
return to: Paranasal Sinus Surgery Protocols or Anterior Craniofacial Resection with Formal Anterior Bifrontal Craniotomy
see also: Cranioplasty
GENERAL CONSIDERATIONS
- Indications
- The anterior pericranial and galeofrontalis flaps have been used extensively for anterior skull base and craniofacial reconstruction.
- Use of this flap is not limited to open resections - it has been advocated for selected endoscopic resections (Giurintano et al. 2021).
- These flaps may be turned inward to separate the intracranial contents from the sinonasal cavity.
- The flap may be extended posteriorly to yield a length that will easily reach the central skull base.
- Contraindications
- Previous forehead surgery with likely interruption of the blood supply of the flap tissues may be a contraindication.
- Previous radiation to the donor site is considered a relative contraindication.
- Because the major blood supply to the anterior pericranium and galea is via the supratrochlear and supraorbital vessels (which derive from the ophthalmic artery), in cases that require orbital exenteration a broad-based flap should be harvested. The flap in these cases should include the contralateral supraorbital and supratrochlear vessels, as well as the ipsilateral frontal branch of the superficial temporal vessel if possible.
- Pertinent Anatomic Considerations
- The galea forms the aponeurotic system between the frontalis and occipitalis muscles. Laterally, it is continuous with the temporoparietal fascia, which is a continuation of the SMAS (superficial muscular aponeurotic system) inferiorly.
- The frontal branch if the facial nerve lies within the temporoparietal fascia. Therefore, anteriorly when lateral to the temporal line, dissection should be done bluntly, raising the temporoparietal fascia with the frontal branch up off of the deep temporalis fascia.
- From superficial to deep, the layers of the scalp are: skin, subcutaneous tissue, galea, subgaleal fascia, and pericranium.
- The anterior pericranium and galea receive their blood supply from the supraorbital and supratrochlear vessels. Both of these vessels are terminal branches of the ophthalmic artery. The more lateral galea receives some blood supply from the frontal branch of the superficial temporal artery.
- The supraorbital and supratrochlear vessels divide into superficial and deep branches. The superficial branches enter the frontalis muscle and emerge to run on the surface of the galea. These branches enter the subcutaneous tissue approximately 3.5 cm above the orbital rim (supratrochlear) and 5.5 cm above the orbital rim (supraorbital). Therefore, the axial blood supply to the galeofrontalis is approximately 5 cm above the orbital rim.
- The deep branches run under the frontalis and galea within the subgaleal fascia (this layer may be considered a component of the pericranium). The deep branches pursue an axial course for approximately 1.5 to 4 cm above the supraorbital rim. There are many penetrating vessels that connect the superficial and deep branches. These vessels are divided if the galea is separated from the underlying pericranium.
- Experience suggests that the effective axial blood supply to these tissues may extend farther than is demonstrable in anatomic studies. By elevating the pericranium with the galeofrontalis tissue as a single unit, the most robust flap is obtained because the communicating vessels between the deep and superficial vessels are preserved.
- The galea forms the aponeurotic system between the frontalis and occipitalis muscles. Laterally, it is continuous with the temporoparietal fascia, which is a continuation of the SMAS (superficial muscular aponeurotic system) inferiorly.
PREOPERATIVE PREPARATION
- Evaluation
- If there is any question regarding the patency of the anterior blood supply to the intended flap due to previous trauma or surgery, the vessels may be localized and traced out using a Doppler in the clinic.
- Potential Complications
- Vascular failure and necrosis of the flap is the most serious complication. The tissues of the flap should be handled with extreme care during harvest. Dissection in the region of the supraorbital rims should be done carefully so as not to disrupt the blood supply.
- Alopecia in the area of flap harvest when a galeal flap is elevated may be a problem. It is most common along the incision line of the coronal flap.
- Injury to the frontal branch of the facial nerve is a potential complication.
- If the patient is going to be radiated following surgery, breakdown of skin in the frontal area following harvest of a galeofrontalis flap can occur. Metal burr-hole covers should not be used under the skin in the area under the galeal harvest, as this may result in hot spots over which radiation injury to the skin is more likely.
NURSING CONSIDERATIONS
- Room Setup
- Instrumentation and Equipment
- Standard
- Special
- Varidyne vacuum suction controller
- Nerve stimulator control unit and instrument
- Halsted microline artery forceps, curved
- Fine needle tip cautery
- Medications (specific to nursing)
- 1% lidocaine with 1:100,000 epinephrine
- Antibiotic ointment
- Prep and Drape
- Standard prep, 10% providone iodine
- Drape
- Head drape
- Towels to square off incision line
- Plastic drape (1010 drape) to cover nose and mouth
- Split sheet
- Drains and Dressings
- Varidyne vacuum suction drain: 7 mm or 10 mm, x 2
- Antibiotic ointment to suture line (see Antibiotic Prophylaxis in Head and Neck Surgery protocol)
- Special Considerations
- Possibility of skin graft (see Skin graft protocol)
- If calvarium harvested, order:
- Dissection of the galeal flap requires separation of the overlying subcutaneous tissue from galea, and identification of the frontal branch of the facial nerve. If the flap is carried laterally, this is greatly facilitated with the use of loupe magnification.
- Lumbar drain may be placed prior to procedure; discuss this with the Neurosurgery Service.
- The patient is supine and positioned on a Mayfield headrest.
- For intracranial procedures, the scalp is prepped per the Neurosurgery Service preference, and neurosurgical instruments are ordered.
- If the ablative procedure does not require intracranial exposure, the scalp is not shaved. The scalp and hair are prepped with Betadine solution (not Betadine soap). The hair is parted along the intended incision line and collected up in rubber band pig-tails.
- A sterile towel is stapled to the scalp just posterior to the intended coronal incision.
- Tarsorrhaphy stitches are placed to protect the cornea.
ANESTHESIA CONSIDERATIONS
- General
- General anesthesia is used with potential considerations for an intracranial procedure.
- The head of the bed is turned 180° from the anesthesiologist, and long anesthesia tubing is required.
- Specific
- No paralysis until after the frontal branch of facial nerve is identified and protected if necessary.
OPERATIVE PROCEDURE-PERICRANIAL FLAP
- If additional length of the pericranial flap posterior to the coronal incision is needed, care must be taken in making the coronal incision so that the pericranium is not divided. The additional extension of pericranium is dissected before elevating the coronal flap anteriorly. Be sure that the person making the coronal flap incision is aware if this will be necessary.
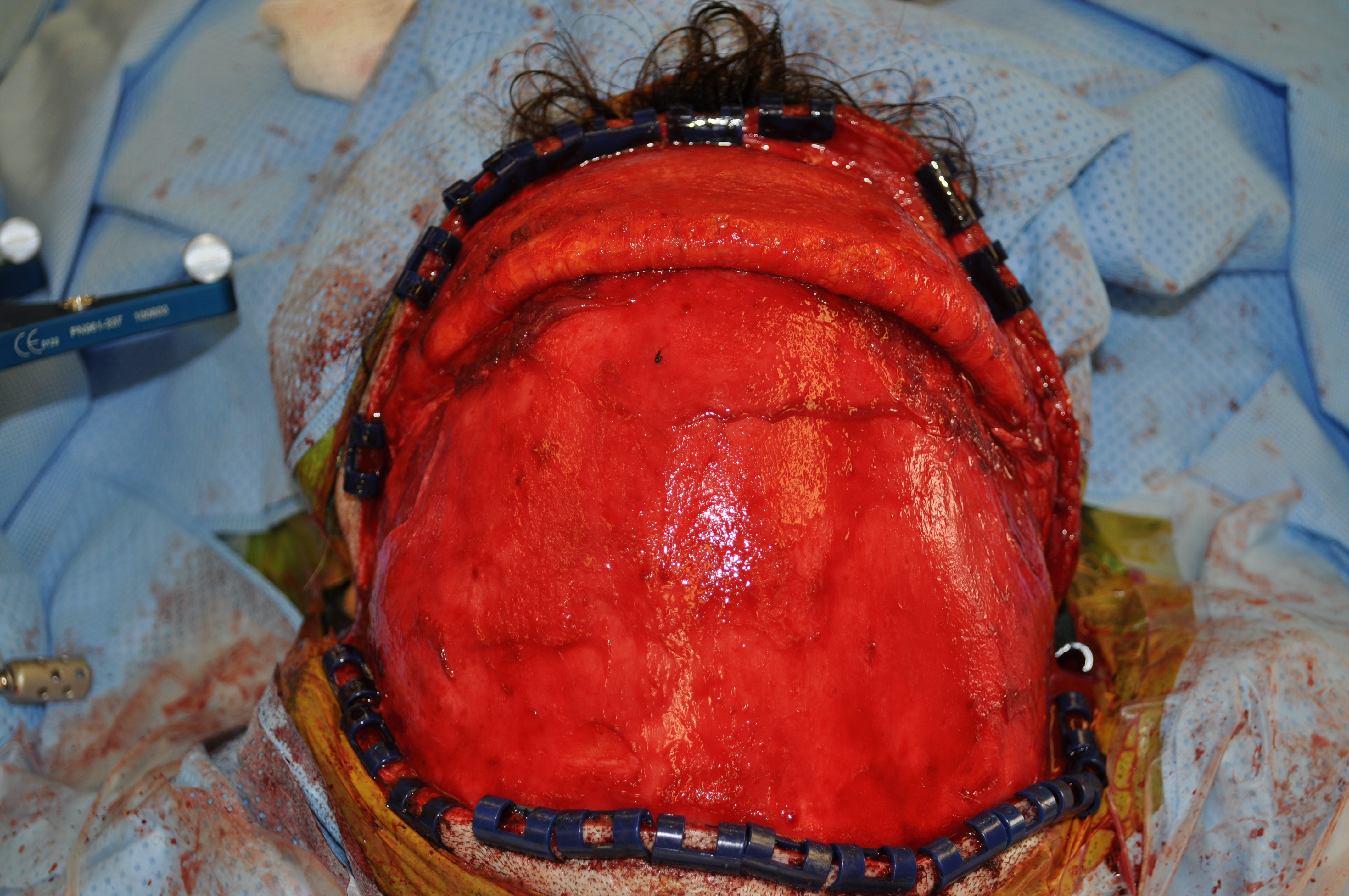
- Once the coronal incision has been made, the plane between the subgaleal fascia and overlying galea is identified.
- The coronal flap is then elevated anteriorly in this plane superficial to the subgaleal fascia component of the pericranium.
- Laterally, the pericranium is incised along the temporal lines for anterior flaps.
- Laterally as the galea is elevated, the frontal branch of the facial nerve should be elevated within the galea.
- Anteriorly and inferiorly, the galea should be separated from the underlying pericranial flap toward the supraorbital rims only as far as needed to obtain adequate length of the flap for inset. Minimal separation of the galea and pericranium in the low forehead region will preserve communicating branches between the deep and superficial vascular systems and enhance the blood supply to the pericranial flap.
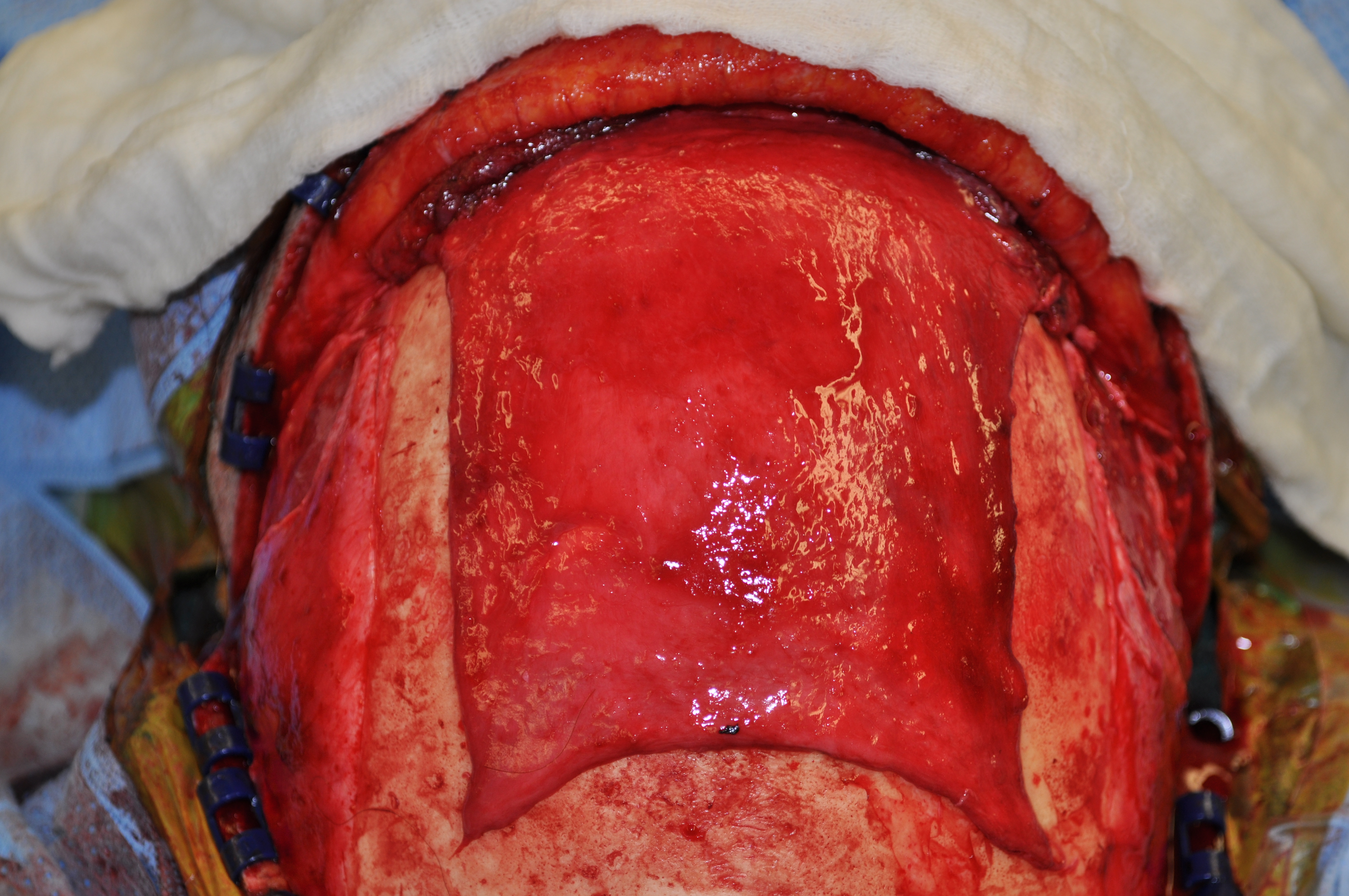
- Once the coronal flap is raised, the pericranial flap is elevated off of the calvarium down to approximately 1 cm above the supraorbital rims. Care must be taken not to disrupt the deep branches of the supraorbital and supratrochlear vessels.
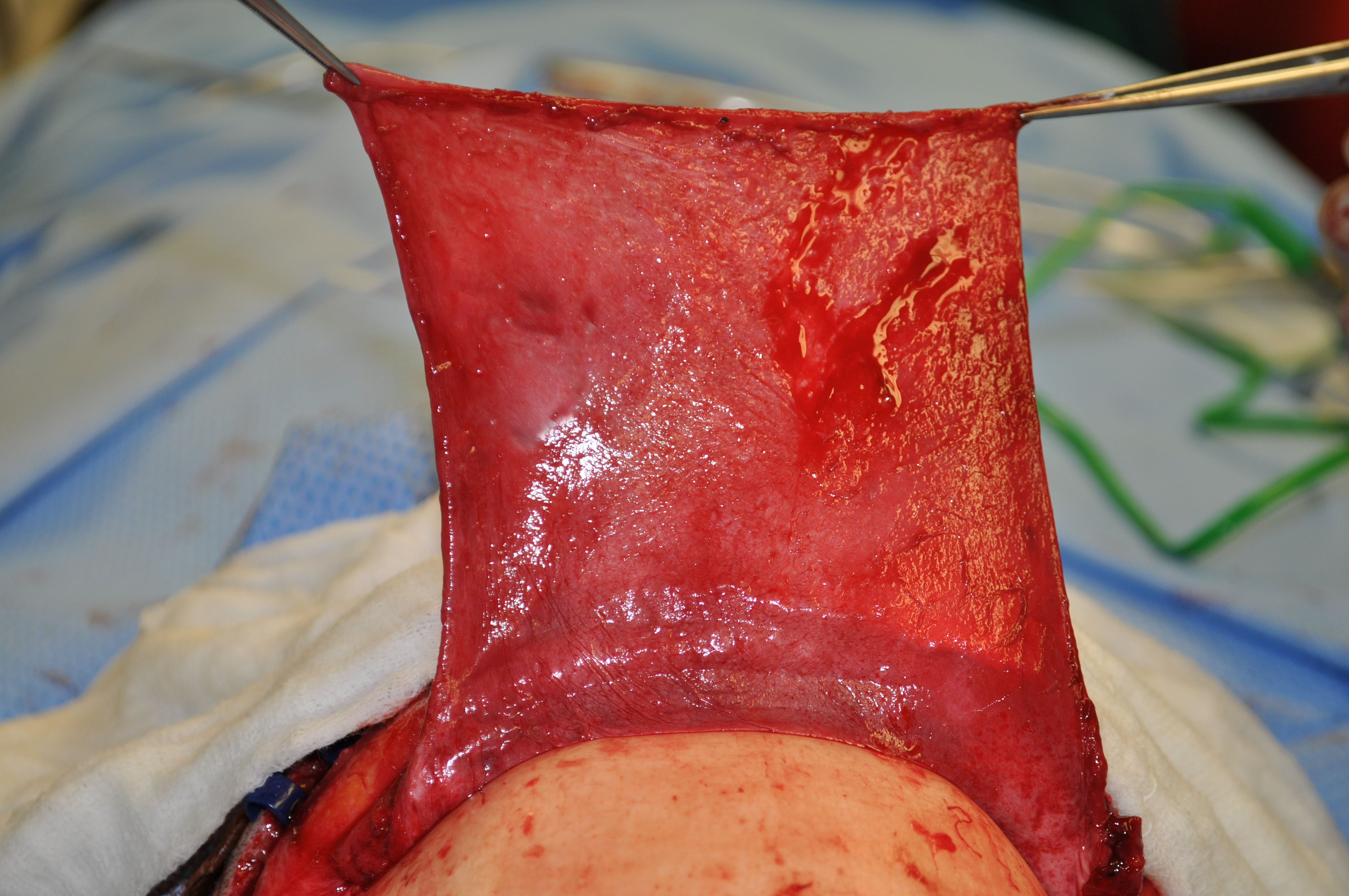
- The pericranial flap is reflected forward and covered with a wet lap sponge until it is needed.
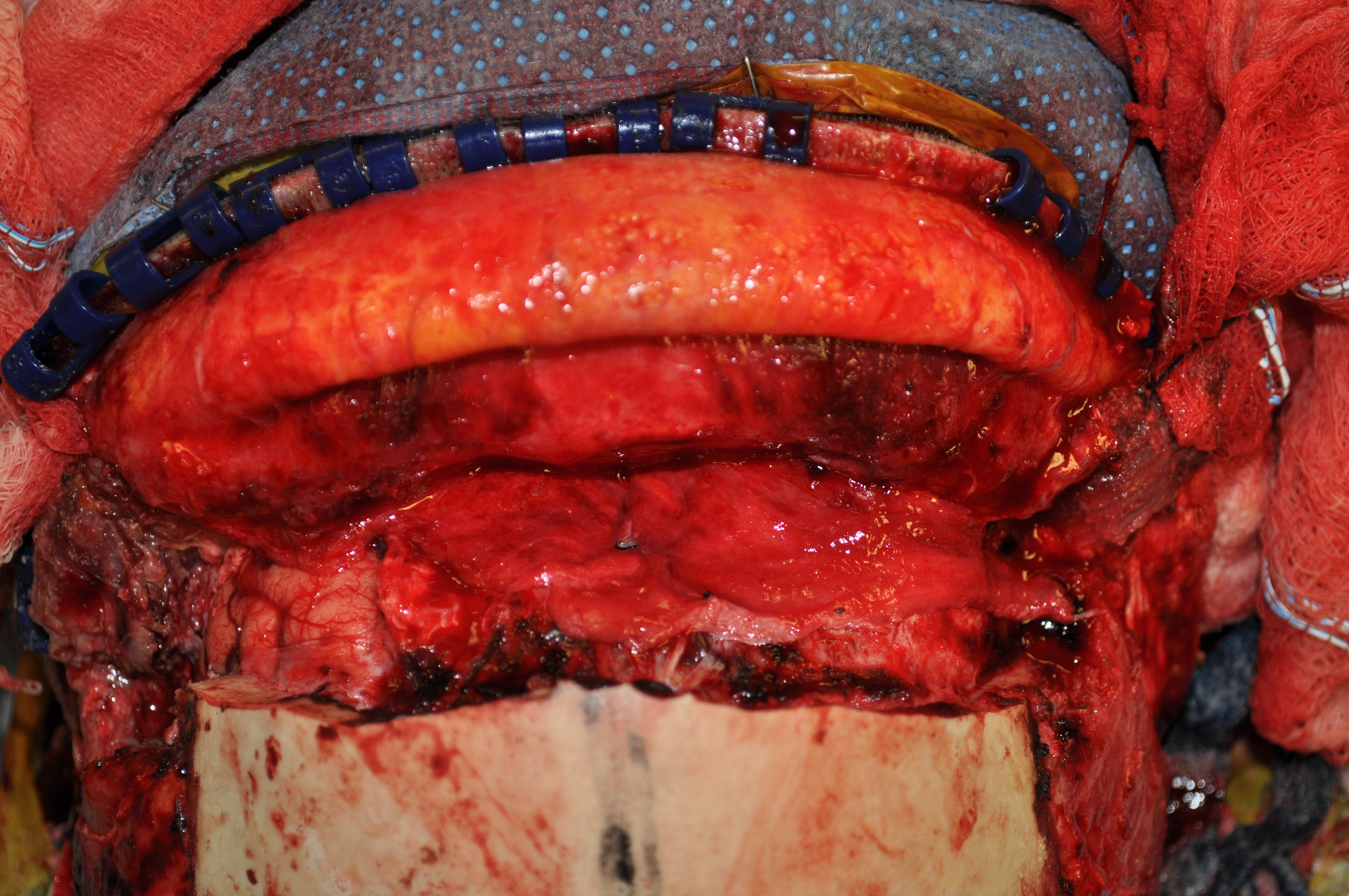
- When insetting the pericranial flap to reconstruct the anterior cranial floor, several tacking sutures may need to be placed through bone in the posterior bony defect to support the flap.
- When replacing the bone removed during the craniotomy, care must be taken that this does not compress the proximal end of the flap.
- The need for a skin graft to line the sinonasal side of the flap is debated. A well-vascularized flap will mucosalize rapidly, and the skin graft probably adds little to the overall viability and strength of the reconstruction. The pericranium with or without skin graft needs to be supported with nasal packing for approximately seven days.
ELEVATION OF THE PERICRANIAL-GALEOFRONTALIS FLAP
- This flap is less frequently used for major craniofacial skull base repair and is more commonly used if a smaller repair, such as vascular covering for nasal bone grafts, is required.
- Once the coronal incision is made, the coronal skin flap is elevated anteriorly in the plane just superficial to the galea in the area where the galea will be harvested. This plane is just deep to the subcutaneous tissue.
- The flap may extend inferiorly to include the upper aspect of the frontalis muscle. For very narrow midline flaps, the medial aspects of these muscles may be raised with the flap.
POSTOPERATIVE CARE
- Nasal packing may remain in place for six to seven days. The packing should be gently removed after this time.
- Patients remain on antibiotics until after the nasal packs are removed.
REFERENCES
Har-Shai Y, Fukuta K, Collares MV, et al. The vascular anatomy of the galeal flap in the interparietal and midline regions. Plast Reconst Surg. 1992;89:64-69.
Potparic Z, Fukuta K, Colen LB, Jackson IT, Carraway JH. Galeo-pericranial flaps in the forehead: a study of blood supply and volumes. Br J Plast Surg. 1990;49:519-528.
Price JC, Loury M, Carson B, Johns ME. The pericranial flap for reconstruction of anterior skull base defects. Laryngoscope. 1988; 98:1159-1164.
Scher RL, Cantrell RW. Anterior skull base reconstruction with the pericranial flap after craniofacial resection. ENT Journal. 1989;71:210-217.
Giurintano J, McDermott MW, El-Sayed IH. Vascularized Pericranial Flap for Endonasal Anterior Skull Base Reconstruction. J Neurol Surg B Skull Base. 2021 Feb 18;83(2):133-136. doi: 10.1055/s-0040-1721816. PMID: 35433180; PMCID: PMC9010135.