












Click on thumbnail above to enlarge; advance with cursor over lateral border
See also: Parotidectomy for Chronic Parotitis; Parotidectomy with Facial Nerve Dissection; Sjogren's Syndrome
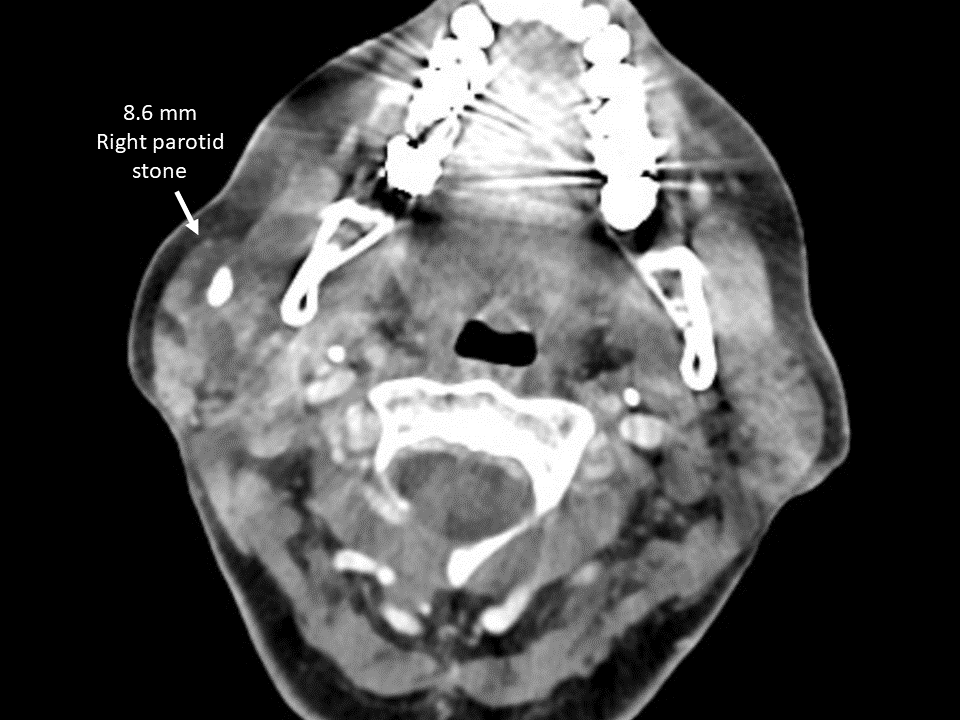
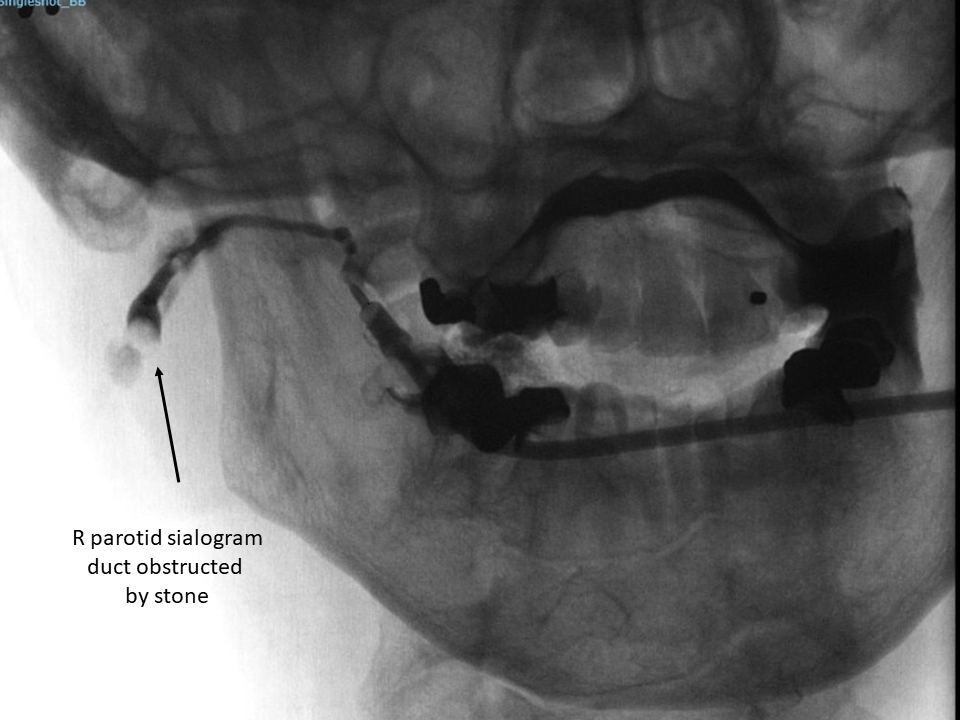
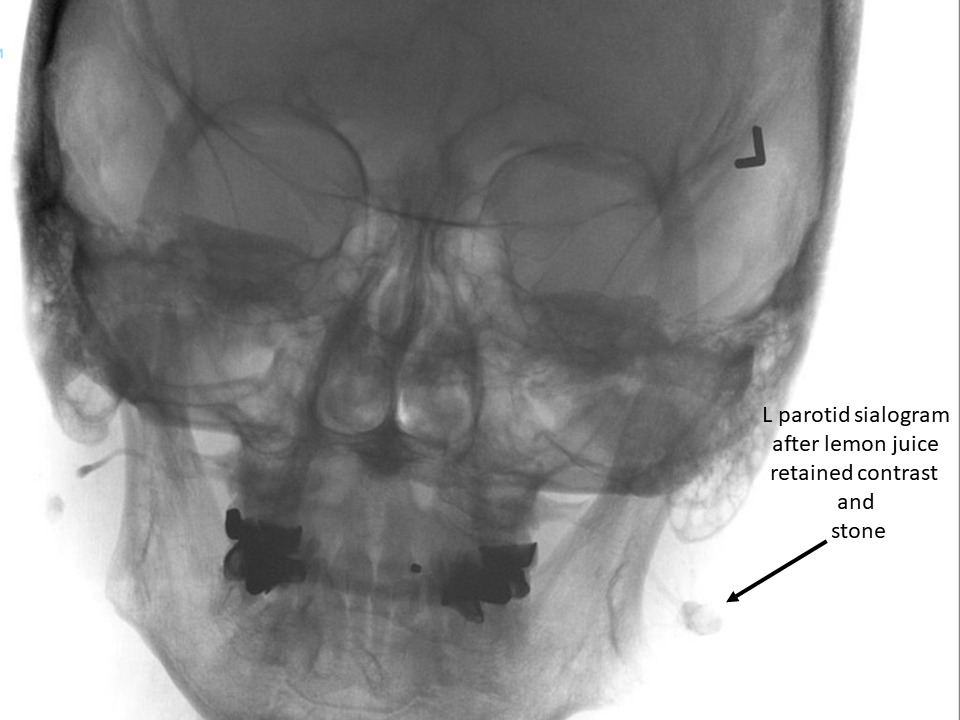
SSA (SS-A/Ro) and SSB (SS-B/La) antibody positive Sjogrens syndrome with recurrent parotid swelling, pain and bilateral parotid stones
Preoperative Assessment:






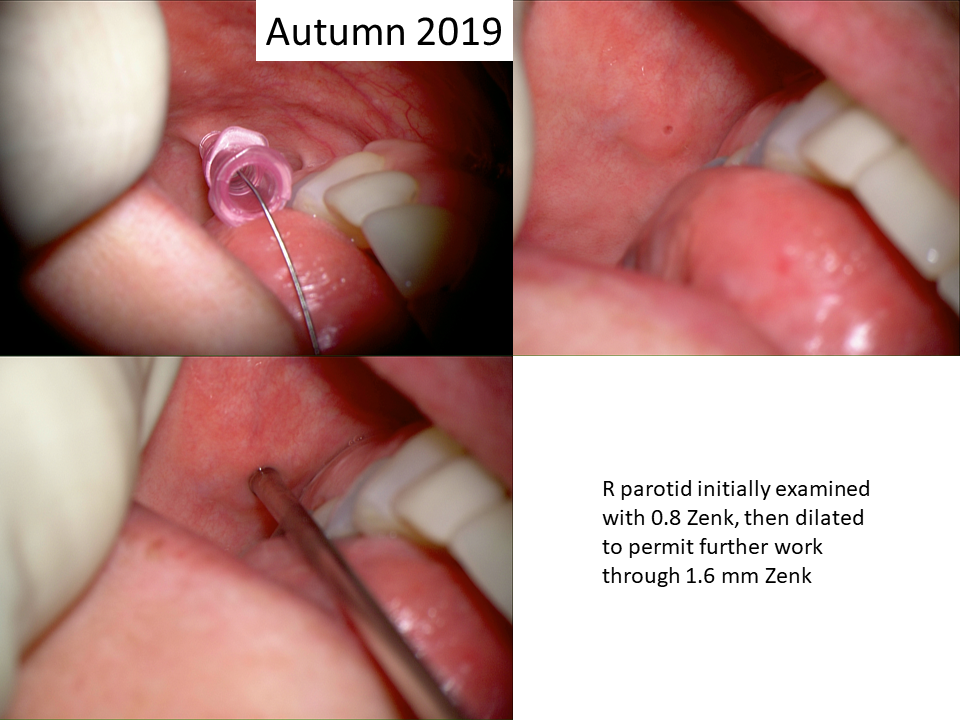
Autumn 2019 Op Note
Preop Dx: Sjogren's syndrome with bilateral parotid sialolithiasis and sialadenitis
Postop Dx: Same
Procedure: Right parotid sialodochoplasty (complex):
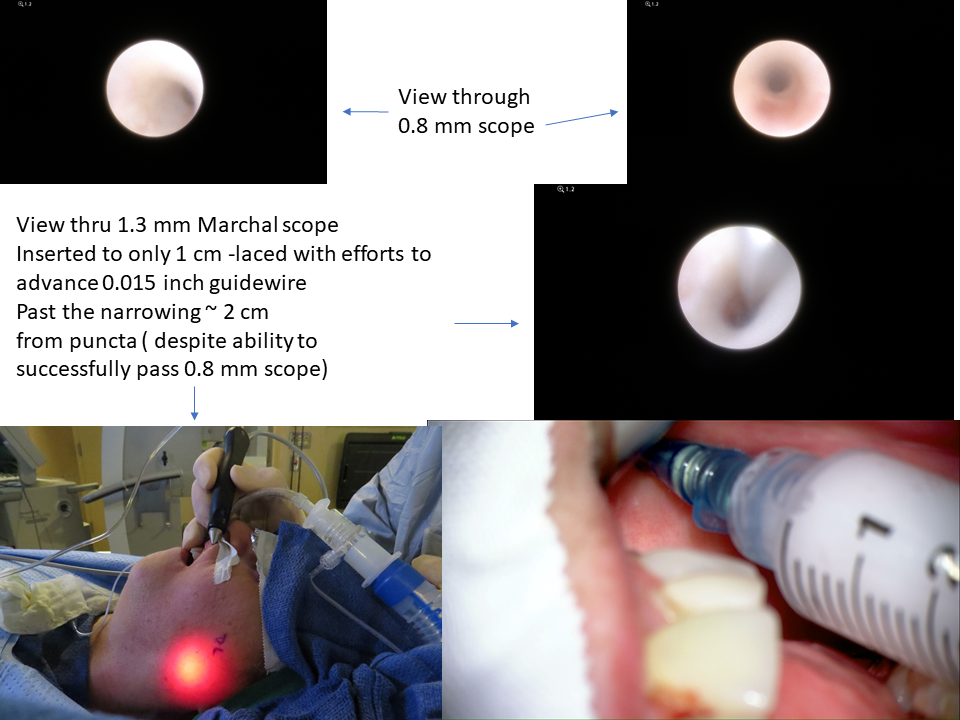
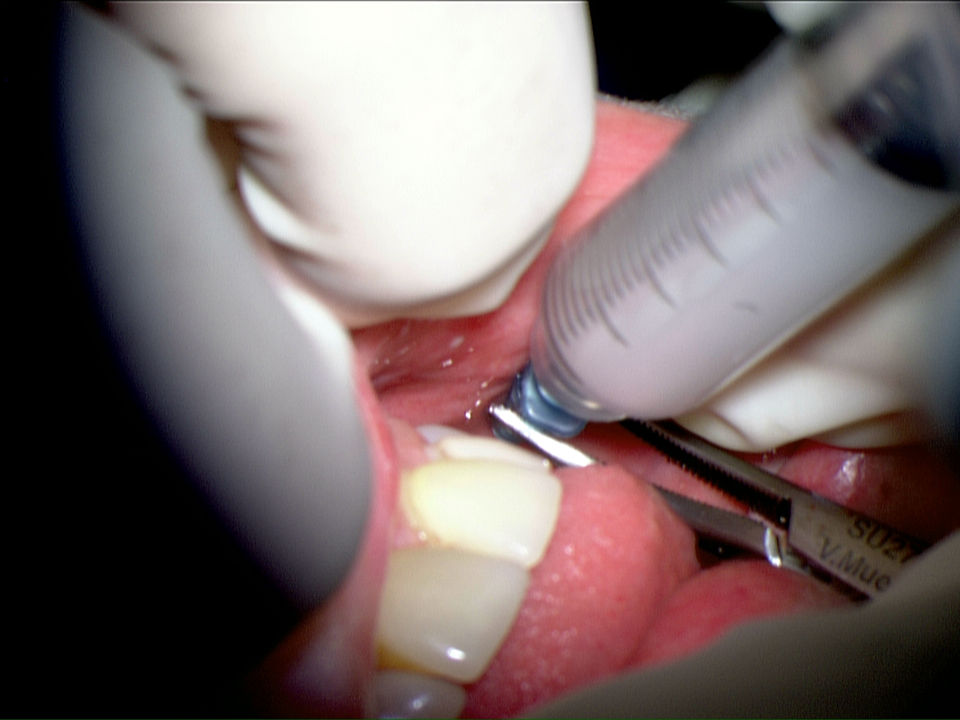
Ductal dilation with 24-22-20 angiocaths (seldinger technique over guidewire) followed by sialendoscopy with 0.8 mm Zenk scope then dilation with marchal dilators x 2 over 0.015 inch guidewire followed by 1.6 mm Zenk sialendoscopy with stone fragmentation (Ho:YAG laser 3.0 watts, 5 cps total of 0.15 killi-joules) and removal with forceps/basket/massage of gland followed by 5 cc of Kenalog 10 infusion to gland.
Left parotid sialodochoplasty (complex):
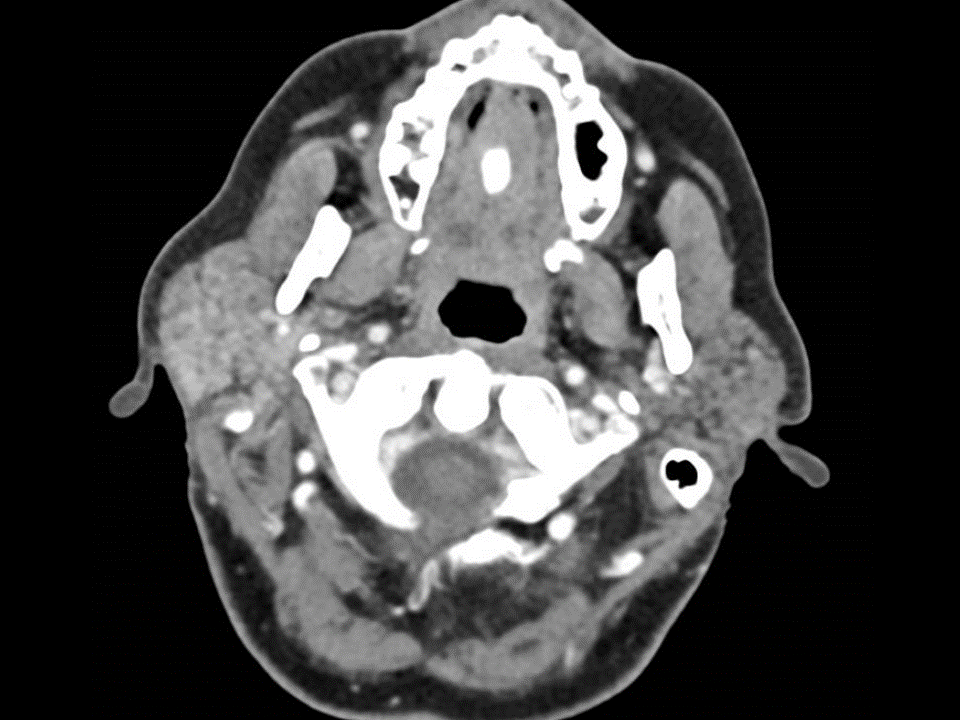
Distal ductal dilation (only to 2 cm) with 22 angiocath then small marchal (seldinger technique over 0.015 inch guide wire) unable to pass the guidewire further - with successful navigation of 0.8 mm Zenk sialendoscope to ~ 5 cm (hilum of gland - see photos) without encountering stone (reference to CT shows it intraparenchymal)
With inability to pass 1.3 mm Marchal scope past 2 cm with use of guide wire unable to pass beyond ~ 3 mc. Followed by 5 cc of Kenalog 10 infusion to the gland




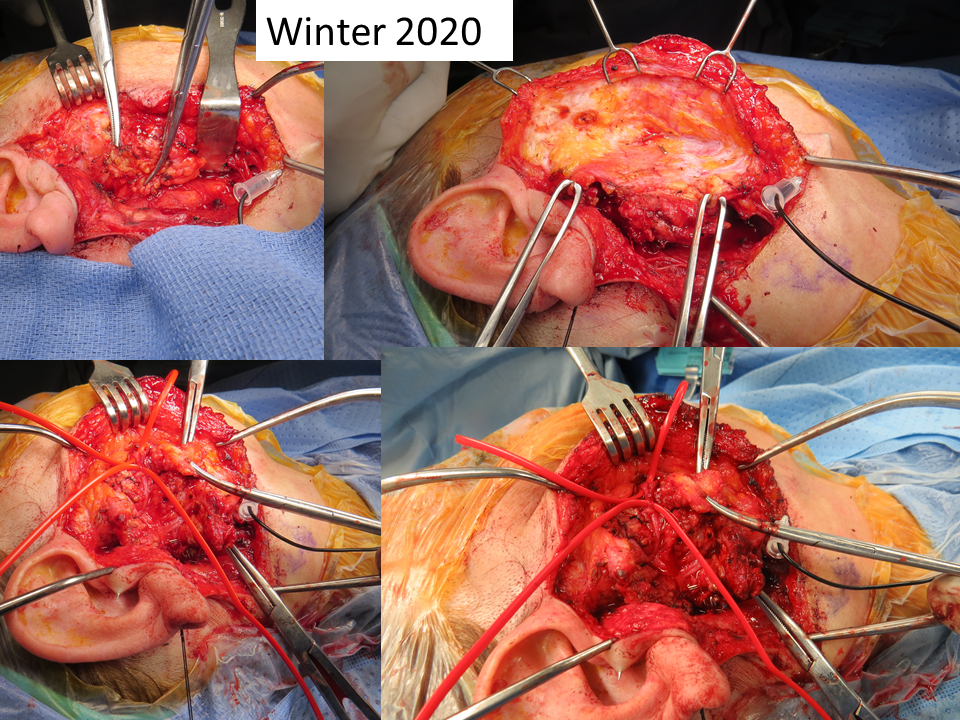
Winter 2020 Op Note
Preop Dx: Sjogren's syndrome with sialadenitis and ductal stricture (left parotid) and sialolithiasis (right parotid)
Postop Dx: Same
Procedure:
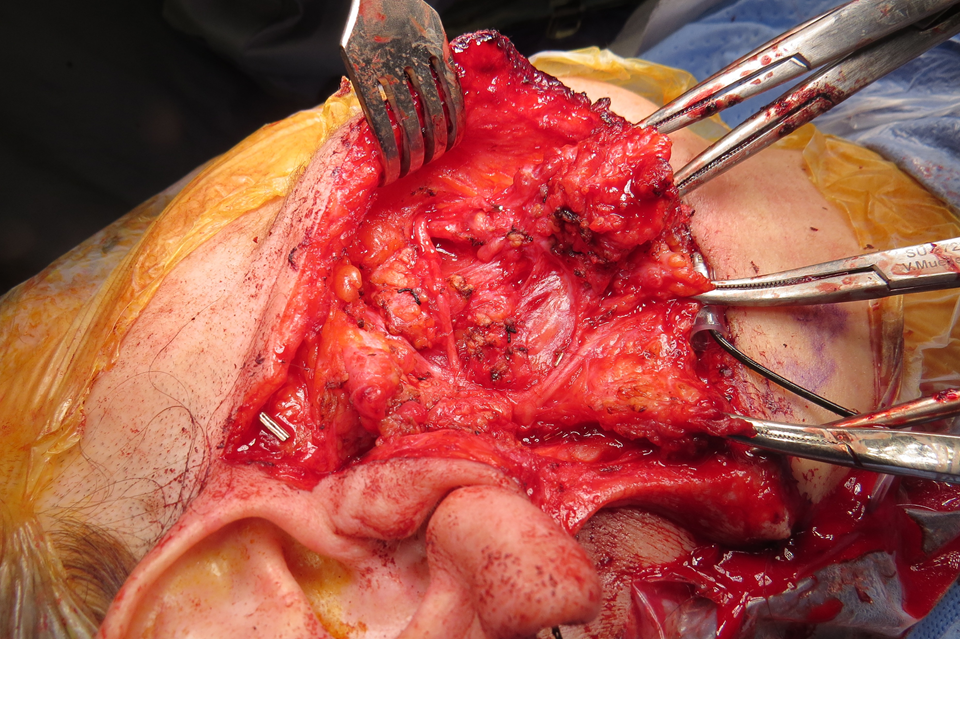
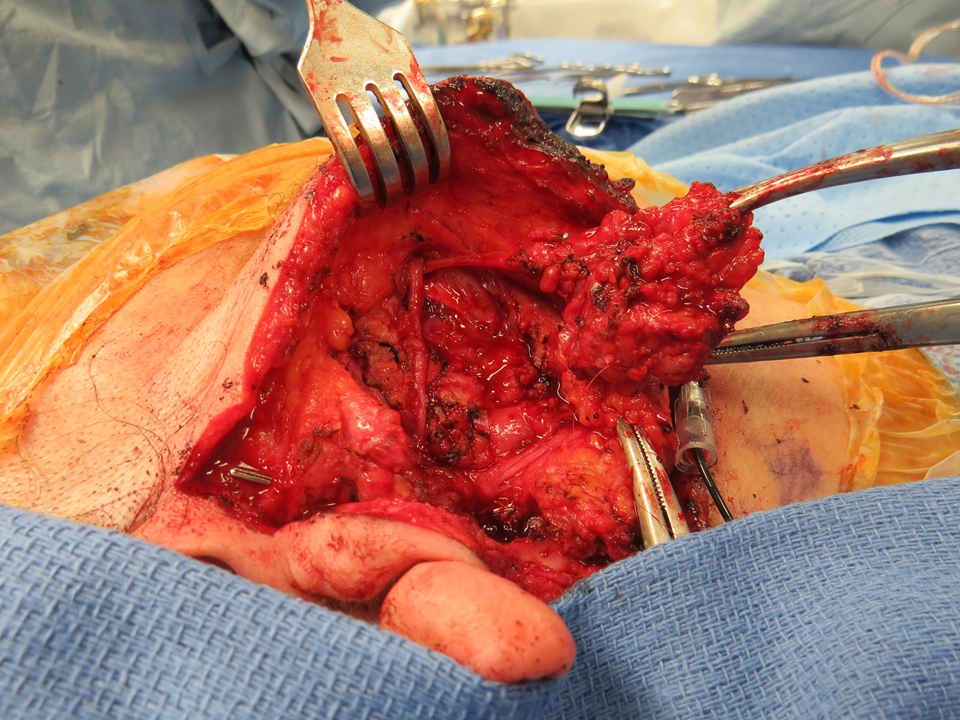
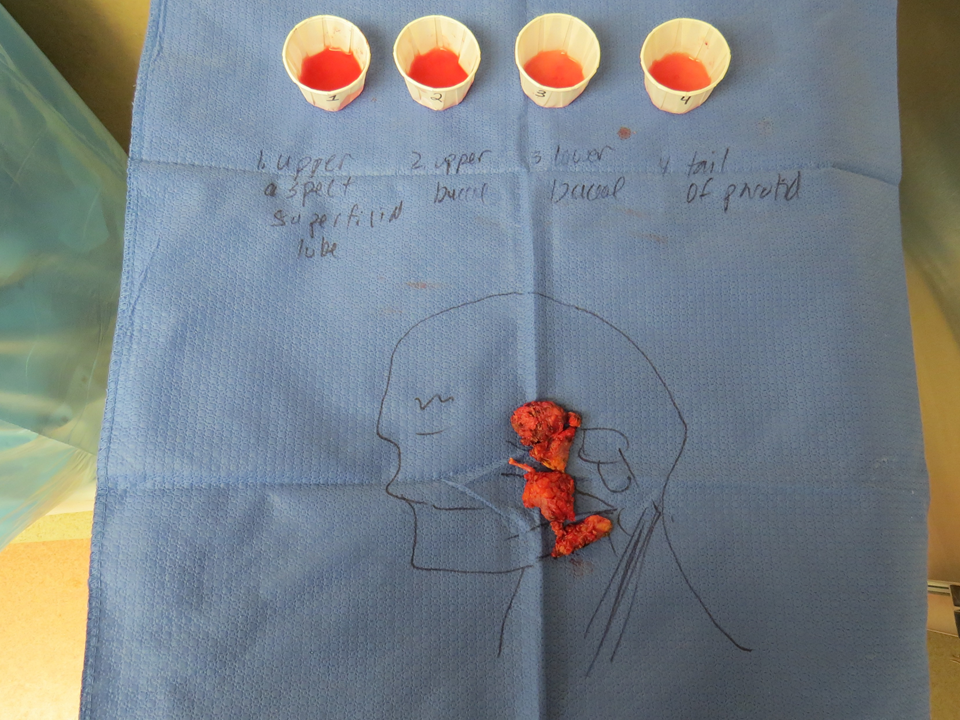
Right parotidectomy with facial nerve dissection and stone removal
Left parotid sialodochoplasty (sialendoscopy with distal duct dilation and kenalog 10 (3 cc) infusion)
Anesthesia: General OETT
Findings:
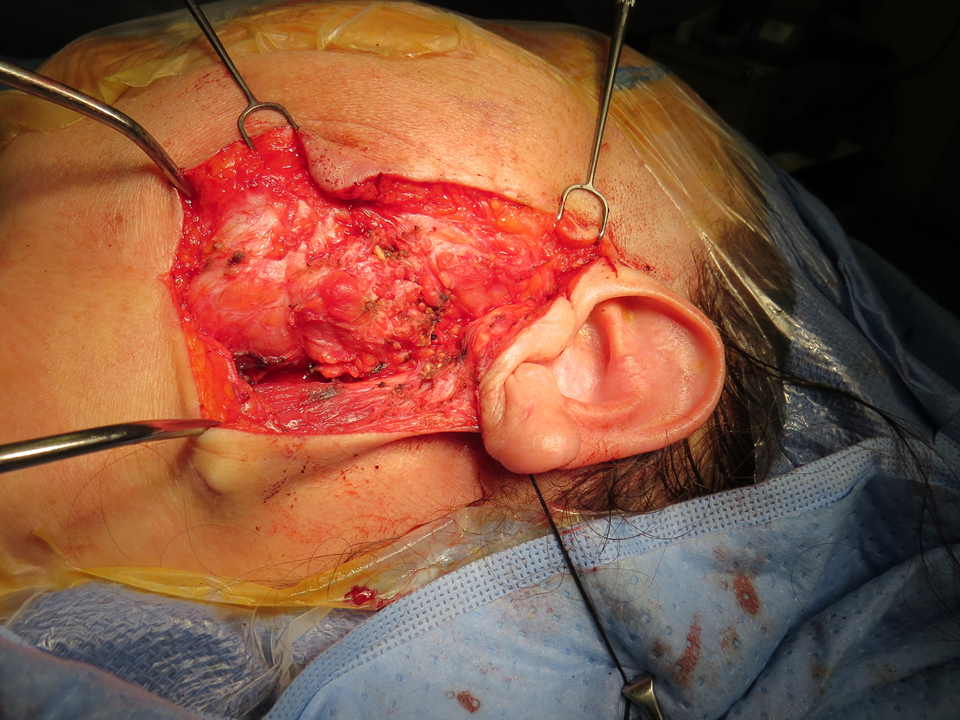
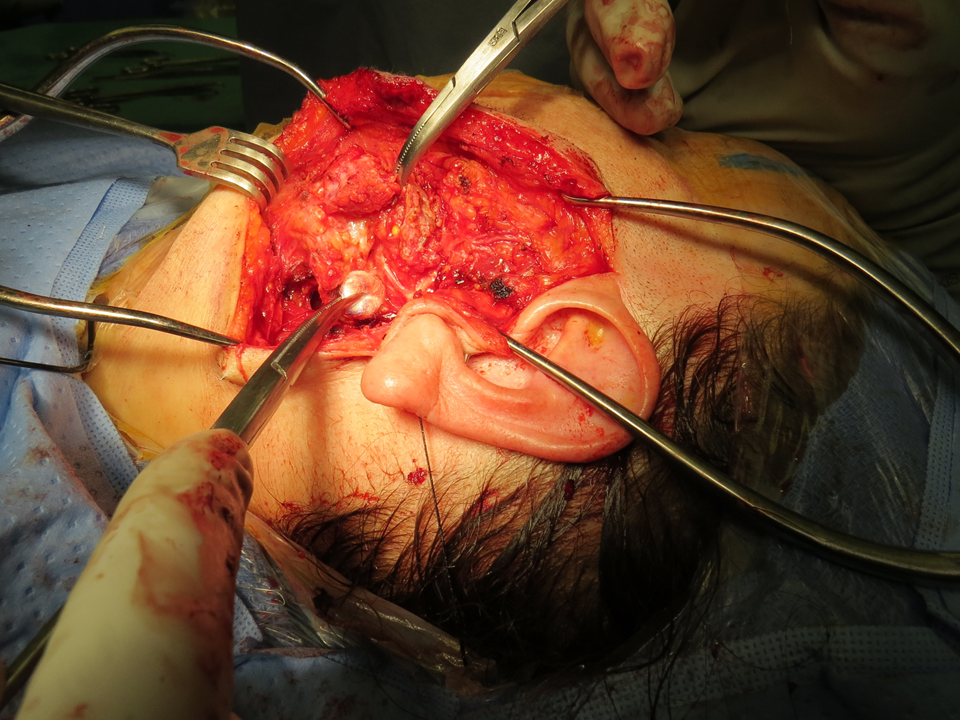
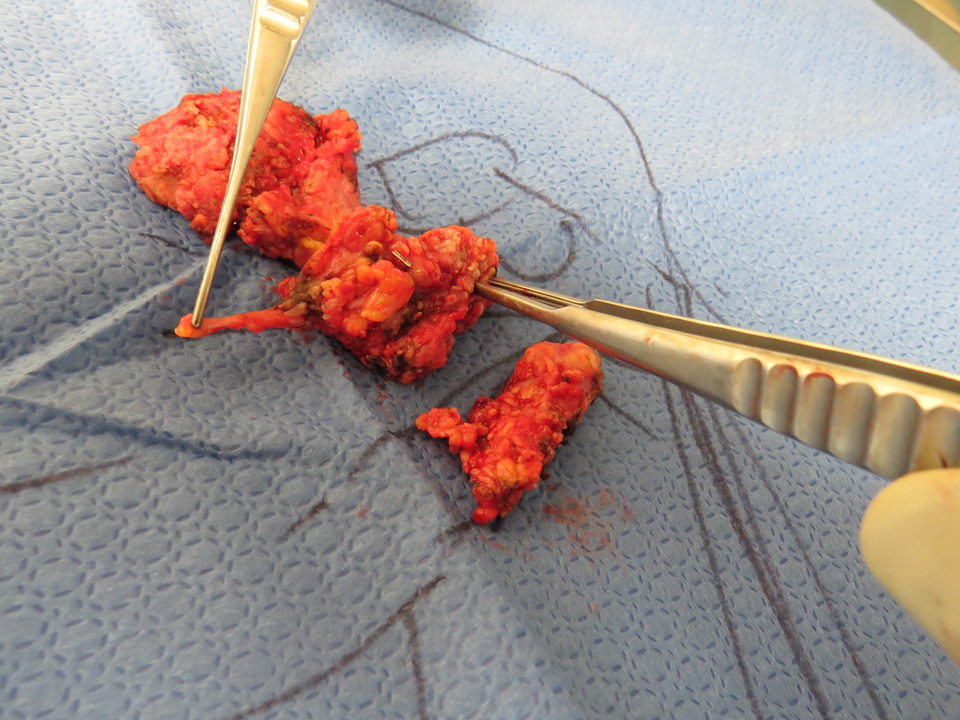
Right parotidectomy:
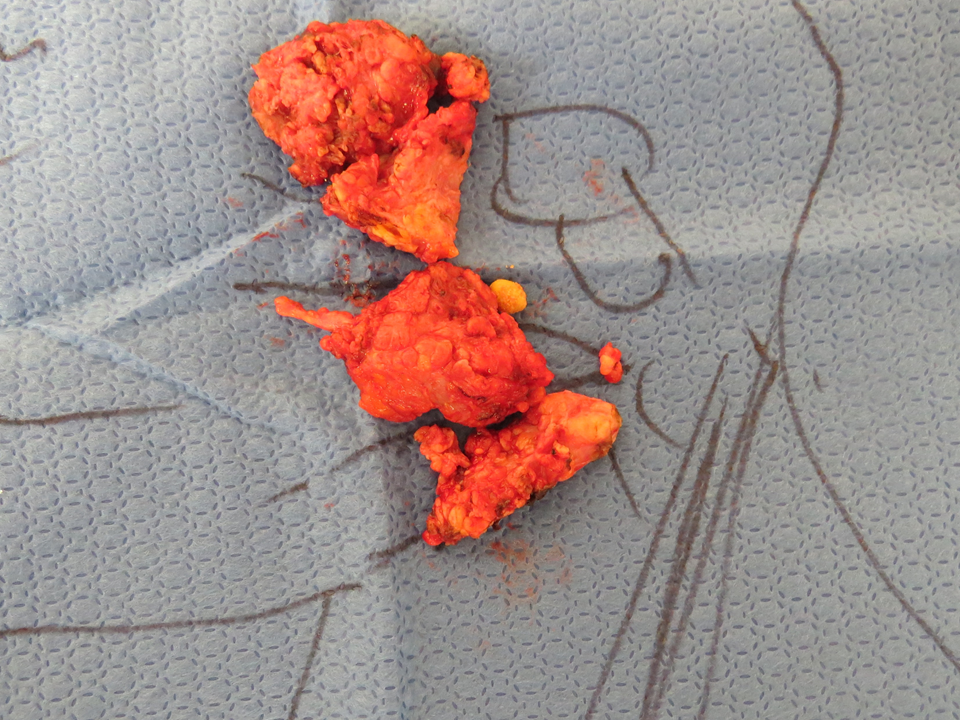
Scarred and inflamed right parotid c/w dx of sjogrens and chronic sialadenitis with stone identified and removed with 2 hemoclips placed on the distal (under buccal branch in proximal buccal space) - see photos below (7 mm stone)
Scapel dissection of buccal branch off the duct/stone complex with manipulation of buccal branch requiring vascular loops to mobilize it - with inability to stimulate buccal branch but stimulation at trunk did not identify a deficit
Facial nerve stimulated successfully (Checkpoint) at base of main trunk at 0.5 mV 80usec pulse
Left parotid sialendoscopy, distal duct dilation from 24 to 22 to 20 gauge angiocath (unable to get 18 in) - with second to smallest Marchal dilator used to ~ 1.5 cm. Able to 'hub' the 22 gauge (and 20) angiocath for delivery of 3 cc of kenalog 10 at the end of the procedure but unable to navigate past a very tight stricture that permitted advancing 0.8 mm Zenk scope to only 15. - 2 cm.







Summer 2020 Op Note
Preop Dx: Sjogrens syndrome, left parotid sialolithiasis and sialadenitis
Postop Dx: Same
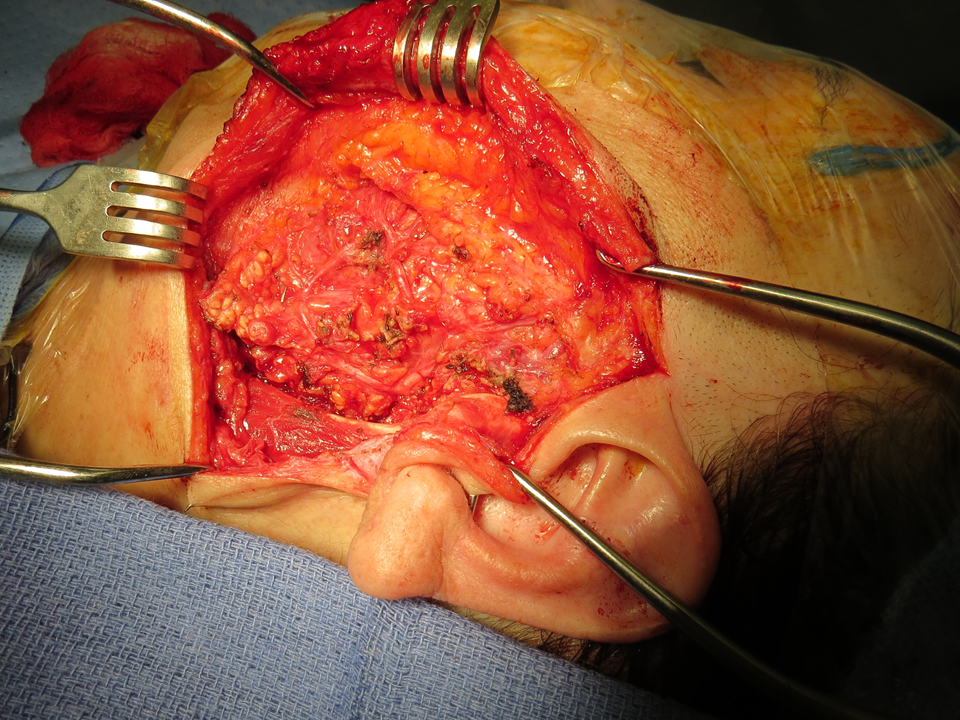
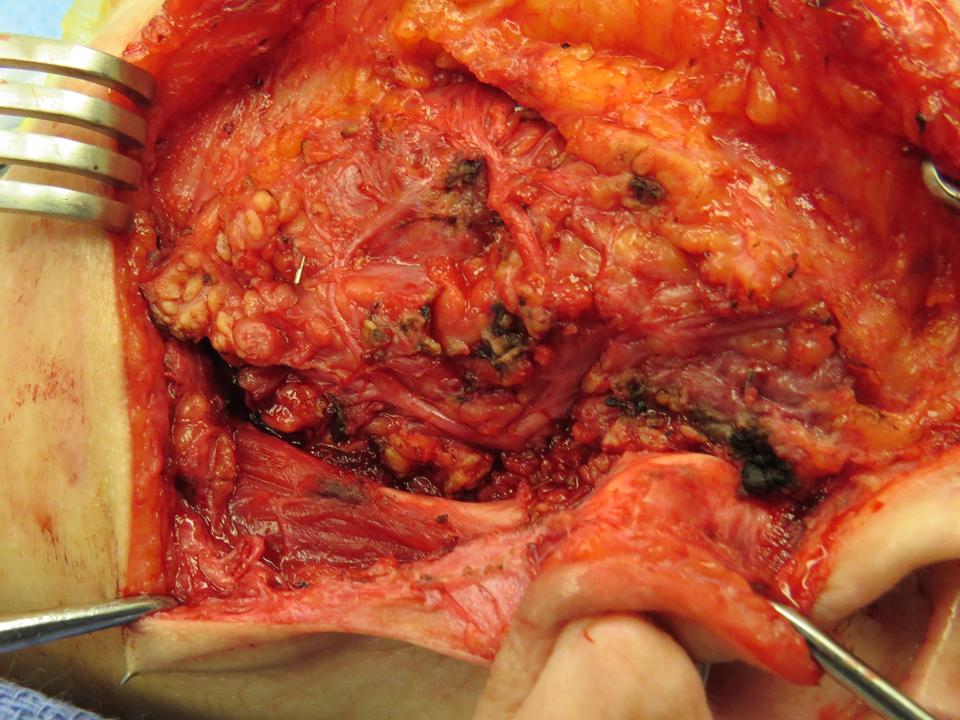
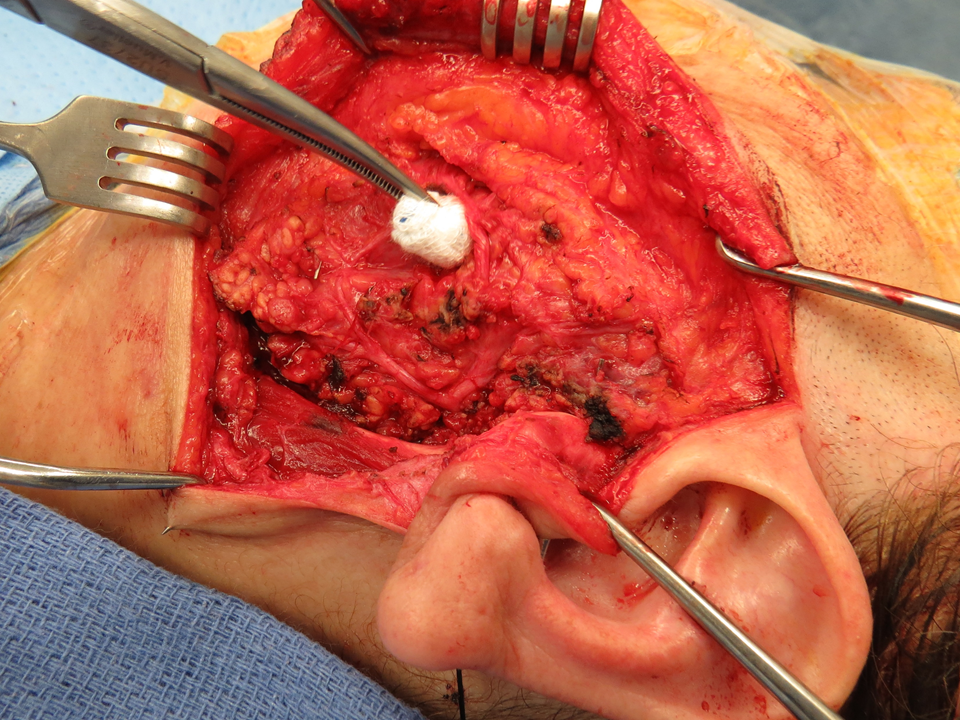
Procedure: Left parotidectomy with facial nerve dissection; use of NIMS facial nerve monitoring and check point nerve stimulator (full face stimulated with trunk stimulation with checkpoint 0.5 mamp 100 microsecond pulse)
Anesthesia: General OETT
Findings: markedly scarred swollen left parotid with dense scarring about hilum adjacent stone
Duct identified an ligated (hemoclip) anteriorly after mobilizing buccal branch of facial nerve to isolate duct over anterior-mid portion of masseter











