




return to: Salivary Gland Surgery Protocols
see: Case example Submandibular Gland Resection
see: Case Example Retained Submandibular Stone After Submandibular Gland Resection with neck fistula
GENERAL CONSIDERATIONS
- Indications
- Recurrent sialadenitis (infection) or obstructive sialodocholithiasis (salivary stones)
- Sialorrhea (drooling)
- Contraindication
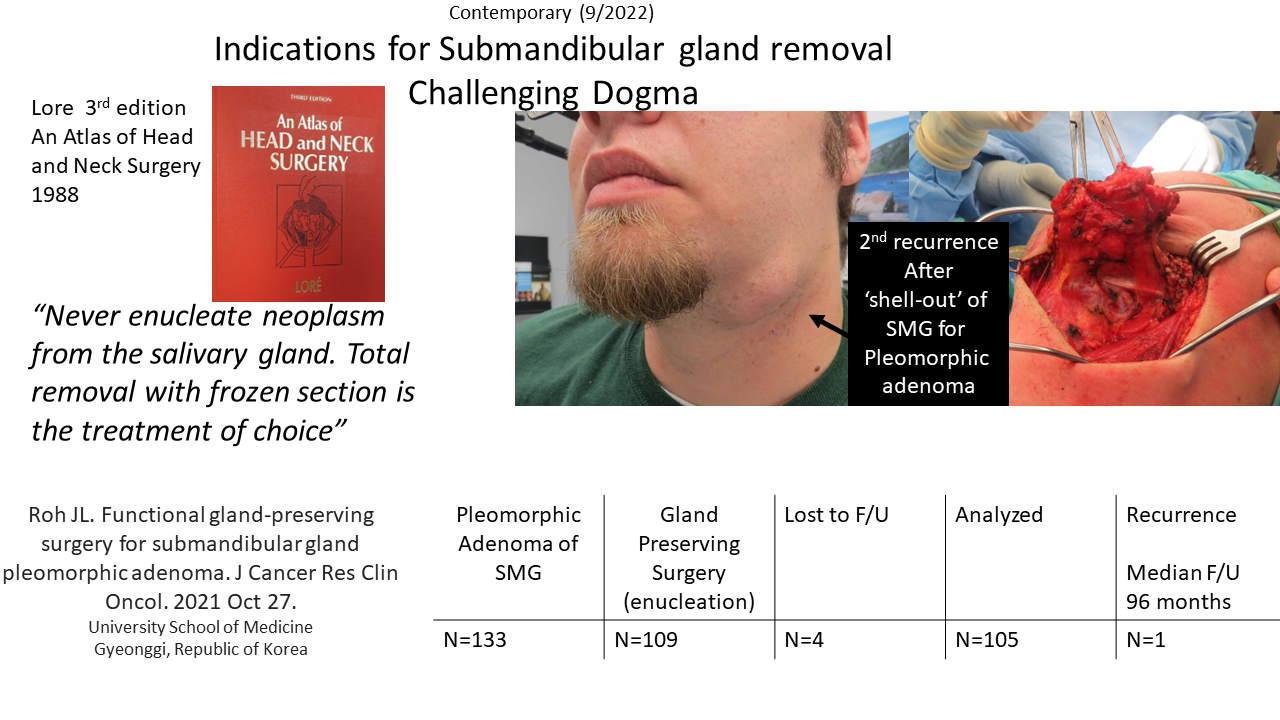
- Suspicion of tumor: As a general concept, a 'shell-out' removal of the gland should not be done as a "biopsy" to rule out tumor, whether benign or malignant. A formal "Level I neck dissection" rather than a "shell out" of the gland should be done unless the evaluation clearly points to a non-neoplastic indication for gland removal (see Selective Neck Dissection protocol). Fine needle aspiration biopsy and core needle biopsy are generally indicated before removing a gland for suspected tumor. If a 'shell-out' identifies a tumor - especially if margins are close, a formal level I neck dissection is advised to endeavor to improve the margins about the resection.
- Poor medical condition: For those few patients who are unable to tolerate general anesthesia, the gland has on rare occassion been removed under local anesthesia.
PREOPERATIVE PREPARATION
- Evaluation
- Consider CT (we generally get with contrast even when looking for stones - others have advocated doing it without contrast if looking for stones)
- Ultrasound with or without FNA
- May consider sialography.(see: Sialograms and Sialography)
- Unless clinical findings clearly indicate non-neoplastic process:
- Perform fine needle aspirate (FNA) biopsy
- CT or MRI
- Consent
- Describe procedure and incision.
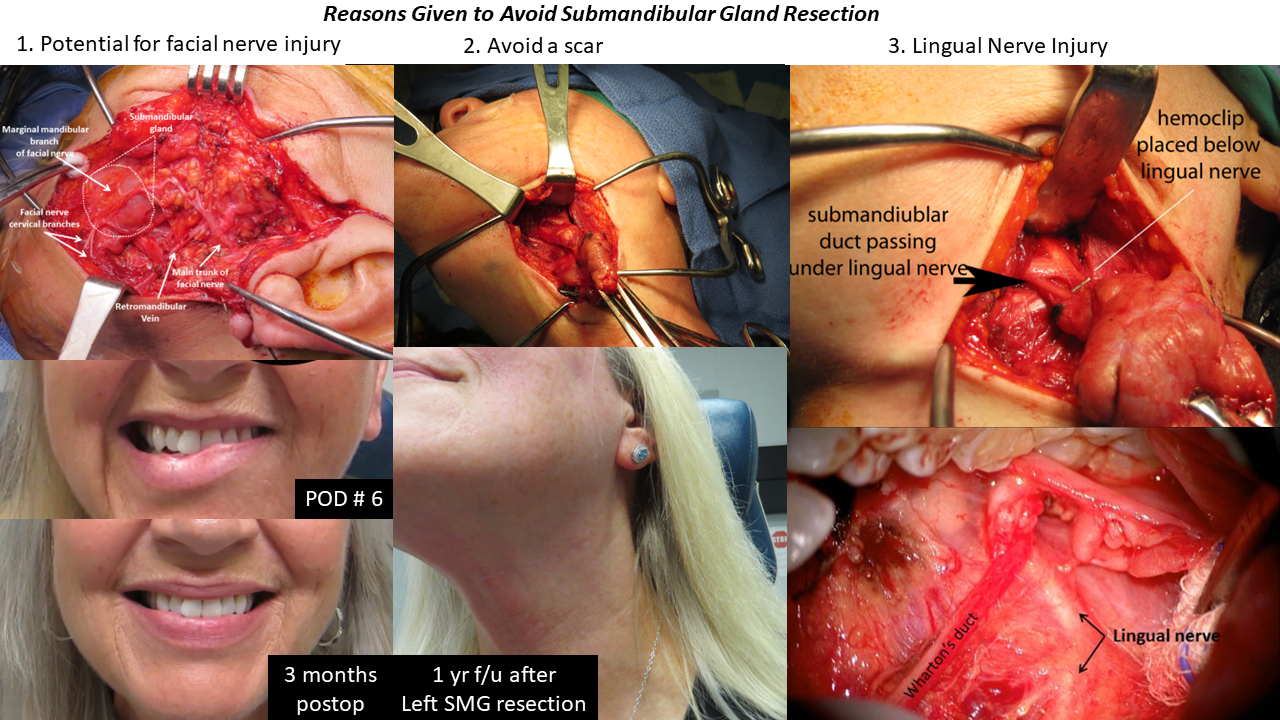
- Describe location of relationship of gland to marginal mandibular nerve, lingual nerve, and hypoglossal nerve.
- Describe Wharton's duct and its relationship to the floor of mouth, sublingual glands, lingual and hypoglossal nerves.
- Describe expected sequelae:
- Numbness about incision
- Potential for altered lower lip contour from transection of platysma muscle and cervical branch of facial nerve
- Describe complications:
- Bleeding, infection, reaction to anesthetic agents
- Damage to adjacent structures: marginal mandibular nerve, lingual nerve, hypoglossal nerve
- Retained stone in distal stump of Wharton's duct - and consider measures to avoid - see: Retrograde (actually Antegrade) Sialendoscopy to Prevent Retained Ductal Stone with Submandibular Gland Resection
NURSING CONSIDERATIONS
- Room Setup
- Instrumentation and Equipment
- Standard
- Special
- Varidyne vacuum suction controller
- Nerve stimulator control unit and instrument
- Consider use of sialendoscopes (sialendoscopy protocol) in a retrograde fashion to evaluate distal Wharton's duct for retained stone (selected cases)
- Medications (specific to nursing)
- Antibiotic ointment
- 1:100,000 epinephrine (no lidocaine)
- Prep and Drape
- Standard prep, 10% providone iodine
- Drape
- Head drape
- Drape with towels to expose neck and lower face including lips
- May consider (rarely performed, especially if access to the floor of mouth is needed or concurrent sialendoscopy to be done) appling incise drape (clear) and/or 1010 drape to isolate contaminated oral cavity from the surgical field
- Split sheet
- Drains and Dressings
- Varidyne vacuum suction drain (7 mm or 10 mm) or Penrose drain
- Antibiotic ointment to suture line
ANESTHETIC CONSIDERATIONS
- Preoperative Systemic Medications
- Antibiotics as soon as IV started (see Antibiotic protocol) - cases with active infection are generally best put off until infection controlled - may have on a prolonged course of antibiotics before surgery, sometimes supplemented by steroids for several days before surgery
- Ensure patient is not paralyzed (to permit use of a facial nerve stimulator) 'fully relaxed' is a description than 'paralyzed' to use of anesthetic is discussed with the patient listening
- Position
- Oral endotracheal intubation with tube secured to contralateral corner of mouth
- Table turned just past 180° with surgeons located on either side of the head
- Head of bed elevated to diminish bleeding
OPERATIVE PROCEDURE
- Incision and Flap Elevation
- Along the relaxed skin tension lines, a horizontal incision is made at least 2 fingerbreadths below the mandible to ensure the marginal mandibular nerve is not damaged. Note variability in level of marginal mandibular nerve warrants use of never stimulator to determine the level at which the platysma is transected (below level of nerve)
- Incision through dermis permits secondary dissection with hemostat or kelly above platysma to go through subutaneous fat to expose platysma - facilitated by use of two Gelpi retractors
- Carry the incision down through the platysma to expose the anterior border of the sternocleidomastoid muscle posteriorly and the anterior belly of the digastric muscle.
- The posterior inferior aspect of the submandibular gland is identified immediately anterior to the sternocleidomastoid muscle where it overlays the posterior belly of the digastric muscle.
- A primary goal of flap elevation is to expose the submandibular gland without damaging the marginal mandibular nerve.
- Marginal Mandibular Nerve Preservation
- The marginal mandibular nerve may be preserved without identifying it by:
- Elevation of the fascia of the submandibular gland from an inferior to superior direction that carries the marginal mandibular nerve superiorly away from the gland.
- Elevation of the posterior facial vein will draw the marginal mandibular nerve superiorly away from the gland.
- The marginal mandibular nerve may be identified, dissected, and elevated separately superiorly above the mandible.
- This maneuver is used for a comprehensive Level I dissection to permit full removal of the contents of Level I including the prevascular and postvascular nodes around the facial artery as it courses over the mandible.
- Use of the nerve stimulator (Parson's McCabe) or Checkpoint nerve stimulator facilitates identification of the marginal mandibular nerve through stimulation or contraction of the depressors to the ipsilateral lower lip.
- Direct identification of the marginal mandibular nerve without the nerve stimulator may be effected by knowledge of its relationship to adjacent landmarks:
- The nerve overlies the posterior facial vein.
- The nerve underlies the platysma and overlies the submandibular gland.
- The cervical nerve branches to platysma are continuous with the marginal mandibular nerve and can be dissected proximally to encounter the nerve.
- The marginal mandibular nerve may be preserved without identifying it by:
- Gland Removal
- Following flap elevation, the gland is exposed and retracted inferiorly, employing an Allis clamp or Babcock for traction.
- The digastric muscle is identified along its course including the common tendon and the anterior belly.
- The anterior aspect of the gland is mobilized posteriorly to expose the mylohyoid muscle.
- An Army-Navy retractor is placed under the posterior border of the mylohyoid muscle to retract anterosuperior to expose the lingual nerve.
- Bipolar cautery, medium-sized hemoclips, or suture ligature is placed to the submandibular ganglion permitting separation of the gland from the lingual nerve.
- The duct of the gland is traced anteriorly and transected after placement of a hemoclip as distal as possible. Retention of a segment of Wharton's duct may predispose to infection resulting from retained stone or debris in the duct. To decrease the risk of stone retention in the Wharton's duct remnant either sialendoscopy confirming a clear duct at the beginning of the procedure or retrograde sialoendoscopy may be performed after gland removal (see: Case Example 2 Retrograde Sialendoscopy to Prevent Retained Ductal Stone with Submandibular Gland Resection and Case Example of Submandibular Gland Resection with Sialendoscopy to Avoid Retained Stone in Duct Remnant).
- The gland is dissected posteriorly to encounter branches (usually 3) from the facial artery perfusing the gland.
- The facial artery may be left intact with suture ligature of the multiple branches to the gland from the facial artery (see: Case example Submandibular Gland Resection) permitting removal of the gland from the wound.
- Alternatively, the facial artery may be suture ligated below the gland (after passing under the digastric muscle) and above the gland (before passing over the mandible).
- The hypoglossal nerve is not routinely displayed.
- Completion of Procedure
- Frozen section analysis may be used to rule out the presence of tumor and will permit a more comprehensive Level I dissection if an unexpected tumor is identified.
- The wound is irrigated with saline and closed in layers over a drain.
- 3-0 or 4-0 vicryl or chromic subcutaneous
- 5-0 nylon to skin of the neck
- Drains
- Penrose drain may be placed, a light wrap around pressure dressing is applied (burn netting).
- A closed suction #7 or #10 flat, Jackson-Pratt fully perforated drain may alternatively be placed with no dressing other than antibiotic ointment is applied.
- Choice of drains based on findings at surgery: if infection present, use passive (penrose drain); if no infection and no communication intra-orally, may alternatively use closed suction drain.
POSTOPERATIVE CARE
- Suction Drain Management versus passive penrose drain
- The suction drain is left in for 36 hours minimum (longer depending on output) see: Closed Suction Drain Management
- General rule: Remove drain only after three consecutive 8-hour shifts demonstrate a 24 hours cumulative output less than 30 cc.
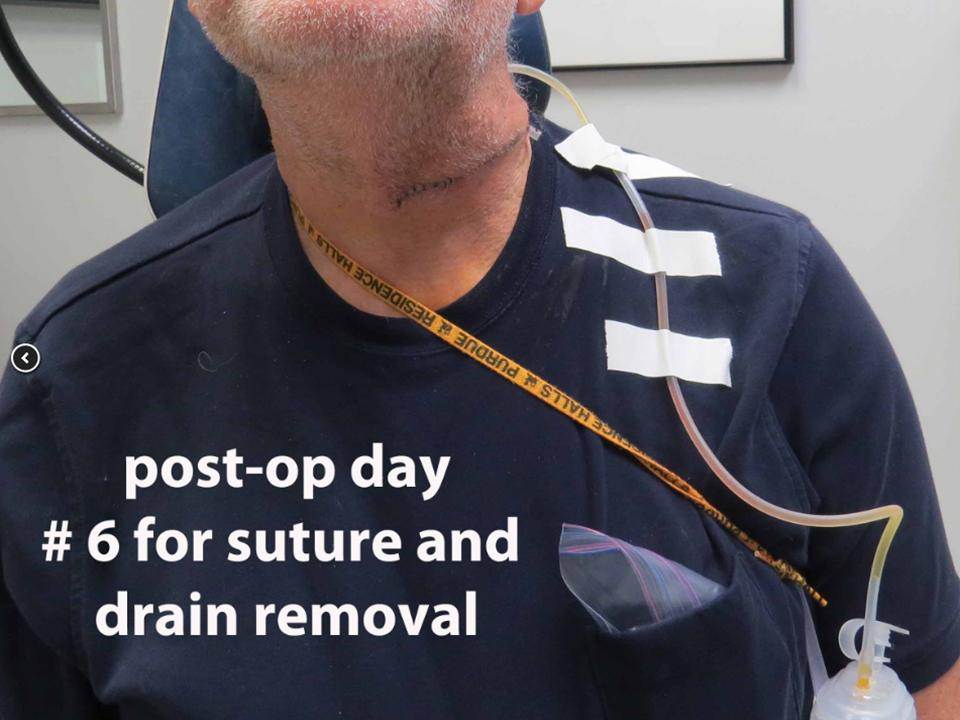
- The drain may be managed in an outpatient setting - especially in case of infection may leave passive penrose drain in until sutures are removed (POD #6; alternatively can remove POD #3 or 4)
- Most commonly currently using passive penrose drain (especially if gland is inflamed/infected)
- Antibiotics (see Antibiotic protocol)
- Suture removal on postoperative day 6 - usually done along with drain removal at that time.
SAMPLE DICTATION
The patient was brought to the operating room and placed on the operating table in supine position. Transorally intubated. An 4cm line extending anteriorly from the from the anterior border of the sternocleidomastoid muscle and parallel to the mandible was marked at 2 fingerbreadths below the angle of mandible in a pre-existing skin crease. Epinephrine 1:100,000 was injected in the incision line in the left upper neck and the area prepped with Betadine and draped in sterile fashion. The face was exposed to permit monitoring with facial nerve stimulator during the resection. The skin incision was extended through the platysma with frequent use of the facial nerve stimulator to ensure the plastysma incision was well below the marginal mandibular nerve. The inferior boder of the submandibular gland was identified with blunt dissection. The fascia of the submandibular gland was elevated off of the gland from inferior to superior to lift the fascia so that the marginal branch of the facial nerve was elevated off the gland with the fascia and protected as the overlying platysma was elevated with this flap (without separate elevation of platysma). The facial artery was identified with the three small branches to the gland ligated with 4-0 silk preserving the facial artery (note: alternatively may ligate the facial artery). The gland was dissected off the mylohyoid muscle which was then retracted anteriorly allowing identification of the lingual nerve. The gland was dissected away from the lingual nerve and Wharton's duct with a clip placed toward the distal end of Wharton's duct under the lingual nerve. The specimen was then delivered from the operative field and sent to pathology. The gland appeared inflamed but was otherwise without any appreciable abnormalities. The surgical site was copiously irrigated with sterile saline and hemostasis obtained with bipolar cautery. The incision was closed over a 1/4-inch Penrose drain using deep 3-0 Vicryl stitches to reapproximate the platysma and a running 4-0 nylon in skin. The patient was then turned over to the care of the anesthesiology team, extubated uneventfully in the operating room and transferred to the post-anesthesia care unit.
REFERENCES
Hoffman H, Funk G, Endres G. Evaluation and surgical treatment of tumors of the salivary glands. In: Themley SE, Ponje WR, Botskis JG, Lindberg RD, eds. Comprehensive Management of Head and Neck Tumors. 2nd ed. Philadelphia, Pa: WB Saunders, 1999.