

Return to: Sialograms and Sialography; Normal Submandibular Sialogram Sequence
History:
Right submandibular swelling prompted by smelling or eating food lasting for 2-3 hours was a discomfort beginning 4 months before the sialogram
Sialogram Procedure Note (Modified):
Procedure: Right submandibular duct cannulation dilation with radiocontrast insufflation (Isovue 370®)
Preop Diagnosis: Right submandibular sialadenitis possible ductal stricture
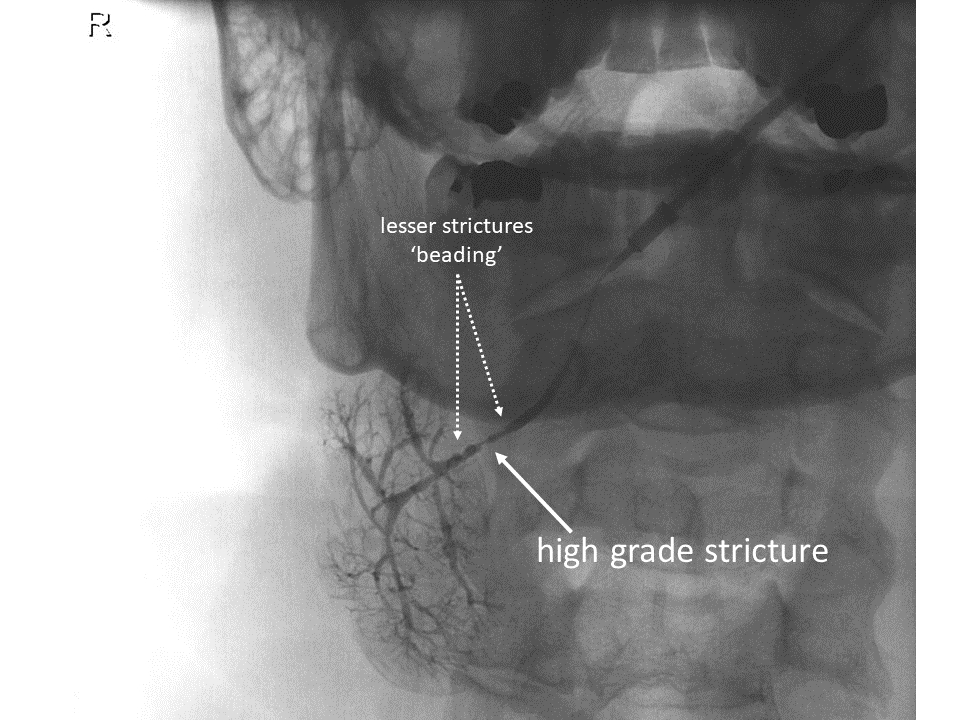
Postop Diagnosis: Right submandibular duct stricture 1-1/2 cm distal to the gland hilum
Anesthesia: Topical 2% viscous lidocaine to the floor of mouth, augmentin 875 mg po bid beginning the morning of the sialogram (instucted to come in well fed and well hydrated, not NPO)
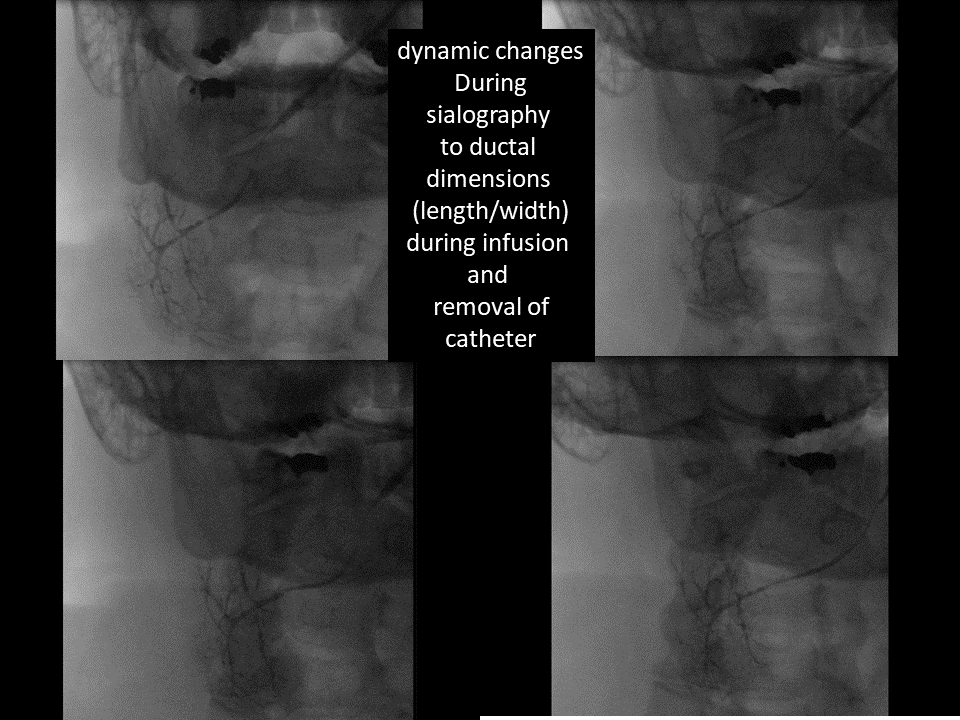
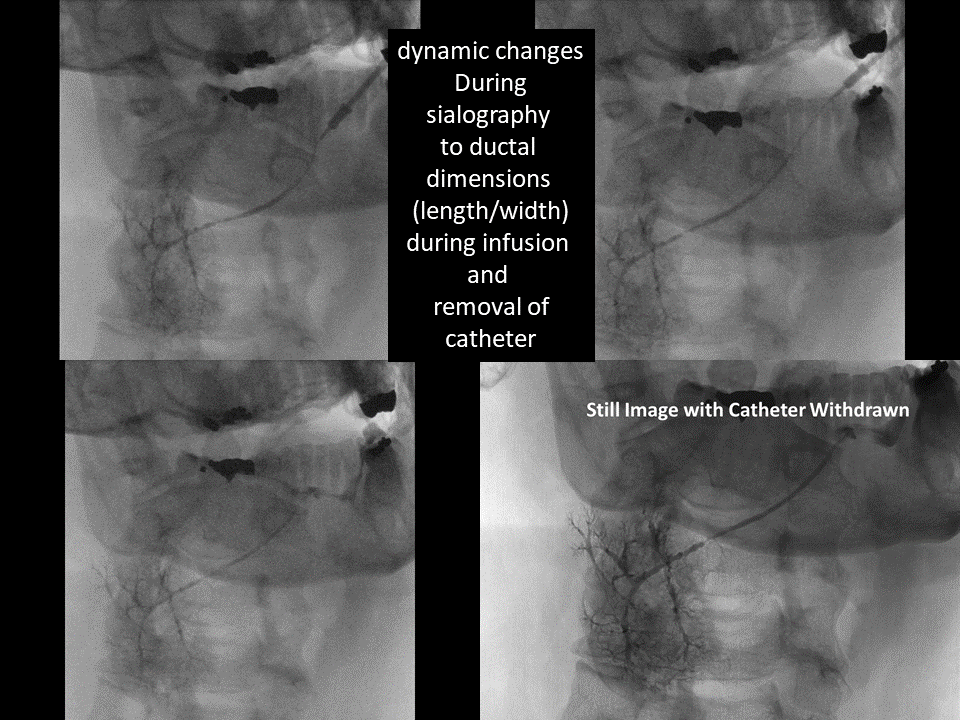
Description of Procedure: Following identification the patient informed consent and a brief timeout in the fluoroscopy suite with him positioned supine and the microscope employed at the head of the table the oral cavity was inspected with the tongue touching the roof of the mouth allowing for ready view of both submandibular distal duct orifice ease with the need to use the Turner needle to slightly enlarged the right submandibular duct orifice to accommodate a 0.015 inch guidewire over which through the Seldinger technique a 22-gauge Angiocath was readily placed and held with rapid egress of clear saliva filling the hub allowing for placement of IV tubing primed with Isovue-370 to initially instill 1/2 cc without discomfort and ultimately 3 cc in the course of the examination employing video imaging for assessments of dynamics during infusion and removal of catheter.
Radiology Report:
Indication: Sialoadenitis, unspecified. Evaluate patient with a right sided sialogram.
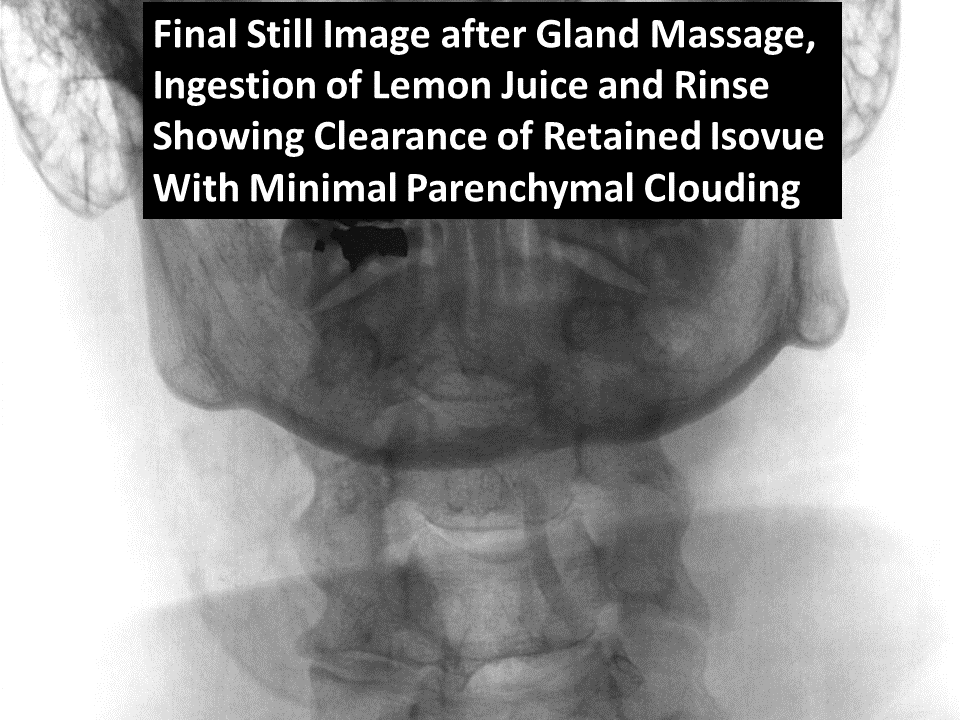
Technique: Dr. Hoffman was present and performed cannulation of the submandibular duct opening. After successful cannulation was achieved, a 10 cc syringe with Isovue 370 contrast agent was connected to the cannula and instilled into the duct under fluoroscopic monitoring. A total of 3 cc of contrast agent was utilized. After adequate duct opacification was achieved, AP and lateral spot films were obtained. The cannula was then removed and duct was allowed to empty following oral administration lemon juice to patient. Post void image was then obtained.
Fluoro Time: 108 seconds
Radiation Dose: 585.68 uGy-cm2
Findings: Adequate opacification of the submandibular duct and branches is achieved. High-grade proximal duct stricture with mild dilation and increased intraglandular arborization of the submandibular gland. Post void film shows adequate emptying with faint contrast remaining within the gland or duct system.
Impression: High-grade proximal duct stricture with mild dilation and increased intraglandular arborization of the submandibular gland.
Follow-up
1. Six months after sialogram clinic visit: "Total relief of symptoms following sialogram" for period (unspecified) after sialogram but recurrence of swelling 'comes and goes, not as bad' warranting request for intervention
2. Nine months after sialogram in-clinic procedure (microscope room): "Mild swelling and pain than prior to sialogram" but sufficient to request procedure
Modified Procedure Note:
Procedure: Right submandibular duct cannulation dilation with Kenalog-10 insufflation
Preop Diagnosis: Right submandibular duct stenosis with sialadenitis
Postop Diagnosis: Same
Anesthesia: Premedication with augmentin 875 mg po bid for three day course beginning morning of procedure, 2% viscous lidocaine applied to the floor the mouth
Description of Procedure: Following identification the patient informed consent and a brief timeout with him supine the microscope brought in from above his head the oral cavity was examined showing a widely patulous left submandibular duct orifice through which clear saliva readily expressed but difficulty initially and even identifying the duct orifice on the right allowing for manipulation without any saliva seen emanating from it injection to use the Turner needle to enlarge the duct orifice with several attempts leading to placement of a 0.015 months guidewire cannulating the duct over which modified Seldinger technique a 24-gauge gauge Angiocath was placed with 3 cc's of Kenalog 10 instilled into the gland and left 'hubbed' for 3 to 4 minutes.
The 0.015 inch diameter guidewire was replaced through the 24-gauge Angiocath with removal of the 24 gauge angiocath permitting retention of the guidewire over which a 22-gauge Angiocath placed to further dilate the duct orifice which, on removal, permitted massage of the gland demonstrating egress of infused Kenalog-10
He tolerated the procedure well identifying that the intensity of the discomfort during insufflation was similar to that which he experienced yesterday with eating and was identical in location and other qualities that which he had experienced previously
3. 15 months after sialogram clinic visit: Even more improvement of symptomatic swelling and discomfort of the submandibular gland following the steroid infusion 'took care of it completely for 4 to 5 months' but over the past several months some twinges making him feel it was returning therefore requesting repeat gland ductal dilation with steroid infusion.
4. 17 months after sialogram in-clinic procedure (microscope room):
Modified Procedure Note:
Procedure: Right submandibular duct cannulation dilation with Kenalog-10 insufflation
Preop Diagnosis: Right submandibular duct stenosis with sialadenitis
Postop Diagnosis: Same
Anesthesia: Premedication with augmentin 875 mg po bid for three day course beginning the morning of the procedure as well as 2% viscous lidocaine applied to the floor the mouth
Description of Procedure: Following identification the patient informed consent and a brief timeout with him supine the microscope brought in from above his head neuro cavity was examined showing a widely patulous right submandibular duct orifice through a 0.015 months guidewire successfully cannulated the duct.
Over which the Seldinger technique a 22-gauge gauge Angiocath was hubbed and 4cc's of Kenalog 10 instilled into the gland with a clamp feeling for medicine large but well-tolerated without pain with accompanying fullness of the right submandibular gland developing - leaving the angiocath hubbed for 3 minutes
He tolerated the procedure and was observed in clinic before discharge
5. 23 months after sialogram clinic visit: absence of swelling or pain - doing well
Exam: right submandibular gland nontender but slightly firmer than left with only minimal saliva expressivel from left submandibular duct but not the right
Targetted f/u in one year with ultrasound - earlier if symptomatic with discussion re: options
a. repeat dilation steroid infusion in clinilc
b. open ductoplasty (if above unsuccessful) in operating room with sialoballoon dilation
c. botulinum toxin injection to gland (see: Botulinum Toxin Treatment for Sialadenitis (OnabotulinumtoxinA - Botox®) (IncobotulinumA - Xeomin®) and (AbobotulinumtoxinA - Dysport®) Salivary Swelling)
d. submandibular gland removal