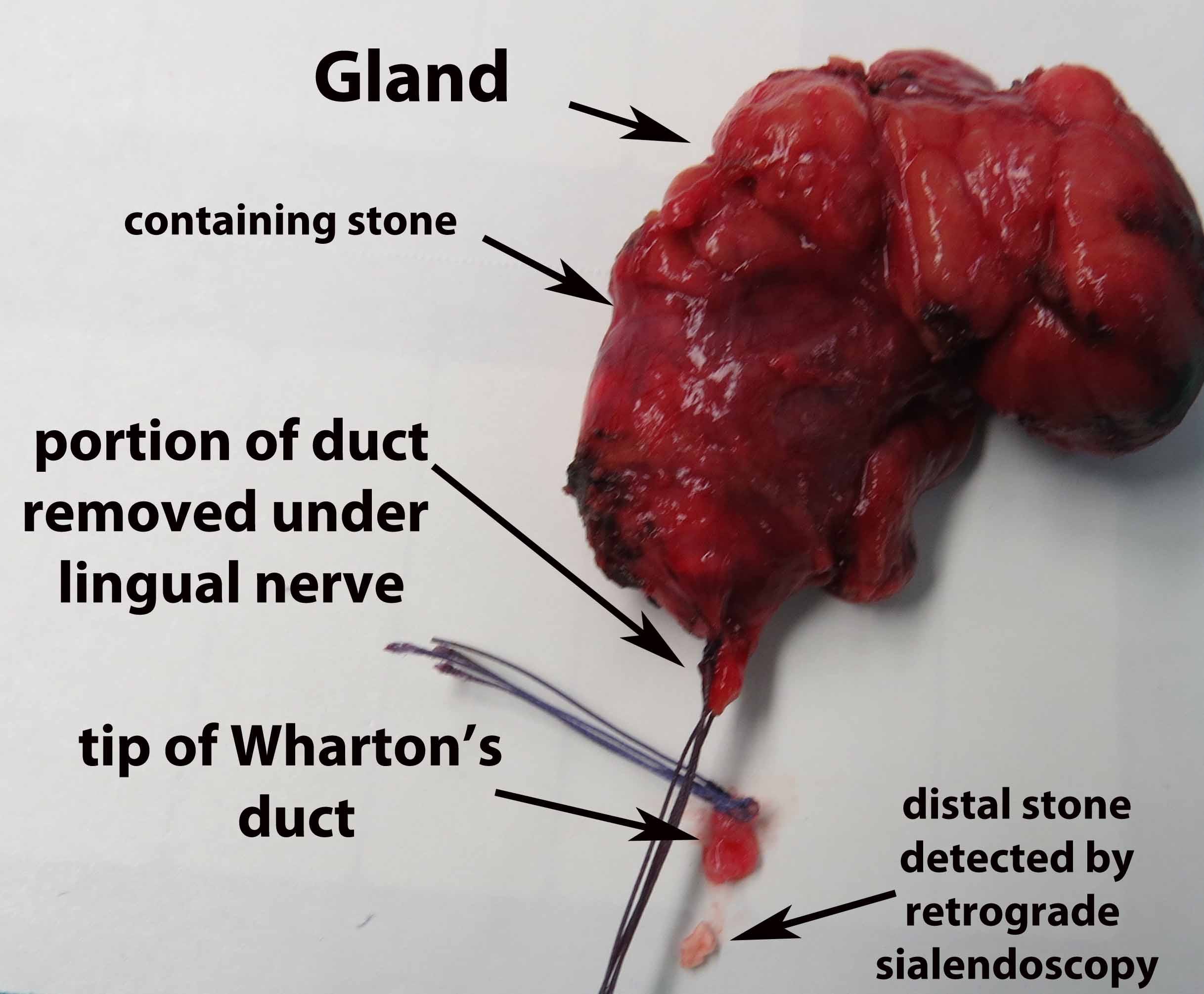
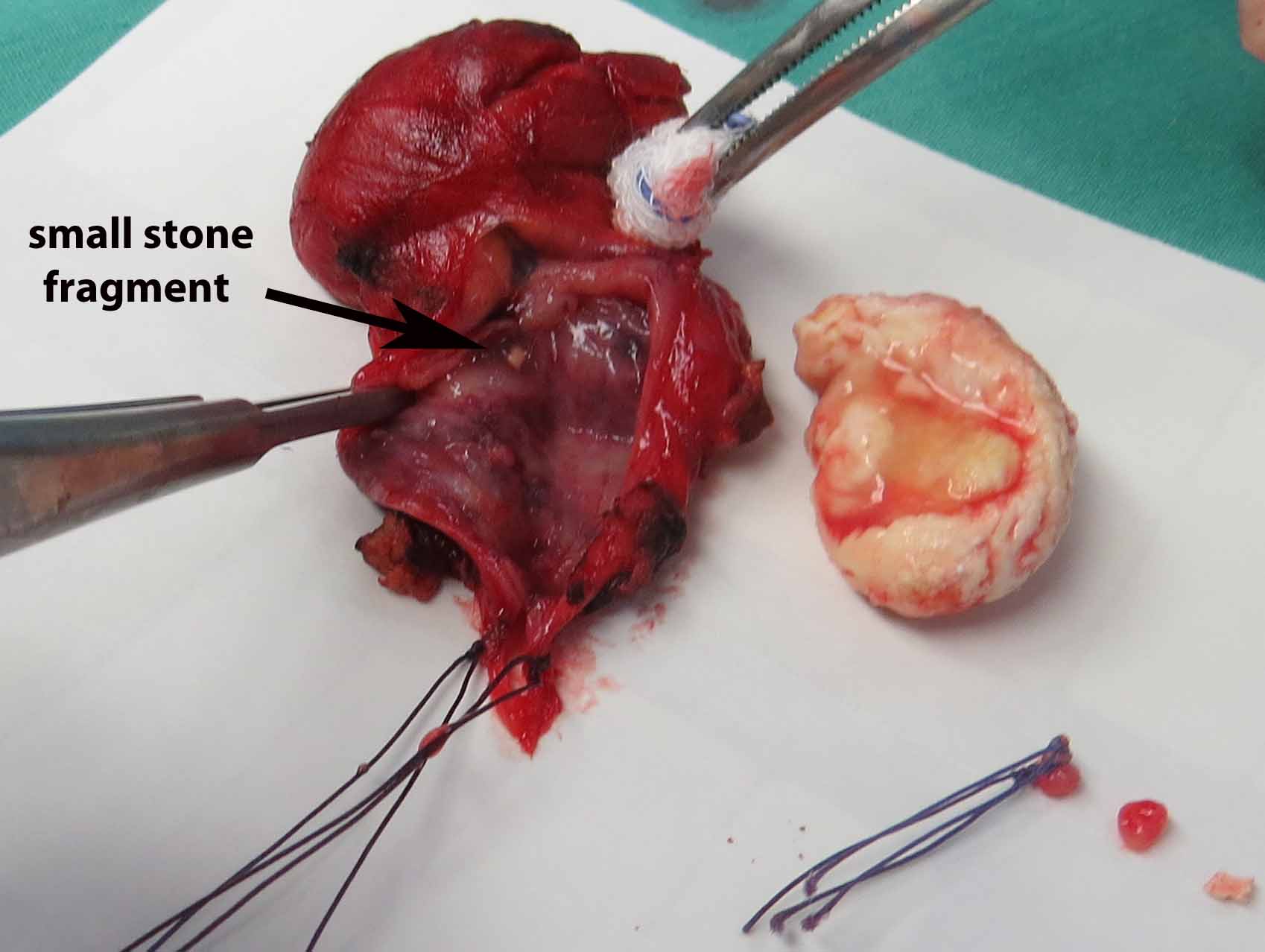
Antegrade (commonly misconstrued as retrograde) sialendoscopy done after gland removal to direct resection of tip of left submandibular gland duct and associated stone.
Large distal stone removed with SMG. Small proximal stone identified on antegrade sialoendoscopy and removed using ductoplasty approach.
Anesthesia: General
PROCEDURE DETAILS
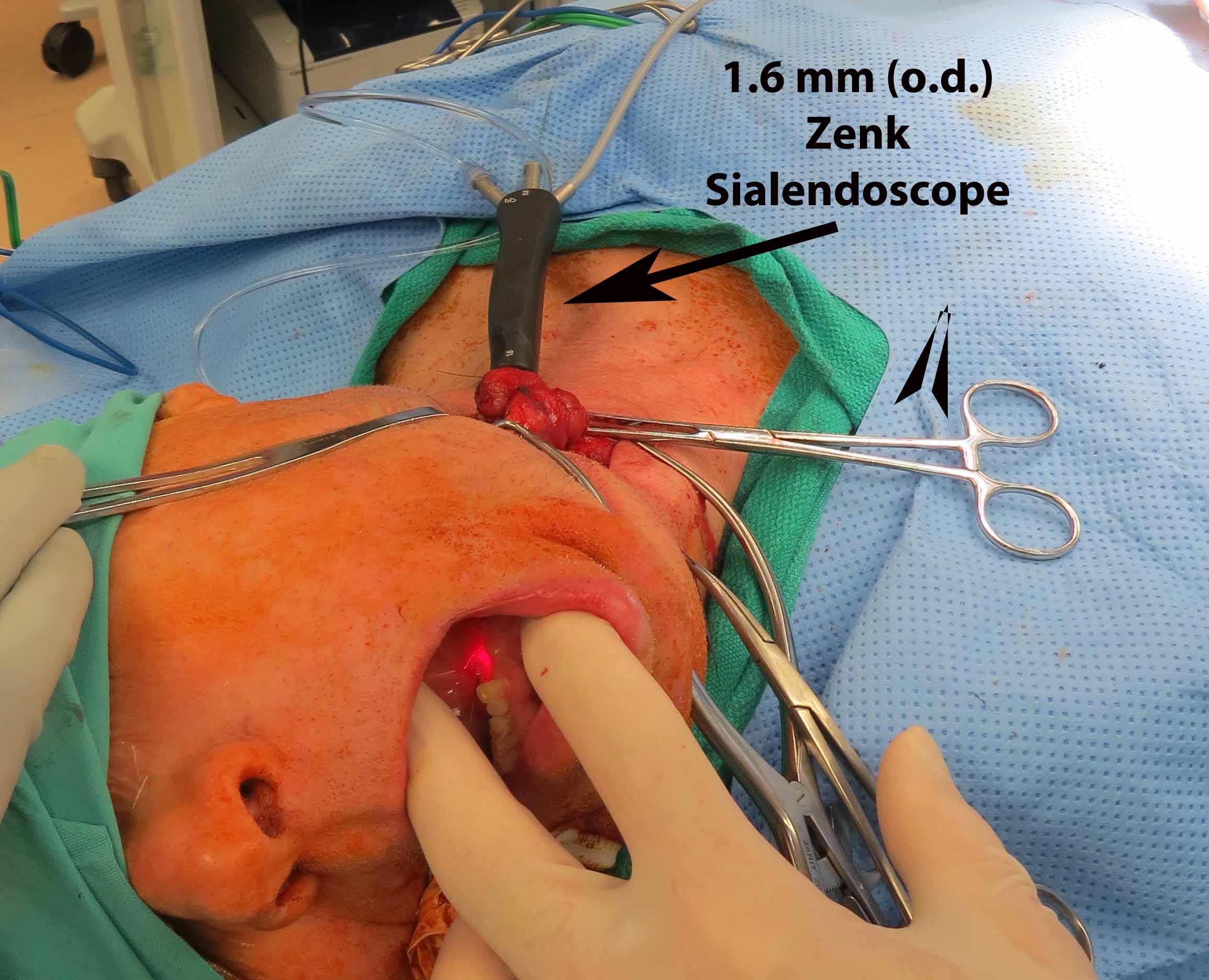
General endotracheal anesthesia was induced. The tube was taped off to the right. All pressure points were appropriately padded. He was turned 180 degrees away from our anesthesiologist. He was prepped (intraoral placement of throat pack followed by rinses with dilute betadine solution) and draped in a sterile fashion for both combined intraoral sialendoscopy and a cervical approach for submandibular gland resection. First, the submandibular papilla sialendoscopy was performed. The microscope was brought in and a 0.018 inch guidewire was introduced into the submandibular gland papilla on the left. A 22 gauge Angiocath was introduced over this and it was dilated appropriately for introduction of Marchal dilators. The small size of the Marchal dilator was used. Roughly 1 mL of 1% lidocaine was instilled for topical anesthesia into the submandibular duct. Upon initial sialendoscopy, using the 0.08 sialendoscope was advanced with a proximal stone identified near the puncta.
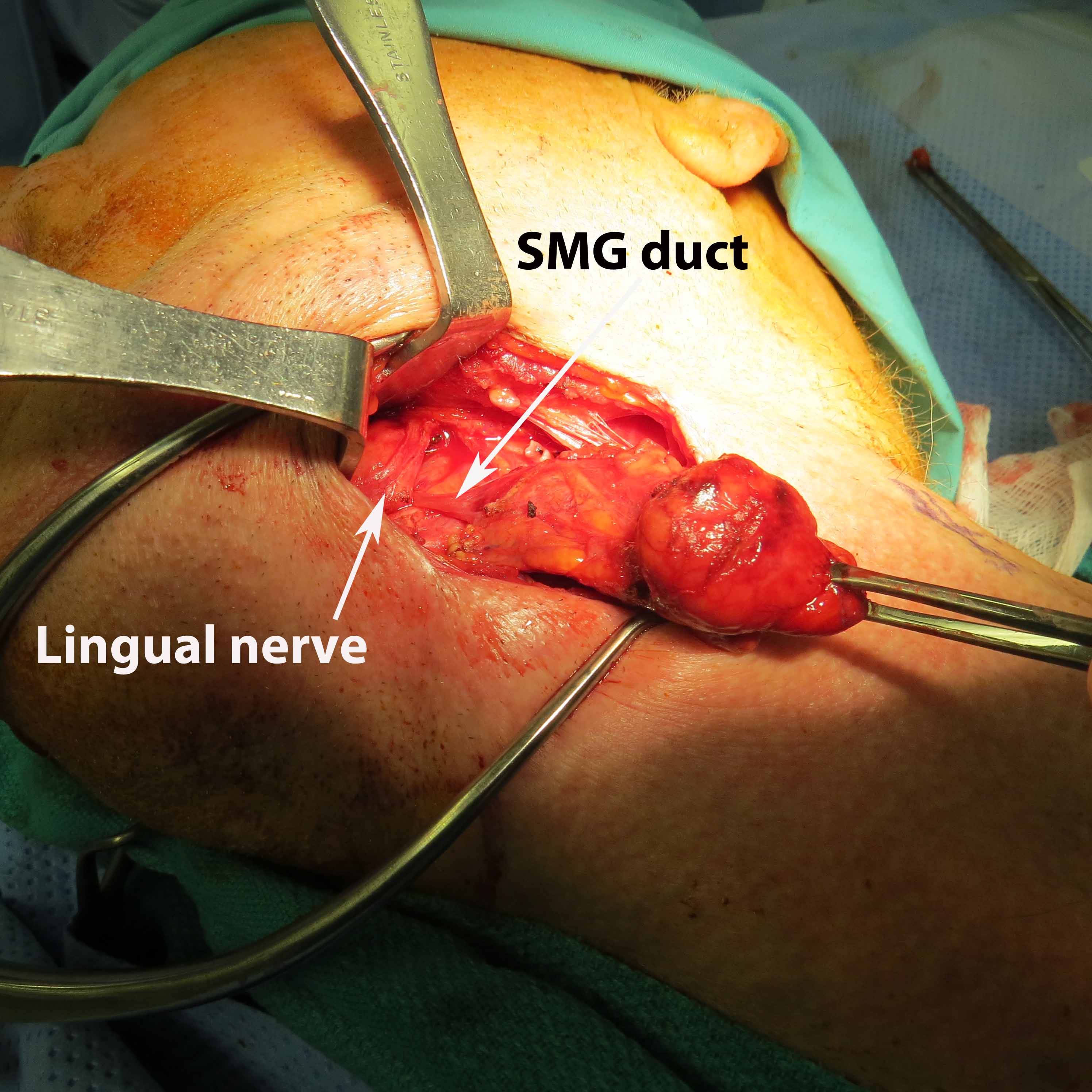
The sialendoscope was then removed and the neck was approached, roughly 2 fingerbreadths below the level of the angle of the mandible. A horizontal incision was made from the anterior border of the SCM medially. This was then incised down to the subplatysmal plane. The anterior border of the SCM was exposed permitting identification of the posterior inferior border of the submandibular gland. The marginal mandibular nerve was seen to be ptotic identified, stimulated and preserved. The inferior aspect of the submandibular gland identified and fascia incised. The dissection was proceeded medially, the inferior aspect of the submandibular gland. This was then grasped with an Allis clamp and pulled downward. The lateral aspect of the mylohyoid was identified and medialized using Army-Navy. The dissection proceeded with a submandibular gland in a subcapsular plane with downward traction and the lingual nerve was identified, as well as the stone inside of the submandibular duct which was seen to be extremely hard and quite large. The sublingual gland and lingue nerve were dissected free. The posterior facial nerve was suture ligated and used to retract the marginal mandibular nerve up and out of our field. The duct was then entered using 4-0 Vicryl to grasp either side of the duct. It was entered just proximal to the stone and recannulated for a antegrade sialendoscopy.
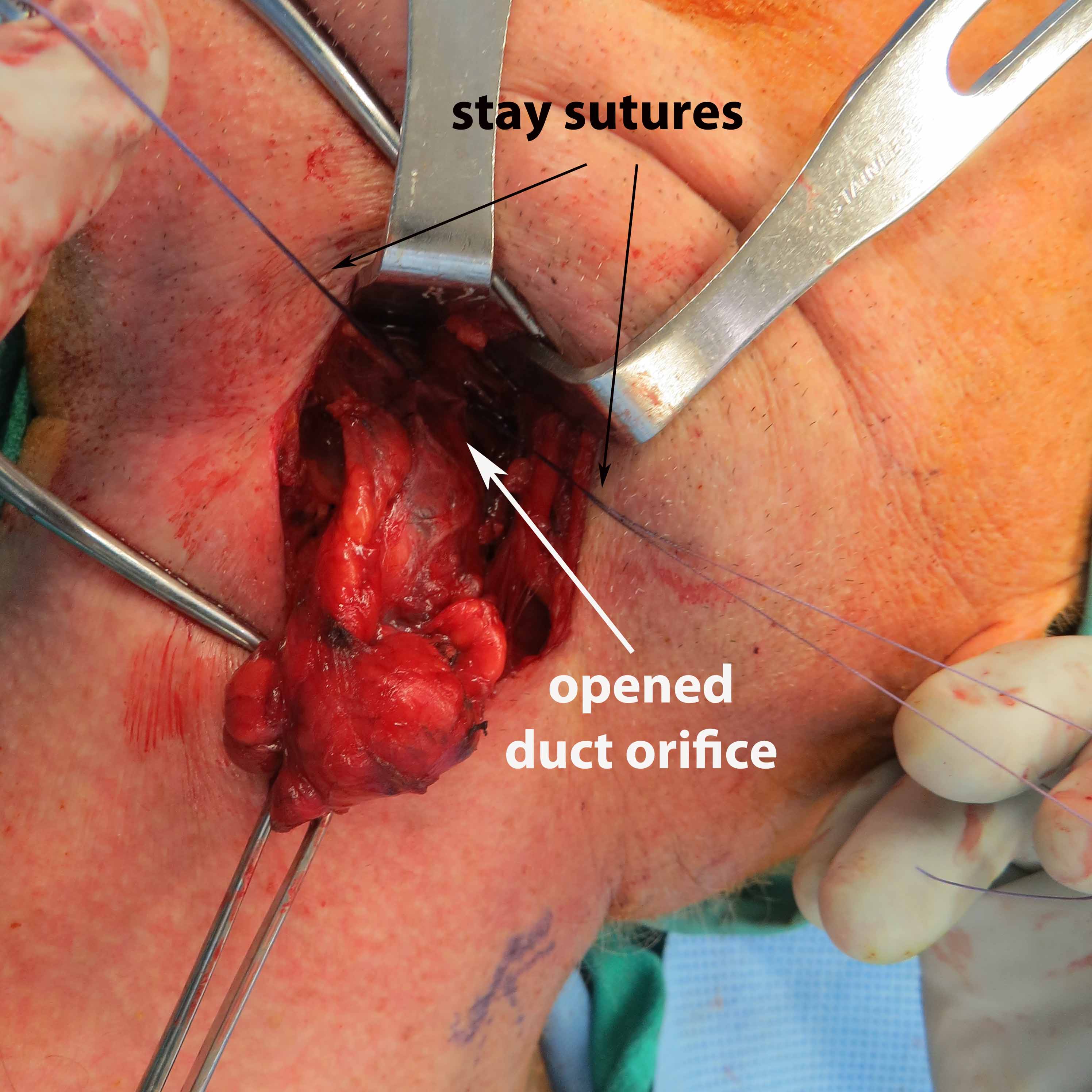
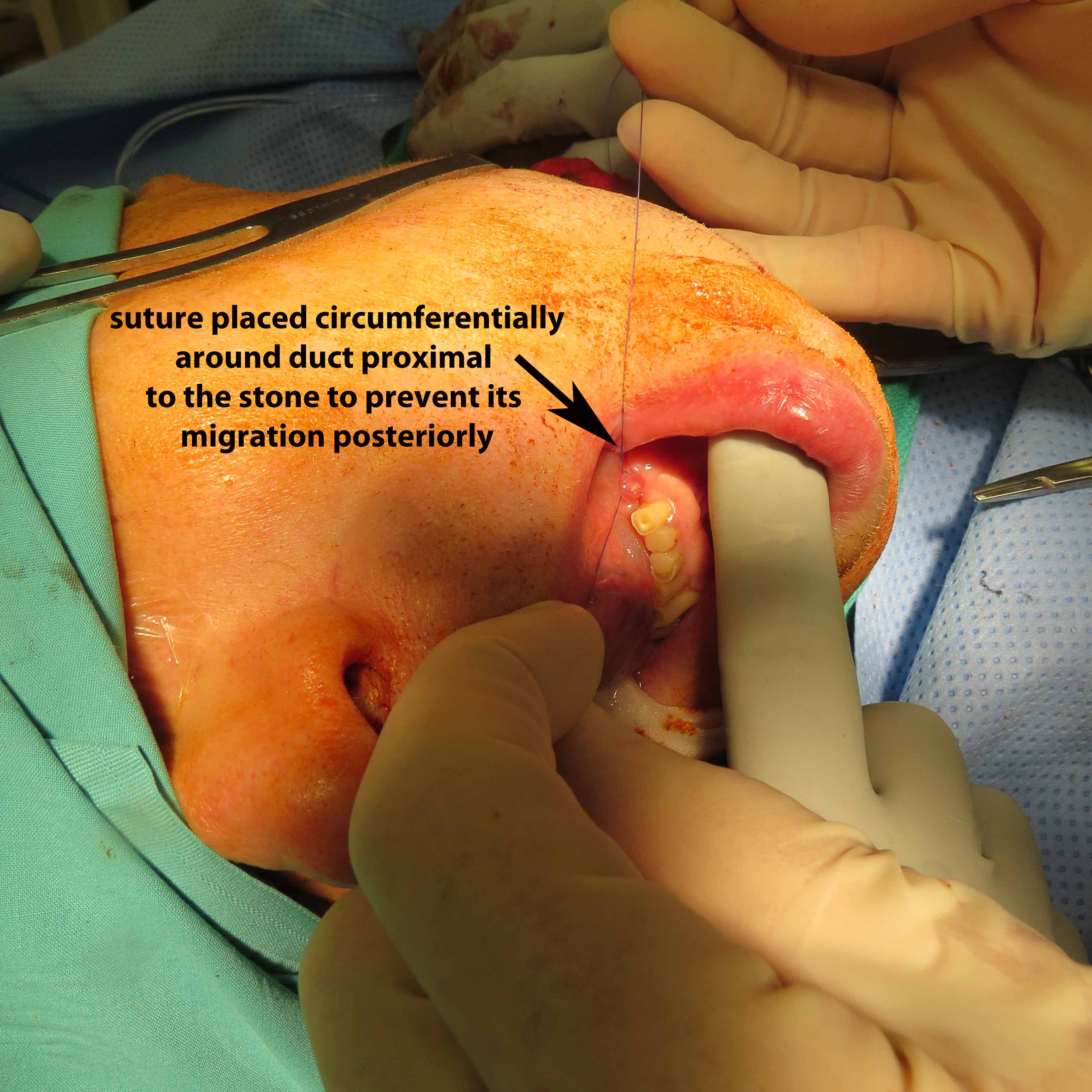
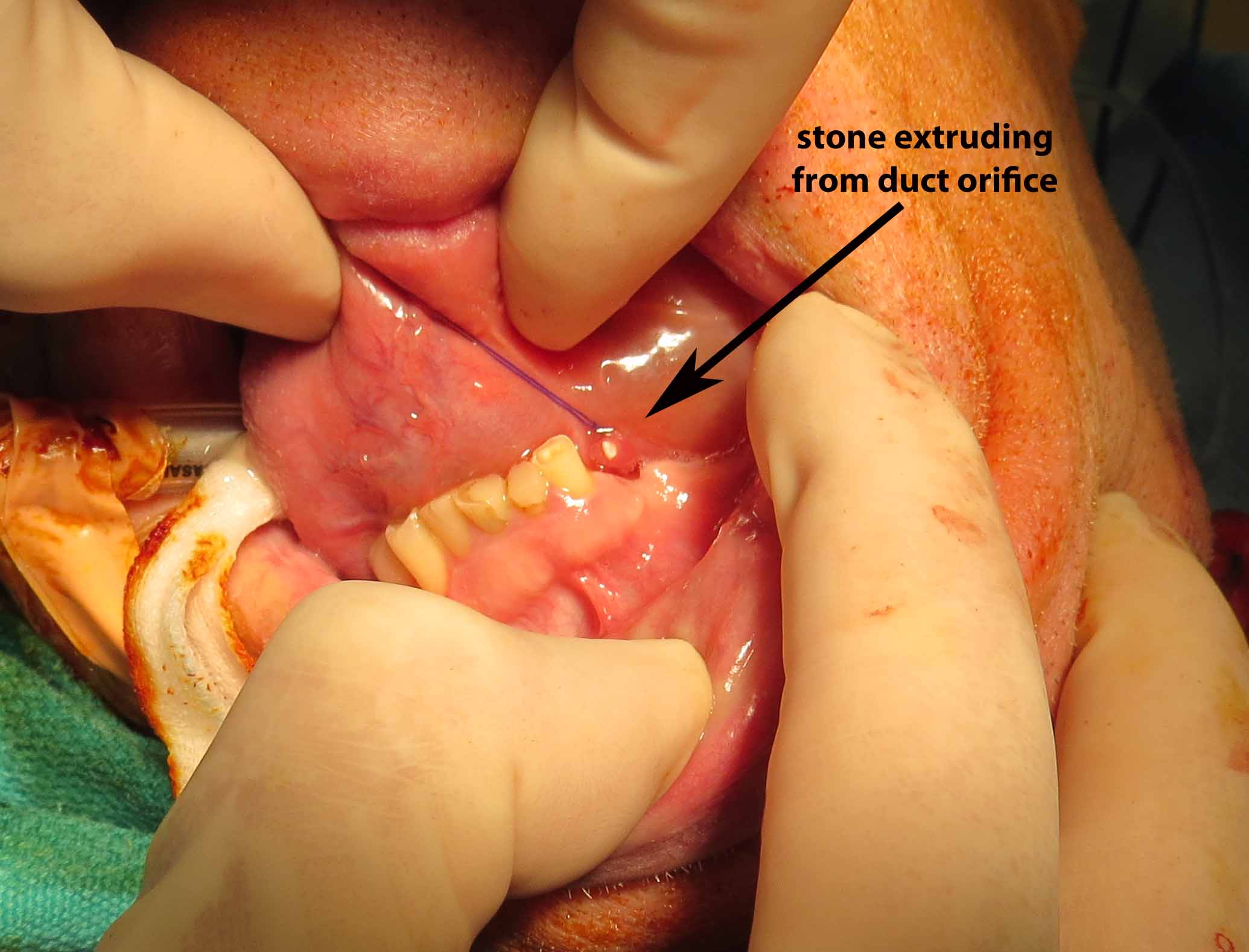
A antegrade endoscopy did show what was previously suspected as a proximal stone close to the papilla. This was actually at the level of the papilla. Circumferential placement of a 3-0 vicryl about the distal duct was done to prevent migration of the stone. The tip of the duct was then excised, removed, and sent for permanent pathology. The duct was left open into the floor of mouth. The submandibular gland was then removed slowly, using a mini clip to ligate the duct distally under the lingual nerve and sent for permanent pathology as well.
The wound was checked for hemostasis and was irrigated thoroughly. A 10 mm perforated Jackson-Pratt drain was placed. It was closed in 2 layers using 4-0 Vicryl in interrupted fashion for the platysmal and subcutaneous plane, as well as a 4-0 nylon in interrupted fashion for the skin. It was cleaned, dried, and bacitracin was applied, turned back to the care of Anesthesia colleagues for stable extubation, transferred to postop care, having tolerated the procedure well.
References
Potash A, Hoffman HT. Retrograde sialendoscopy: a new technique for avoiding retained ductal stones. Ann Otol Rhinol Laryngol. 2012 Jan;121(1):38-43.