






click on image above to enlarge; advance with cursor over border
see images of surgical procedure at bottom of page -Provided by Dr. Douglas K Henstrom MD University of Iowa Facial Plastic and Reconstructive Surgeon, Director of Facial Nerve Center
return to: Reconstructive Procedures Protocols or Nerve Grafting for Facial Paralysis (Cross Face Nerve Grafting)
GENERAL CONSIDERATIONS
- Indications
- Segmental loss of a motor or sensory nerve with viable distal and proximal segments accessible for grafting.
- Facial reanimation with cross-face nerve grafting (see also: Facial Reanimation)
- Contraindications
- Absence of viable motor units in the end organ is a contraindication to motor reinnervation procedures. The assessment of this may be assisted with electromyography and potentially muscle biopsy.
- Patients who require intact foot and lower leg sensation for sports or employment situations should be considered for an alternative donor site.
- Peripheral neuropathy with existing compromise of sensation to the lower extremity
- Pertinent Anatomy
- The sural nerve is a sensory nerve of the lower lateral leg and lateral aspect of the foot.
- The nerve is comprised of spinal nerve roots from S1 and S2.
- In the posterior calf, the sural nerve emerges from between the two heads of the gastrocnemius muscle and runs with the small saphenous vein inferiorly to curve under the lateral malleolus.
- In the area of the lateral malleolus, the nerve divides into several branches that run over the lateral foot. The branching pattern may be variable.
- The nerve may be harvested as a vascularized nerve graft within the cutaneous paddle of a fibula free flap and is often identified during skin paddle dissection of the fibula flap.
PREOPERATIVE PREPARATION
- Evaluation
- Exclude history of trauma to lateral lower leg
- Potential Complications
- Patients should be aware of anesthesia of lateral calf and dorsum of foot following the procedure.
- The incision scar may be undesirable to some patients and an alternative donor site should be chosen.
- Temporary ankle stiffness and edema of foot.
- Poor healing and infection are possible.
NURSING CONSIDERATIONS
- Room Setup
- See Basic Soft Tissue Room Setup
- Instead of the Basic Soft Tissue Supply Pack, use the ENT Supply Pack
- Instrumentation and Equipment
- Standard
- Minor Instrument Tray, Otolaryngology
- Microsurgery Instrument Tray, Otolaryngology
- Retractor Tray, Small
- Operating Microscope with eye pieces opposite of each other.
- Standard
- Medications (specific to nursing)
- Antibiotic ointment
- Prep and Drape
- Standard prep, 10% providone iodine-circumferential from midfoot up to knee. Rollable stockinet over leg
- Drape
- Impervious drape under leg
- Towels around leg from upper thigh to ankle so the posterolateral aspect of the leg is accessible
- Split sheet around leg
- Drains and Dressings
- Antibiotic ointment to suture line
- Fluffs, Kerlix 4 in x 2, 6 in Ace wraps x 2; applied
ANESTHESIA CONSIDERATIONS
- Lateral lower extremity must be available for surgery: no a lines, TED hose, pneumatic stockings
OPERATIVE PROCEDURE
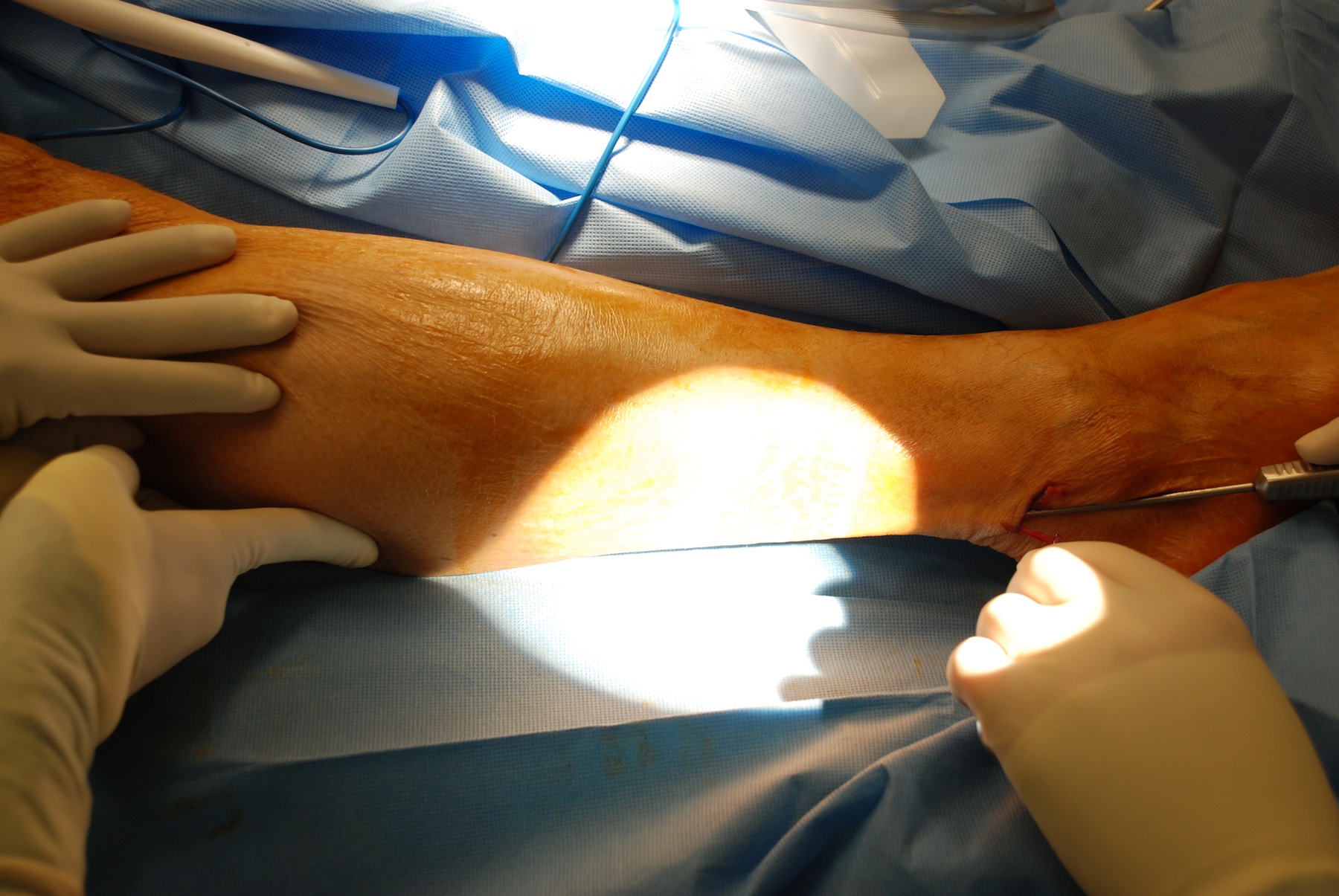
- The sural nerve is best identified approximately 2 cm posterior to the lateral malleolus and approximately 1-2 cm proximal. In this area, the nerve has not undergone significant branching. The nerve tends to be more posteriorly located than drawn in many texts.
- A horizontal incision is made in the region above. If the small saphenous vein is visible, the nerve or a branch of it will be medial to it.
- The nerve is traced proximally for as long a segment as is required. May use tendon stripper for this if needed.
- If a branching pattern is required for facial reinnervation, the nerve is traced distally and branch points are identified. Often, the nerve does not branch significantly until reaching the lateral aspect of the foot.
- A longitudinal incision over the nerve may be used rather than "stair step" transverse incisions to harvest the nerve with minimal trauma, if indicated.
- Of note, recent publications have supported endoscopic harvesting of the nerve with minimally invasive incisions.
- The nerve may be harvested under tourniquet control to minimize bleeding during dissection, but is not necessary.
- The nerve is cut proximally and distally with a new scalpel blade and placed on moist gauze.
- If a single segmental defect is to be grafted, the nerve is reversed at inset. This maximizes the number of useful tubules through which the new nerve will grow by minimizing the possibility that new nerve will ineffectually grow out through small branches that have been cut.
- The donor site is closed with deep sutures of 4-0 moncryl, and the skin is closed with running subcuticular 5-0 moncryl.

![A[1]](https://medicine.uiowa.edu/iowaprotocols/sites/medicine.uiowa.edu.iowaprotocols/files/wysiwyg_uploads/A%5B1%5D.png "A[1]")






ENDOSCOPIC NERVE HARVEST
- Horizontal incision about 2 cm in length and about 1 cm above and behind the lateral malleolus, through skin and sub q.
- Identify saphenous vein, and should find sural nerve immediately posterior to vein.
- Place vessel loop around nerve and retract slightly.
- Spread up and down nerve to create more space for pocket for rubber doughnut portion of endoscope.
- Endoscope inserted with cone tip on end.
- Run Endoscope up nerve, keeping it in view the entire time. Can feel the back of the leg and direct the muscle and the nerve. Go up and make mark on leg at end of where you want to go.
- Now leg must be inflated (between 12-15 pressure). This requires are tight seal with rubber stopper. Endo harvester and guillotine now inserted into scope. Harvester is place around nerve and slid up and down to free it 360 degrees around all up and down
- Branches and proximal end must be cut with the guillotine and then nerve pulled out down incision.
- Hook up a small syringe with saline to one port to give a little irrigation if needed when inflating and working in the leg
POSTOPERATIVE CARE
- The donor leg should be elevated when the patient is sitting or in bed for several days.
- Antibiotic ointment is applied to the incision.
REFERENCES
Coert JH, Dellon AL. Clinical implications of the surgical anatomy of the sural nerve. Plast Reconstr Surg. 1994;94:850-855.
Ortiguela ME, Wood MB, Cahill DR. Anatomy of the sural nerve complex. J Hand Surg Am. 1987;12:1119-1123. (vm)
Hadlock TA, Cheney ML. Single-incision endoscopic sural nerve harvest for cross face nerve grafting. J Reconstr Microsurg. 2008 Oct;24(7):519-23. Epub 2008 Sep 16.